Article Text

Abstract
Metastatic colorectal cancers (mCRC) harboring microsatellite instability (MSI) are sensitive to immune checkpoint inhibitors (ICIs), but the mechanisms of resistance to ICIs remain unclear. Dissociated responses in patients with ICI-treated cancer suggest that certain organs may serve as sanctuary sites due to the tumor microenvironment. This case series describes five patients with ICI-treated MSI mCRC with disease progression limited to the adrenal glands. At ICI initiation, three patients were free of metastasis in the adrenal glands. Four patients experienced objective response per RECIST (Response Evaluation Criteria in Solid Tumors) while treated with ICI. ICI treatment was discontinued due to progressive disease limited to the adrenal glands (n=3) or toxicity (n=2). The time between ICI initiation and progression in the adrenal glands ranged from 11 to 39 months. Adrenalectomy (n=3) and stereotactic body radiation therapy (n=2) were performed. At the last follow-up, all patients were alive and progression free. Molecular analyses were performed in one patient. A significant impairment of the antigen presentation pathway was observed in the ICI-resistant lesion of the adrenal gland, which could be explained by the presence of glucocorticoids in the adrenal gland microenvironment. We also detected an overexpression of TSC22D3, a glucocorticoid-target gene that functions as a mediator of anti-inflammation and immunosuppression. This case series suggests that the adrenal glands may be the sanctuary sites for ICI-treated MSI mCRC through the glucocorticoid-induced impairment of the antigen presentation machinery.
- gastrointestinal neoplasms
- biomarkers
- tumor
- genome Instability
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Microsatellite instability (MSI) is a tumor phenotype resulting from a deficient mismatch repair system (dMMR). It is observed in approximately 5% of patients with metastatic colorectal cancers (mCRC). Immune checkpoint inhibitors (ICIs) have changed the treatment of patients with MSI/dMMR mCRC, with an objective response (OR) rate ranging from 30% to 60% and a 1-year overall survival rate ranging from 72% to 85% in heavily pretreated patients.1 Recently, first-line pembrolizumab has been associated with clinically meaningful and statistically significant improvement of progression-free survival compared with standard of care chemotherapy with or without bevacizumab or cetuximab.2 However, up to 50% of patients with MSI/dMMR mCRC exhibit primary resistance to ICIs. Besides, 5%–25% of responders might develop acquired resistance to these treatments, knowing this estimation might increase with longer follow-up.1 Mechanisms underlying de novo and acquired resistance to ICIs in MSI/dMMR cancer are barely known. Besides, dissociated responses have been reported in approximately 8% of patients with metastatic solid tumors treated with ICIs, suggesting potential site-specific patterns of response.3 4 MSI/dMMR mCRC are associated with a specific metastatic pattern, reflected in high rates of peritoneal carcinomatosis and distant lymph node metastasis. Contrarily, adrenal glands metastases are rarely found in mCRC.
Here we report a case series of five patients with MSI/dMMR mCRC treated with ICI who experienced progression of adrenal gland metastases despite OR or disease stability of other metastatic sites, suggesting potential site-specific resistance to ICI. Translational analyses were performed for one patient, seeking for potential site-specific mechanisms of resistance.
Results
The five patients of this case series represent 2.5% of the entire population of patients with ICI-treated MSI/dMMR in our institutions. Table 1 summarizes the disease history of these five ICI-treated mCRC cases. The age of patients ranged from 44 to 77 years. Three patients had germline MMR gene mutation. Two patients had an adrenal gland metastasis at the ICI initiation. Other metastatic sites were distant lymph nodes (4/5), liver (3/5), peritoneum and lung (1/5). Four patients were treated with a combination of an anti-PD1 monoclonal antibody and an anti-CTLA4 antibody, one received an anti-PD1 alone. Four patients experienced OR, with three partial responses and one complete response. Reasons of treatment discontinuation were progression limited to the adrenal glands (n=3) and toxicity (n=2). All five patients experienced a significant disease progression limited to the adrenal gland, with three of them being newly defined target lesions (online supplemental figure S1). The time from ICI initiation to the date of disease progression in the adrenal gland ranged from 11 to 39 months. The progressive adrenal metastases were treated with adrenalectomy (n=3) or stereotactic body radiation therapy (n=2). No other systemic anticancer treatments was initiated. At the last follow-up visit (the time from local treatment date to the last patient visit: 3–47 months), all patients were alive and free of progression.
Supplemental material
Patient clinical characteristics
Tumor tissue samples from patient #1 were investigated to identify the potential resistance mechanisms. Paired tumor-normal tissue samples from the progressive adrenal gland, the primary tumor, and liver metastasis resected before ICI initiation were analyzed using whole-exome sequencing and RNA sequencing (Supplementary methods). All three metastatic disease sites displayed the hypermutator phenotype (online supplemental figure S2A and S3) in repetitive (43.9, 43.9, 51.7 mutations/Mb) and non-repetitive DNA sequences (29.1, 27.5, 32.0 mutations/M for the colon, liver, and adrenal tumors, respectively). All sites exhibited an MSI phenotype (online supplemental figure S2B; 34.5, 32.4, 37.0) MSIsensor score for the colon, liver and adrenal tumors, respectively).
Supplemental material
Supplemental material
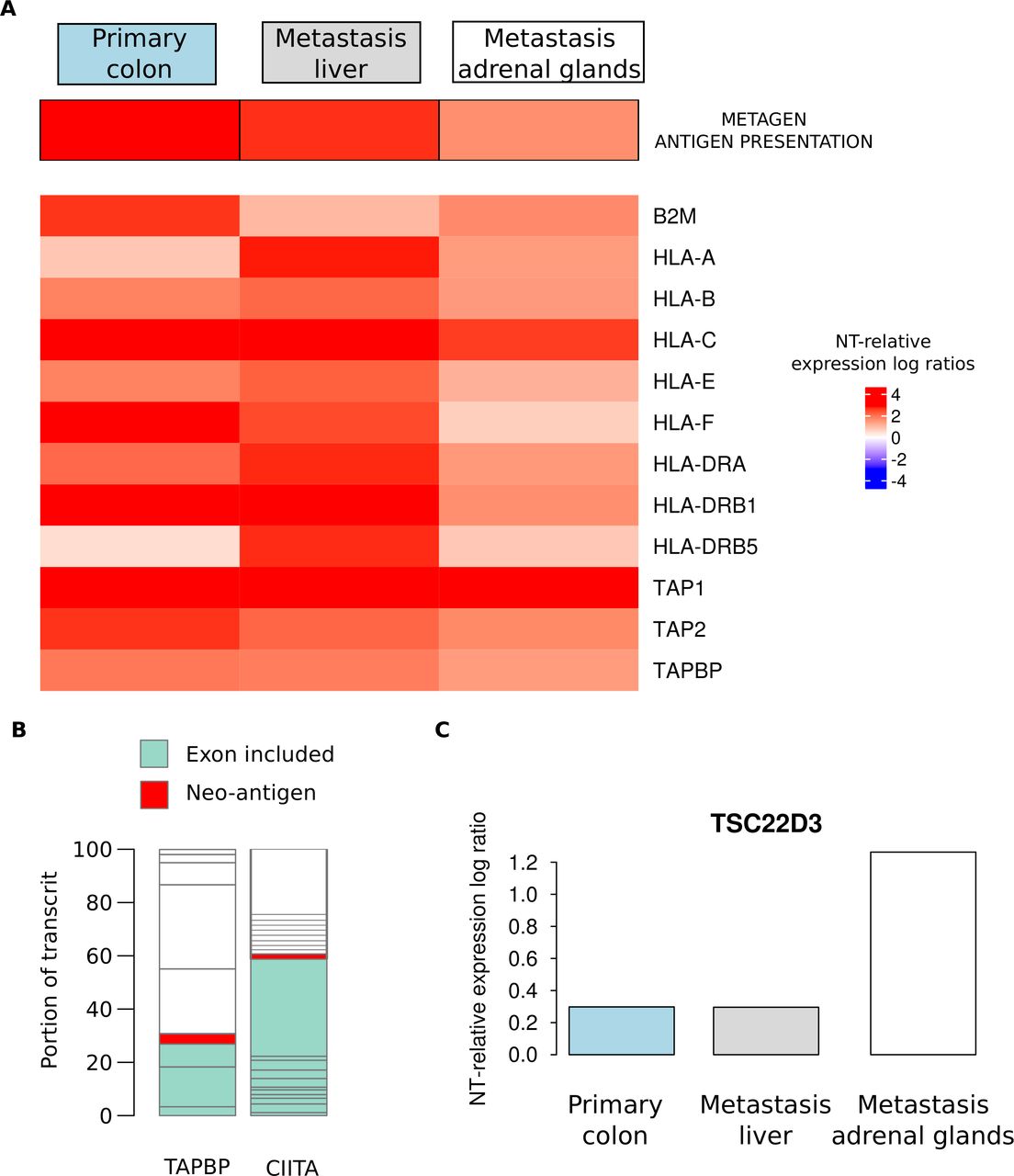
We hypothesized that adrenal tumors could decrease their antigen presentation, leading to immune escape. For the majority of the antigen presenting genes (HLA-B, HLA-C, HLA-E, HLA-F, HLA-DRA, HLA-DRB1, TAP1, TAP2, TAPBP) a decrease expression in the adrenal tumor was observed (figure 1A). This loss of expression might be related to the presence of glucocorticoids, which inhibit NF-κB gene, controling the HLA-class I expression (online supplemental figure S4). This might be also explained by adrenal-specific mutation(s) in antigen presentation pathway. In line, we identified two candidate’s mutations, namely TAPBP and CIITA (figure 1B), which are essential for the signaling pathway (online supplemental figure S4). We also detected an overexpression of TSC22D3 (figure 1C), a glucocorticoid-target gene, which functions as a mediator of anti-inflammation and immunosuppression and has been shown to abolish the therapeutic benefit of PD-1 blockade in mouse models of cancers.5 Our analysis of the tumor microenvironment using Microenvironment Cell Populations-counter (MCP-counter did not show significant differences in cell populations according to the tumor site. There were no significant differences for expressions of gene (PDCD1, PDCD1LG2, CTLA4, and HAVCR2) encoding for checkpoint proteins (PD1, PDL2, CTLA4, and TIM3, respectively; data not shown).
Supplemental material

{kind=link}
Potential resistance mechanism. The heatmap shows the percentage of nucleotide (NT) relative expression ratios at three tumor sites for key genes from the antigen presentation pathway. (A) Biological consequence of two microsatellite mutations on two key genes of the antigen presentation pathway. (B) Box plot represents NT relative expression ratio across tumor sites for TSC22D3 gene (C).
Discussion
We report here a case series of five patients with MSI/dMMR mCRC who experienced disease progression limited to the adrenal gland while on ICIs. To our knowledge, this is the first report suggesting the site-specific resistance to ICIs of MSI/dMMR tumors. Molecular analysis of one patient showed a significant decrease of expression of the antigen presentation pathway genes in the ICI-resistant adrenal gland.
The concept of the sanctuary sites, such as the brain, ovary, or testis is well known in the context of cytotoxic chemotherapy. In the era of immunotherapy it is supported by the existence of dissociated tumor responses.4 Besides, retrospective studies suggest that the sensitivity to ICIs may depend on the metastatic site, with lung lesions being more likely to achieve OR than other sites such as liver metastases.6 The differential responses to treatment observed according to the site of metastasis suggest that the tumor microenvironment is involved in the intrapatient heterogeneity of tumor response.
Few clinical case reports of ICI-treated solid tumors and surgical series of patients with melanoma suggest that adrenal glands might be a sanctuary for tumor cells.7 No warning signal has been reported for patients with lung cancer, though.3 Our case series with five tumor progressions limited to the adrenal glands in patients with MSI/dMMR mCRC is striking since CRC involving adrenal glands is uncommon. The fact that these cases had no PD in other metastatic sites after local treatment (surgery or stereotactic body radiation therapy) supports the use of local therapies in case of progression limited to the adrenal glands. One unresolved question is whether ICI should be maintained beyond progression limited to a sanctuary site.
The systemic administration of synthetic glucocorticoids such as dexamethasone and prednisolone has been associated with poorer outcomes in patients with ICI-treated cancer.8 It has been shown that both synthetic and endogenous glucocorticoids can inhibit anticancer immune response through an impairment of the antigen presentation by dendritic cells or the activation of T-cells.9 Given that endogenous glucocorticoids is produced by the adrenal glands, one might hypothesize the adrenal gland microenvironment might be immunosuppressive and acts as a sanctuary site for ICI-treated neoplasms tumor cells.
From the molecular data of one analyzed patient, we conclude that the mechanism underlying the acquired resistance of the tumor to ICI was not related to a loss of the MSI phenotype. All tumor samples of this single patient (the primary colon tumor, liver metastasis, and refractory adrenal gland lesion) presented an MSI phenotype associated with high mutation burden. A defect in the antigen presentation processing was likely to be involved and we hypothesize therefore that this may act synergistically with local immunosuppression for the adrenal gland metastasis resistance in this patient. This hypothesis is strengthened by the work of Yang et al 5 who showed in mouse models that TSC22D3 abolishes the therapeutic effect of PD-1 blockade. Since an antigen presentation is known as a mechanism of acquired resistance to ICIs,10 we hypothesize that the adrenal gland might be a sanctuary of ICI-treated cancer through the glucocorticoid-induced impairment of the antigen presentation machinery.
We acknowledge some limitations of our work. Only one patient has his tumor samples analyzed with the adrenal gland sample collected at the time of disease progression when on ICI and the primary tumor and the liver metastasis samples before the ICI initiation. Another limitation was the lack a control group to evaluate the relationship between dissociated tumor responses and the adrenal gland involvement. Therefore, the interpretation of our results, which deserve confirmation in larger studies, should be interpreted with caution. Molecular investigations of ICI-resistant MSI/dMMR mCRC metastases (from adrenal glands and other sites) are urgently needed to decipher microenvironment-related mechanisms of resistance to ICI and, eventually, identify other sanctuary sites.
In conclusion, our case series highlights the importance of giving attention to the adrenal glands in patients treated with ICIs for MSI/dMMR mCRC.
Supplemental material
Acknowledgments
The authors thank Magdalena Benetkiewicz, Sc.D, for editorial assistance.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RC and VJ contributed equally.
Contributors Data collection: RC, CDLF, MS, TA. Translational analysis: VJ, TR, QL, MA, LA, AD. Data interpretation: RC, VJ, CDLF, TR, QL, MA, LA, AB, MS, AP, RC, FP, PM, MS, AD, TA. Manuscript drafting: RC, VJ, AD, TA. Manuscript reviewing: RC, VJ, CDLF, TR, QL, MA, LA, AB, MS, AP, RC, FP, PM, MS, AD, TA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Dr André reports consulting/advisory role and or received honoraria from Amgen, Bristol-Myers Squibb, Chugai, Clovis, GlaxoSmithKline, Gristone oncology, HalioDx, MSD Oncology, Pierre Fabre, Roche/Ventana, Sanofi, Servier and Tesaro and has received travel, accommodations, and expenses from Roche/Genentech, MSD Oncology, and Bristol-Myers Squibb. Dr Cohen reports honoraria from MSD Oncology, and research grant from Servier Institute. Dr Pellat reports honoraria from Servier and travel fees from Ipsen. Dr Svrcek reports consulting/advisory role and or received honoraria from Bristol-Myers Squibb, Astellas, MSD Oncology, Sanofi, and has received travel, accommodations, and expenses from Bristol-Myers Squibb and Ventana/Roche. The other authors did not report any conflict of interest.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.