Article Text

Abstract
Background Programmed cell death protein 1 (PD-1) pathway blockade with immune checkpoint inhibitors (ICIs) is a standard therapy in advanced hepatocellular carcinoma (HCC) nowadays. No strategies to overcome ICI resistance have been described. We aimed to evaluate the use of ipilimumab and anti-PD-1 ICIs (nivolumab or pembrolizumab) combinations in patients with advanced HCC with progression on prior ICIs.
Methods Patients with advanced HCC with documented tumor progression on prior ICIs and subsequently received ipilimumab with nivolumab/pembrolizumab were analyzed. Objective response rate (ORR), median duration of response (DOR), time-to-progression (TTP), overall survival (OS), and treatment-related adverse events (TRAEs) were assessed.
Results Twenty-five patients were included. The median age was 62 (range: 51–83). About 68% were of Child-Pugh (CP) Grade A and 48% had primary resistance to prior ICI. At median follow-up of 37.7 months, the ORR was 16% with a median DOR of 11.5 months (range: 2.76–30.3). Three patients achieved complete response. The median TTP was 2.96 months (95% CI: 1.61 to 4.31). Median OS was 10.9 months (95% CI: 3.99 to 17.8) and the 1 year, 2 year and 3 year survival rates were 42.4%, 32.3% and 21.6%, respectively. The ORR was 16.7% in primary resistance group and 15.4% in acquired resistance group (p=1.00). All responders were of CP A and Albumin-Bilirubin (ALBI) Grade 1 or 2. CP and ALBI Grades were significantly associated with OS (p=0.006 and p<0.001, respectively). Overall, 52% of patients experienced TRAEs and 12% experienced Grade 3 or above TRAEs.
Conclusions Ipilimumab and nivolumab/pembrolizumab can achieve durable antitumor activity and encouraging survival outcomes with acceptable toxicity in patients with advanced HCC who had prior treatment with ICIs.
- liver neoplasms
- programmed cell death 1 receptor
- CTLA-4 antigen
- drug therapy
- combination
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Liver cancer is the fourth leading cause of cancer death worldwide, with the majority (75%–85%) being hepatocellular carcinoma (HCC).1 HCC often arises from a microenvironment characterized by chronic inflammation, intrinsic immunosuppression and overexpression of immune checkpoints including the programmed cell death protein 1 (PD-1) pathway and programmed death ligand 1 (PDL-1), and the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) pathway. This results in reduction of proliferation, inhibition of activation and functional exhaustion of T cells leading to tumor immune escape. Targeting these characteristics, immune checkpoint inhibitors (ICIs) have significantly advanced the systemic treatment of inoperable, advanced HCC. Nivolumab, an anti-PD-1 antibody, demonstrated good efficacy and safety as second-line treatment for advanced HCC in the CheckMate-040 trial.2 Nivolumab as first-line treatment for advanced HCC also demonstrated clinical benefits when compared with sorafenib in the CheckMate-459 trial, although statistical significance was not obtained.3 In addition, pembrolizumab received accelerated regulatory approval for second-line treatment of advanced HCC based on the Keynote-224 trial.4 Nevertheless, in the subsequent Keynote-240 trial, both the median progression-free survival (PFS) and overall survival (OS) of pembrolizumab did not reach statistical significance per specified criteria.5 Recently, atezolizumab (an anti-PD-L1-antibody) in combination with bevacizumab was approved for first-line treatment of advanced HCC based on results from the IMbrave150 trial, which demonstrated an impressive objective response rate (ORR) of 27.3%, median PFS of 6.8 months and OS at 12 months of 67.2%, all superior to the sorafenib arm.6 Based on these emerging data, ICIs will be increasingly used in both first-line and second-line settings for the treatment of patients with advanced HCC. Importantly, the majority of patients treated with ICIs will either never respond (primary resistance) or eventually develop resistance (acquired resistance). Hence, there is an unmet need to investigate the appropriate treatment for the rapidly expanding group of patients with advanced HCC who had tumor progression on prior anti-PD-1/L1 therapies.
To improve the therapeutic efficacy of ICIs, anti-CTLA-4 and anti-PD-1/L-1 are increasingly used simultaneously, with the combination of ipilimumab (an anti-CTLA-4 antibody) and nivolumab having received Food and Drug Administration approval in various cancer types. In patients with advanced HCC previously treated with sorafenib, ipilimumab–nivolumab has also received regulatory approval based on the promising results of the CheckMate-040 cohort 4 trial which reported an ORR of up to 32% and a median OS of up to 23 months.7 Recently, durvalumab (an anti-PDL-1 antibody) in combination with tremelimumab (an anti-CTLA-4 antibody) reported an ORR of up to 22.7% and a median OS of up to 18.7 months in population with advanced HCC.8 Interestingly, in advanced melanoma, non-small-cell lung cancer and metastatic renal cell carcinoma, salvage ipilimumab and nivolumab have lately demonstrated promising anti-tumor activities in patients with prior PD-1 pathway blockade.9–12
To evaluate the efficacy and safety of combined CTLA-4 and PD-1 blockade in patients with advanced HCC who failed PD-1 pathway blockade, we conducted an analysis of patients who received a combination of ipilimumab and nivolumab/pembrolizumab after tumor progression on prior anti-PD-1/L-1.
Methods
This was a single-center retrospective analysis approved by The University of Hong Kong/Hospital Authority Hong Kong West Cluster Institutional Review Board. Patients were identified from a prospectively maintained HCC database at Queen Mary Hospital, Hong Kong. Between June 2016 and February 2020, consecutive patients with HCC who were ineligible for surgical or locoregional therapies and had documented tumor progression on anti-PD-1/L-1 were included for analysis. All included patients received at least one dose of a combination of ipilimumab and nivolumab/pembrolizumab. Patients who received any other concomitant anticancer therapy were excluded.
HCCs were diagnosed either by histological confirmation, or according to the European Association for the Study of the Liver combined criteria if both characteristic radiological findings and an elevated serum alpha-fetoprotein level were present. Fine-needle cytology or biopsy was used for histological confirmation in cases of diagnostic uncertainty. Tumors were staged according to the Barcelona Clinic Liver Cancer system by CT scan or by MRI. Clinical, radiological and laboratory information were gathered from the database.
Treatment schedule, disease evaluation and follow-up
All patients received ipilimumab 1 mg/kg with nivolumab 3 mg/kg or pembrolizumab 2 mg/kg scheduled every 3 weeks. In general, four induction doses of ipilimumab and nivolumab/pembrolizumab followed by 1 year of maintenance nivolumab/pembrolizumab were scheduled. In selected cases, ipilimumab and nivolumab/pembrolizumab was administrated beyond four cycles at the discretion of treating clinicians. Radiological investigations were evaluated by investigators according to the Response evaluation criteria in solid tumors V.1.1 (RECIST 1.1) and the modified RECIST 1.1 for immune-based therapeutics (iRECIST).13 14 Best objective response (BOR) was defined as the best response per RECIST V.1.1 compared with baseline. ORR was defined as the percentage of patients with complete response (CR) or partial response (PR) according to RECIST 1.1. Patients who achieved CR, PR or stable disease (SD) were defined as achieving clinical benefits. Radiological reassessments of tumor response were scheduled every 8 to 12 weeks after treatment initiation. Primary resistance was defined as always having progressive disease on prior ICI, while acquired resistance was defined as ever having radiological CR, PR or SD with prior ICI. Treatment-related adverse events (TRAEs) were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events (V.4.0).15 All patients’ records were reviewed up to the end of their follow-up periods or study cut-off to observe for delayed TRAEs. TRAE-related ICI discontinuation or delay and systemic immunosuppressive treatments were recorded. All patients were followed up with regular clinical examinations, blood tests and scanning until death or last follow-up.
Statistical analysis
All statistical analyses were performed using SPSS (V.26, IBM, New York, USA). Duration of response (DOR) was calculated from the earliest date of CR or PR to progressive disease or last follow-up if no progression. Follow-up time was calculated from the date of first dose to death or last clinic follow-up. Time-to-progression (TTP) was calculated from the date of first dose to radiological progression, or censored at date of death or last follow-up while on treatment for patients without progression. OS was calculated from the date of first dose to death of any cause or censored at last follow-up for patients who were still alive at study cut-off. Median TTP, median OS and survival rates were estimated by Kaplan-Meier analyses and survival curves were compared using log-rank tests. Median follow-up was estimated by Reverse Kaplan-Meier analysis using follow-up time. Categorical variables were compared using Pearson’s χ2 test or Fisher’s exact test. A p value of 0.05 was used as the cut-off for statistical significance.
Results
Demographics
Twenty-five patients were included in the analysis. Table 1 shows their baseline characteristics. The median age was 62 (range 51–83). The majority of patients were of Child-Pugh (CP) Grade A (68%) and 36% were of Albumin-Bilirubin (ALBI) Grade 1. About 76% had Hepatitis B-related HCC. Regarding prior ICIs, 96% used anti-PD-1 antibodies (nivolumab 76%, pembrolizumab 20%) while 4% used atezolizumab with bevacizumab. The majority (84%) of patients received prior ICI as mono therapy. The median time on prior ICI was 4.86 months (range 0–21.2) and 48% had primary resistance. Most patients had documented radiological progression on prior ICI. Overall, 48% received ipilimumab with nivolumab and 52% received ipilimumab with pembrolizumab. Online supplemental table 1 shows the combined ICI regime according to prior ICI treatment. Of note, 60% of patients received ipilimumab and nivolumab/pembrolizumab as second-line, 28% as third-line and 12% as fourth-line systemic treatment. The median interval between the last dose of prior ICI and the first dose of ipilimumab and nivolumab/pembrolizumab was 3.00 weeks (range 1.29–13.0).
Supplemental material
Baseline characteristics
Clinical outcomes
The median follow-up was 37.7 months (95% CI: 32.8 to 42.7). At the study cut-off date, 28% of patients were still alive. No patients were lost to follow-up. Table 2 summarizes BORs. Overall, ORR was 16%, with three (12%) patients having CR and one (4%) patient having PR as their BORs. Another six (24%) patients achieved SD. Thus, 40% of patients achieved clinical benefits. The median DOR was 11.5 months (range 2.76–30.3). Two patients of DOR 10.6 months and 30.3 months continued to be in CR at the study cut-off date. One patient with CR had treatment suspension after two cycles due to TRAE and had tumor recurrence after a DOR of 12.4 months. There were no differences in the BOR of any patients using the RECIST 1.1 and iRECIST criteria.
Best objective response
The median TTP was 2.96 months (95% CI: 1.61 to 4.31). Overall, the median OS was 10.9 months (95% CI: 3.99 to 17.8, figure 1). The 1-year, 2-year and 3-year survival rates were 42.4%, 32.3% and 21.6%, respectively. 40% of patients received other subsequent systemic therapies.
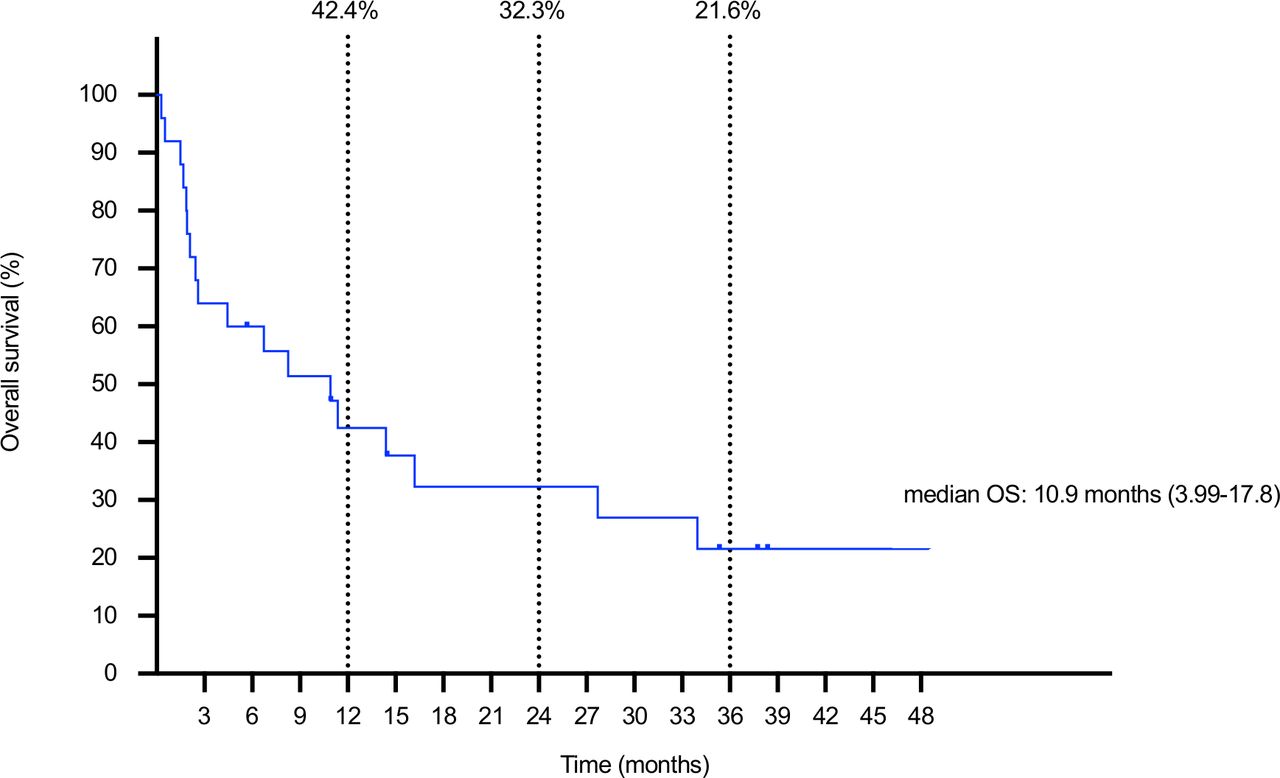
Kaplan-Meier analysis of OS. Dotted lines plot time points, percentages represent survival rates. OS, overall survival.
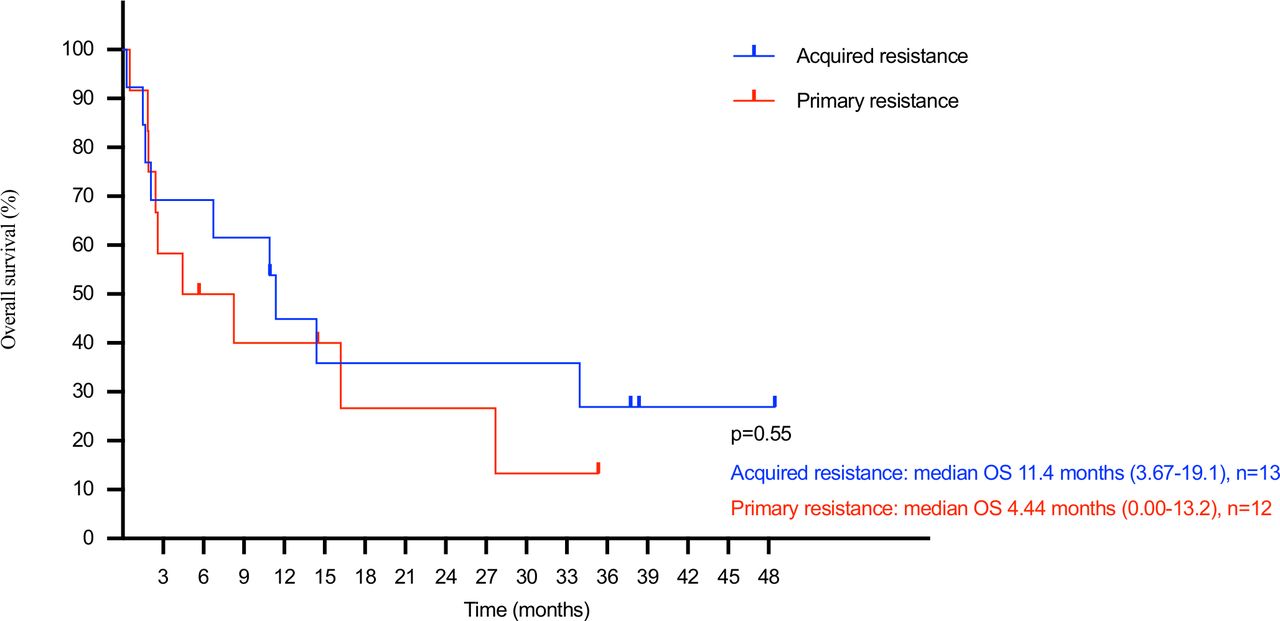
The ORR of patients with primary resistance to prior ICI was 16.7% versus 15.4% of those with prior acquired resistance (p=1.00). Nevertheless, patients with prior primary resistance had a median OS of 4.44 months (95% CI: 0.00 to 13.2), compared with 11.4 months (95% CI: 3.67 to 19.1) of those with prior acquired resistance (p=0.55, figure 2). Importantly, all responders were of CP A at first dose. About 50% of responders were of ALBI Grade 1 and the rest Grade 2. Baseline CP Grade (A vs B or C) was significantly associated with OS (median OS 16.2 months (95% CI: 7.56 to 24.8) vs 1.87 months (95% CI: 1.28 to 2.47), p=0.006, figure 3). Baseline ALBI Grade was also significantly associated with OS (median OS Grade 1 not reached, Grade 2 10.9 months (95% CI: 5.91 to 15.9), Grade 3 1.68 months (95% CI: 0.00 to 4.14), p<0.001, figure 4).
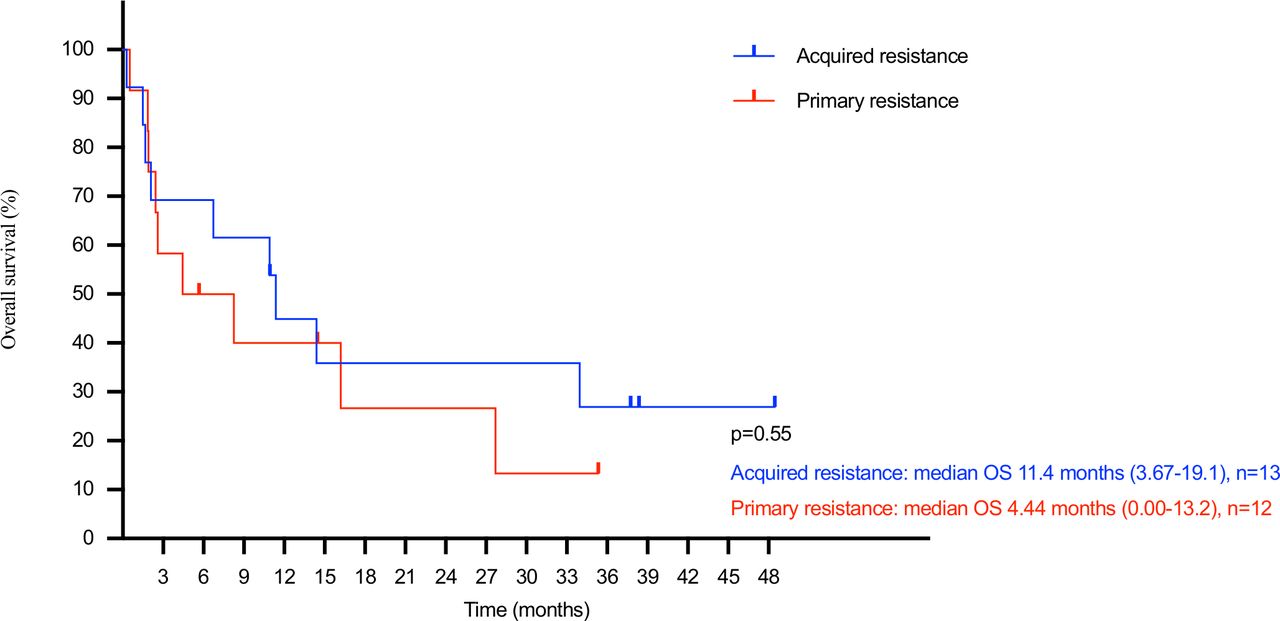
Kaplan-Meier analysis of OS by resistance pattern to prior ICI. Level of significance: p=0.55 (log-rank test). ICI, immune checkpoint inhibitor; OS, overall survival.

Kaplan-Meier analysis of OS by CP Grade. Level of significance: p=0.006 (log-rank test). CP, Child-Pugh; OS, overall survival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier analysis of OS by ALBI Grade. Level of significance: p<0.001 (log-rank test). ALBI, Albumin-Bilirubin; OS, overall survival.
Dosing, safety and TRAEs
The median dose received was three (range 1–22). Only 36% of patients completed four doses of induction ipilimumab and nivolumab/pembrolizumab. No delay in dosing was observed. About 48% of patients stopped treatment due to progressive disease, 16% due to TRAEs, 16% due to non-cancer death and 8% due to infections and other unrelated causes. About 8% of patients were still receiving therapy at study cut-off.
Table 3 shows all TRAEs that occurred in the analysis. Overall, 52% of patients experienced TRAEs. The most prevalent TRAE was skin-related (32%) followed by endocrinopathies (20%). Regarding Grade 3–4 TRAEs, one patient had Grade 3 hepatitis, and another had Grade 4 colitis. In total, three (12%) patients required systemic immunosuppressants. All three received corticosteroids. The median duration of corticosteroids given was 100 days (range 7–185) and the median initiation dose was 30 mg prednisolone (range 5–37.5). In addition, the patient with Grade 4 colitis received concomitant budesonide and mycophenolate mofetil, while a patient with toxic epidermal necrolysis (TEN) received concomitant intravenous immunoglobulin therapy. The patients with Grade 3 hepatitis and Grade 4 colitis recovered after systemic immunosuppressants without any long-term sequelae. One Grade 5 fatal TRAE occurred in a patient who developed TEN after the first dose of ipilimumab and nivolumab. Any grade TRAE was significantly associated with OS (median OS any TRAE 16.2 months (95% CI: 8.38 to 24.0) vs no TRAE 2.10 months (95% CI: 0.93 to 3.27), p=0.024, online supplemental figure 1). However, there was no association between any TRAE and objective responses (p=1.00) or clinical benefit (p=0.69).
Supplemental material
Treatment related adverse events
Discussion
Our present analysis reports an overall ORR of 16% and median OS of 10.9 months after a long-term follow-up of 37.7 months in patients with advanced HCC treated with ipilimumab and nivolumab/pembrolizumab after tumor progression on prior anti-PD-1/L1. Importantly, three (12%) patients achieved CR. Responses were also durable, with a median DOR of 11.5 months. These results are encouraging as the majority of analyzed patients were heavily pretreated with poor prognosis. More importantly, these reported ORR, DOR and OS provide important information to address the emergent clinical problem of how to treat patients with anti-PD-1/L1 refractory advanced HCC.
In fact, salvage ipilimumab with nivolumab after prior anti-PD-1/L1 has been described in patients with renal cell carcinoma (RCC), melanoma and non-small cell lung cancer (NSCLC).9–12 All these studies demonstrated ORRs of about 10%–20% and similar TRAE incidences compared with our analysis. The observation that response rates to ipilimumab-anti-PD-1 were similar regardless of prior anti-PD-1/L1 response was also shared by two such studies.9 10 Notably, our analysis demonstrated an impressive CR rate (12%). Multiple prospective clinical trials are currently underway to investigate ipilimumab–nivolumab after prior PD-1/L1 blockade for patients with RCC,16–18 NSCLC19 20 and melanoma.21 Nevertheless, no comparable prospective trial in patients with advanced HCC exists to the best of our knowledge.
Mechanistically, the effects of the PD-1 pathway on T cells occur predominantly during the effector phase. In contrast, the CTLA-4 pathway affects the immune priming and proliferation phases of T cells.22 Distinct genomic and functional signatures in T cells have been observed in combination blockade compared with single PD-1 pathway blockade.23 The following mechanisms may provide the scientific rationale for the clinical benefits of salvage combined CTLA-4 and PD-1 blockade in patients resistant to single PD-1 pathway blockade. In patients with primary resistance to single PD-1 pathway blockade, an immunosuppressive tumor microenvironment due to the presence of myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Treg) has been established as a key factor of tumor immune escape.24–26 Compared with single PD-1 pathway blockade, combined CTLA-4 and PD-1 blockade has been shown to increase the CD8 +T cell to MDSC ratio, as well as significantly decrease the fraction of Tregs expressing activation markers 4-1BB and KLRG1.27 On the other hand, in patients with acquired resistance to single PD-1 pathway blockade, PD-1 pathway blockade causes subsequent upregulation of alternative immune checkpoints such as CTLA-4,28 which may be reversed by CTLA-4 blockade. Furthermore, PD-1 pathway blockade does not activate genes associated with memory T cells, which have a greater longevity and proliferative capacity than effector T cells and confer longer-term tumor rejection.23 29 CTLA-4 blockade is associated with proliferation of transition memory T cells,23 which may provide more long-term tumor control. This may also explain the durability of response observed in this analysis, especially for the three patients in CR.
In this analysis, all responders were of CP A and of ALBI Grade 1 or 2. In addition, CP and ALBI grades were significantly associated with OS. Cirrhosis has been postulated to contribute to tumor immune escape through several mechanisms. First, cirrhotic livers have an increased extracellular matrix (ECM) content.30 ECM proteins may activate integrins causing the activation of transforming growth factor beta, a potent suppressor of anti-tumor immunity.31 ECM may also provide a physical barrier against immune cell infiltration.32 Second, liver fibrogenesis is mediated by activation of hepatic stellate cells (HSCs).33 HSCs have been shown to inhibit tumor lymphocytic infiltration, induce immunosuppressive cytokines, and induce the differentiation of both Treg and MDSCs, thus inhibiting both adaptive and innate immune responses.34 This analysis is in line with the above observations in its suggestion that the response to ICIs may be affected by the extent of cirrhosis. Interestingly, the CheckMate-040 cohort 5 study demonstrated that although patients with CP B advanced HCC might derive clinical benefits from single agent nivolumab, benefits were mostly limited to patients with CP B7 advanced HCC and survival benefits were less pronounced compared with patients with CP A advanced HCC.35 Further studies are needed to better illustrate the relationship between the degree of cirrhosis and ICI response.
Interestingly, the ORRs to ipilimumab and nivolumab/pembrolizumab in this analysis were similar regardless of whether the patient had primary or acquired resistance to prior anti-PD-1/L1. However, the median OS was much longer in patients with prior acquired resistance compared with those with primary resistance, although this was not statistically significant. In fact, the difference in OS might partly be due to differences in tumor biology: primary resistance patients may have more advanced tumor immune escape, resulting in quicker tumor progression and earlier death compared with acquired resistance patients. More importantly, our findings might imply that using ipilimumab and nivolumab/pembrolizumab might have better efficacy in patients with acquired resistance to prior anti-PD-1/L1 compared with primary resistance cases. The non-significant statistical result observed here was likely due to the small number of patients analyzed.
It is worthwhile to note that all patients in this analysis received ipilimumab at 1 mg/kg. There is evidence that the dose of ipilimumab and anti-PD-1, when used in combination, affects the OS of patients with advanced HCC. An analysis of the CheckMate-040 trial cohort 4 showed that among patients with advanced HCC treated with ipilimumab and nivolumab after sorafenib, the ipilimumab 3 mg/kg and nivolumab 1 mg/kg every 3 weeks arm achieved a median OS of 22.8 months and 8% CR rate, compared with 12.5 months and 6% in the ipilimumab 1 mg/kg and nivolumab 3 mg/kg every 3 weeks arm, and 12.7 months and 0% in the nivolumab 3 mg/kg every 2 weeks and ipilimumab 1 mg/kg every 6 weeks arm.7 In small cell lung cancer, improved OS was also reported with a higher ipilimumab dose.36 However, the important question of whether higher doses of ipilimumab (such as 3 mg/kg) may achieve even better ORRs and survival outcomes in patients with anti-PD-1/L1 resistance remains. Further mechanistic studies and clinical trials are warranted.
Overall, ipilimumab and nivolumab/pembrolizumab were well-tolerated, with only three (12%) patients having ≥Grade 3 TRAEs. Nevertheless, one treatment-related death occurred. The pattern and severity of TRAEs reported in this analysis are comparable to those of ipilimumab 1 mg/kg arms in published trials and lower than those of ipilimumab 3 mg/kg arms, consistent with trial observations that higher ipilimumab dosages are associated with increased incidence and severity of TRAEs.37–41 Patients who experienced any TRAE were observed to have superior OS compared with those who did not. Several possible explanations for this observation exist: the presence of TRAE may be the systemic effect of more active CD8+ T cells which also confer greater antitumor activity; on the other hand, TRAEs may not occur immediately after the first dose, and patients with longer survival had more time for TRAEs to manifest, resulting in an observed increase in TRAE incidence.
There are several limitations to this analysis, including small sample size, single-center nature, heterogeneous population, the inherent biases in a retrospective study, and lack of central blinded independent review for treatment responses. This limits the study to be hypothesis-generating only and cannot directly recommend the routine clinical use of ipilimumab and nivolumab/pembrolizumab. Additionally, the subgroup analyses contained small numbers of patients and thus larger-scale studies should be conducted to validate their findings. The OS might have been affected by other subsequent treatments. Finally, most patients were not pretreated with tyrosine kinase inhibitors such as sorafenib before receiving any anti-PD-1 ICI as recommended by current guidelines.
In conclusion, this study demonstrates that using ipilimumab and nivolumab/pembrolizumab as salvage therapy in patients with advanced HCC after tumor progression on prior anti-PD-1/L1 can achieve durable antitumor activity and encouraging survival outcomes with acceptable toxicity. Prospective clinical trials are urgently needed to validate the findings of this hypothesis-generating study and to address the unmet medical need.
Supplemental material
Acknowledgments
The authors thank the patients and their families, investigators and research staff at Queen Mary Hospital, Hong Kong. The authors also thank the Department of Medicine, Queen Mary Hospital, The University of Hong Kong, for funding support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at The American Society of Clinical Oncology 2021 Gastrointestinal Cancer Symposium.
Contributors JSLW and TY conceived and designed the study. JSLW, GGWK, VT, BCWL, RL, JC, KWM, WHS, JT, CML, TTC and TY recruited patients and collected the data. JSLW, VT and TY analyzed the data. All authors interpreted the data and were involved in development, review, and approval of the manuscript.
Funding This study was funded by the Research Grant Council-Theme Based Research Fund (T12-704/16-R).
Competing interests TY reports receiving honoraria from Bristol-Myers Squibb and MSD. TY has a consulting or advisory role at Bristol-Myers Squibb and MSD. JC reports receiving honoraria from Bristol-Myers Squibb and has a consulting or advisory role at Bristol-Myers Squibb. JSLW, GGWK, VT, BCWL, RL, KWM, WHS, JT, CML, and TTC have nothing to disclose.
Patient consent for publication Not required.
Ethics approval This study was approved by The University of Hong Kong/Hospital Authority Hong Kong West Cluster Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The study only utilized deidentified patient data collected from the authors’ own institution.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.