Article Text

Abstract
Background Emerging clinical data suggest that an immune checkpoint inhibitor in combination with an antiangiogenic agent is a reasonable strategy for multiple malignancies. We assessed the combination of camrelizumab with apatinib in pretreated advanced primary liver cancer (PLC, cohort A) from a multicohort phase Ib/II trial.
Methods Patients with PLC after prior systemic treatment(s) were administered camrelizumab (3 mg/kg, once every 2 weeks) plus apatinib (125, 250, 375, or 500 mg; once per day) in a 3+3 dose-escalation stage and subsequent expansion stage. The primary endpoints were tolerability and safety of study treatment.
Results From April 2017 to July 2019, 28 patients (21 with hepatocellular carcinoma and 7 with intrahepatic cholangiocarcinoma) received camrelizumab plus apatinib. Two dose-limiting toxicities (both grade 3 diarrhea) were reported in the 500 mg cohort. Therefore, the 375 mg cohort was expanded. Of the 19 patients in the 375 mg cohort, dose reduction to 250 mg occurred in 8 patients within 2 months after treatment initiation. Of the 28 patients with PLC, 26 had grade ≥3 treatment-related adverse events, with hypertension being the most common (9/28). One treatment-related death occurred. The objective response rate was 10.7% (95% CI 2.3% to 28.2%). Median progression-free survival and overall survival were 3.7 months (95% CI 2.0 to 5.8) and 13.2 months (95% CI 8.9 to not reached), respectively.
Conclusion The combination of camrelizumab with apatinib had a manageable toxicity and promising antitumor activity in patients with advanced PLC. Apatinib at a dose of 250 mg is recommended as a combination therapy for further studies of advanced PLC treatment.
Trial registration numbers NCT03092895.
- drug therapy
- combination
- immunotherapy
- liver neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Primary liver cancer (PLC) consists mainly of hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma (ICC), and mixed HCC–ICC type, of which about 90% are HCC.1 In 2018, there were 841 000 new cases of PLC worldwide, with 782 000 deaths. China is an area with a high PLC incidence, contributing to >50% of the new cases and deaths globally.1 2 Patients with PLC are often diagnosed at the locally advanced stage or on developing distant metastasis, which is not suitable for surgery or other local treatment, thereby leading to poor prognosis with a 5-year survival rate of only 10%–20%.3
Since the development of sorafenib and systematic chemotherapy containing oxaliplatin in recent years, the progress of systemic therapy for advanced PLC mainly came from antiangiogenic molecular target drugs and immune checkpoint inhibitors (ICIs).4 The median overall survival (mOS) for sorafenib, lenvatinib, regorafenib, cabozantinib, ramucirumab, and donafenib as first-line or second-line therapy for advanced PLC is between 6.5 months and 13.6 months, and most objective response rates (ORRs) are <10%.4–6 Compared with traditional molecular target drugs and systemic chemotherapy, ICIs, represented by programmed death-1 (PD-1)/programmed death ligand-1 (PD-L1) inhibitors (such as nivolumab and pembrolizumab), have significantly improved the effectiveness in the treatment of advanced PLC, with the ORR being up to 15%–20%7 8; nevertheless, the overall effect remains limited. PLC has the dual characteristics of a rich blood supply and innate immune tolerance. Previous studies have shown that antiangiogenic drugs can reverse the immunosuppressive status of the tumor microenvironment,9 and in combination with ICIs they can be synergistic, which is a promising therapeutic strategy to improve the efficacy of treatment for advanced PLC.
Camrelizumab is a humanized PD-1 monoclonal antibody that has a high affinity (KD=3.31 nmol/L) with PD-1, a high occupancy of circulating T-lymphocyte receptors (85% at a dose of 200 mg),10 and a good tolerance and curative effect on a variety of solid tumors, including PLC.11 On the other hand, apatinib is a highly selective small-molecule tyrosine kinase inhibitor of vascular endothelial growth factor receptor 2 (VEGFR-2). Results from phase II clinical trials have shown that apatinib as a first-line treatment has potential survival benefits for Chinese patients with advanced HCC.12
Based on these theoretical bases and clinical data, we conducted a clinical trial on camrelizumab in combination with apatinib for the treatment of patients with advanced PLC. The patients enrolled in this study were from cohort A in a phase Ib/II trial of camrelizumab in combination with apatinib or chemotherapy in advanced PLC or biliary-tract cancer (BTC). The treatment results of this cohort are reported herein.
Methods
Study design and subjects
Patients were from cohort A of an open, multicenter, multicohort phase Ib/II clinical trial of camrelizumab in combination with apatinib or chemotherapy in the treatment of advanced PLC or BTC. Patients with advanced PLC who failed or could not tolerate systematic therapy were enrolled in this study. Eligible patients were 18–70 years old, had a histologically or cytologically confirmed diagnosis of advanced PLC, were unsuitable for surgery or local treatment, had at least one measurable lesion as defined by the Response Evaluation Criteria in Solid Tumors (RECIST) V.1.1, had a Child-Pugh score of ≤7, had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1, had a predicted life expectancy of greater than 12 weeks and had adequate organ function. Patients with chronic hepatitis B virus (HBV) infections with a viral load of <500 IU/mL were permitted to enroll, and those infected with HBV and hepatitis C virus were required to receive standardized antiviral treatment. The main exclusion criteria were as follows: current or previous pulmonary fibrosis; interstitial pneumonia; active or prior autoimmune disease; previous abdominal fistula, gastrointestinal perforation, or abdominal abscess in the past 2 months; previous gastrointestinal bleeding or clear tendency of gastrointestinal bleeding in the past 6 months; current or previous central nervous system metastasis; local treatment for the liver (including but not limited to surgery, radiation therapy, hepatic artery embolization, transarterial chemoembolization, hepatic artery perfusion, radiofrequency ablation, cryoablation, or percutaneous ethanol injection) within 4 weeks before enrollment; grades 3–4 cardiac insufficiency (New York Heart Association standard); and hypertension not well controlled by antihypertensive drugs.
Procedures
This study included two stages: the first stage was to determine the maximum tolerable dose (MTD) in a 3+3 dose-escalation stage, and the second stage was the dose-expansion stage.
In the dose-escalation stage, the camrelizumab dose was set to 3 mg/kg, intravenously, once every 2 weeks. The initial dose of apatinib was 125 mg, oral, once per day (QD), which was then increased stepwise to 250 mg QD, 375 mg QD, and 500 mg QD. Three to six patients were included in each dose group. The observation period for the dose-limiting toxicity (DLT) was the first cycle of continuous administration (28 days). If DLT occurred in two patients in a certain dose group, the dose escalation was stopped. The prior dose would be considered as the MTD. Afterwards, a total of 12 patients were entered into the dose-expansion stage.
The patients were administered with camrelizumab in combination with apatinib until investigator-assessed disease progression (according to RECIST V.1.1), unacceptable toxicity, withdrawal of consent, investigator decision, or study completion. For patients with radiological disease progression, if the investigator judged that the patients would benefit from and were tolerant of continued treatment, and if the patient had been informed and provided voluntary consent, the combination treatment was allowed to continue. During treatment, camrelizumab could be suspended for <6 weeks to manage adverse events (AEs), although the camrelizumab dose was not allowed to be adjusted. On the other hand, apatinib could be suspended for <28 days, and the dose was allowed to be reduced (except in the 125 mg group).
Outcomes
The primary endpoints of this study were the safety and tolerance of camrelizumab in combination with apatinib in the treatment of advanced PLC. The secondary endpoints included ORR, duration of response (DoR), progression-free survival, time to progression, disease control rate (DCR), and OS.
During the study, any AEs and laboratory abnormalities were monitored and recorded from the time of informed consent until 90 days after the last administration, and were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events V.4.03.
Tumor imaging evaluation was performed every 8 weeks (±7 days) during the study period, and the tumor responses were evaluated according to the RECIST V.1.1 criteria. Complete responses (CRs) or partial responses (PRs) were required to be confirmed at least 4 weeks after the first response.
Statistical analysis
The sample size of this study was not based on the statistical hypothesis test but was determined according to the dose-escalation rules of 3+3 and the number of patients in the expansion stage. All patients who received at least one study drug treatment and had safety evaluation data were included in the safety set (SS). All patients who received the study drug at least once were included in the full analysis set (FAS). Statistical analyses were performed using the Statistical Analysis Software V.9.4. The Kaplan-Meier method was used to estimate mOS, median progression-free survival (mPFS), median time to progression (mTTP), and median duration of response (mDoR), and the Brookmeyer and Crowley methods were used to estimate their bilateral 95% CI. The Clopper-Pearson method was used to calculate the 95% CI for ORR and DCR.
Results
Patient baseline characteristics
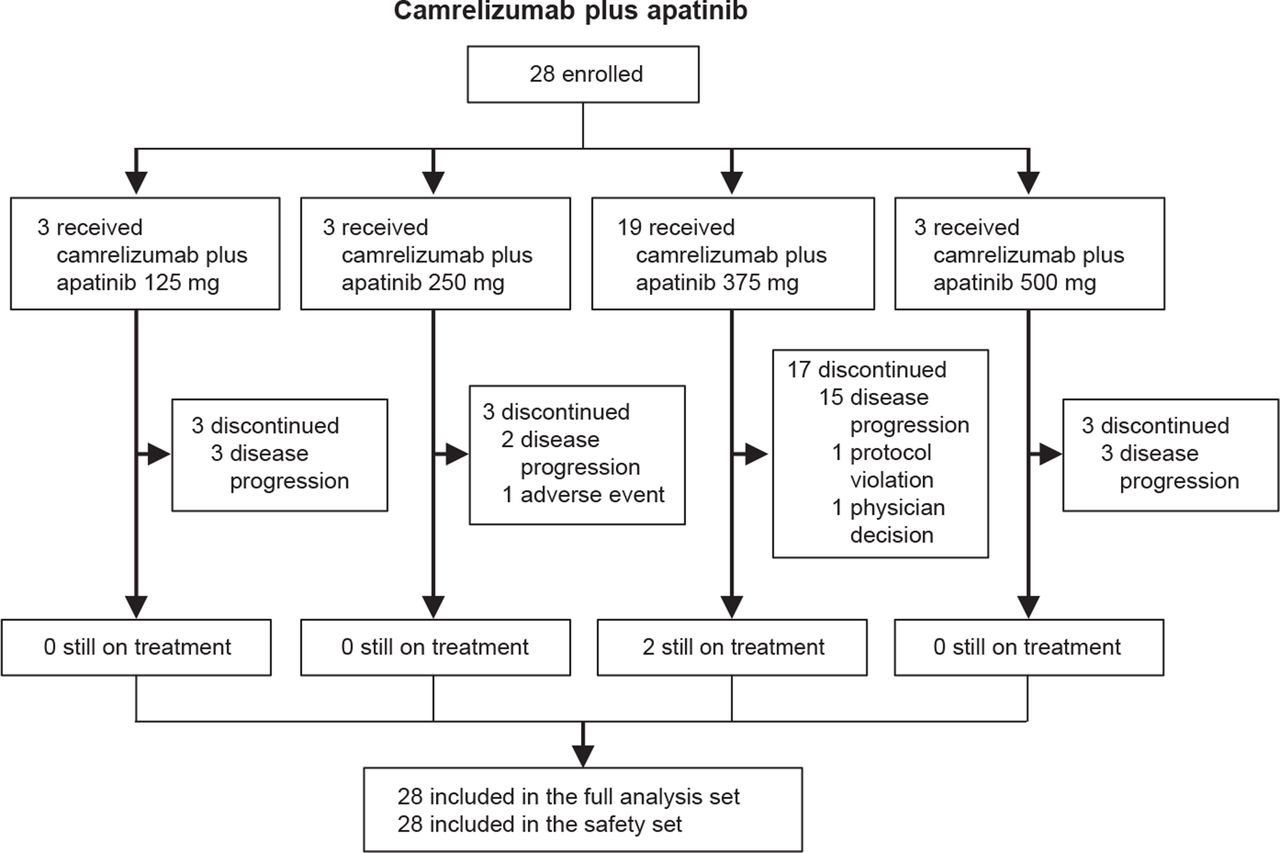
From April 28, 2017 to June 28, 2018, 28 patients from three clinical centers were enrolled and treated with camrelizumab in combination with apatinib. All patients were included in the SS and FAS. The data cut-off was on July 15, 2019, and the median follow-up duration was 12.4 months (range, 2.3–26.3). The median exposure times of camrelizumab and apatinib were 5.8 months (range, 0.9–17.9) and 5.5 months (range, 0.5–20.0), respectively. At data cut-off, 26 patients (92.9%) discontinued the combination treatment, and 2 patients (7.1%) remained under treatment. The causes of treatment discontinuation were disease progression (23 patients, 82.1%), protocol violation (1 patient, 3.6%), AE (1 patient, 3.6%), and researcher judgment (1 patient, 3.6%), as shown in figure 1.

Trial profiles.
Demographic and disease baseline characteristics of patients are presented in table 1. Of the 28 patients, 21 (75.0%) and 7 (25.0%) had HCC and ICC, respectively; the median age was 52 years (range, 34–67); 21 (75.0%) patients were female; 18 (64.3%) patients had an ECOG score of 1; 15 (53.6%) patients had an alpha-fetoprotein level of ≥400 ng/mL; 18 (64.3%) were at Barcelona Clinic Liver Cancer stage C; 26 (92.9%) patients had extrahepatic metastasis; and 22 (78.6%) patients were infected with HBV.
Baseline characteristics
Tolerability and safety
A total of 12 patients were enrolled into the dose-escalation stage, with three patients in each dose group. No protocol-defined DLTs were reported in the apatinib 125, 250, and 375 mg groups, whereas two patients in the apatinib 500 mg group had DLTs, both of which had grade 3 diarrhea. Therefore, the MTD was 375 mg, and camrelizumab in combination with apatinib 375 mg was selected for further dose expansion in 19 patients. All the 19 patients in the 375 mg group had experienced treatment interruption in the apatinib treatment, and the dose was reduced to 250 mg in eight patients (42.1%) within 2 months after the initiation of treatment (figure 2).
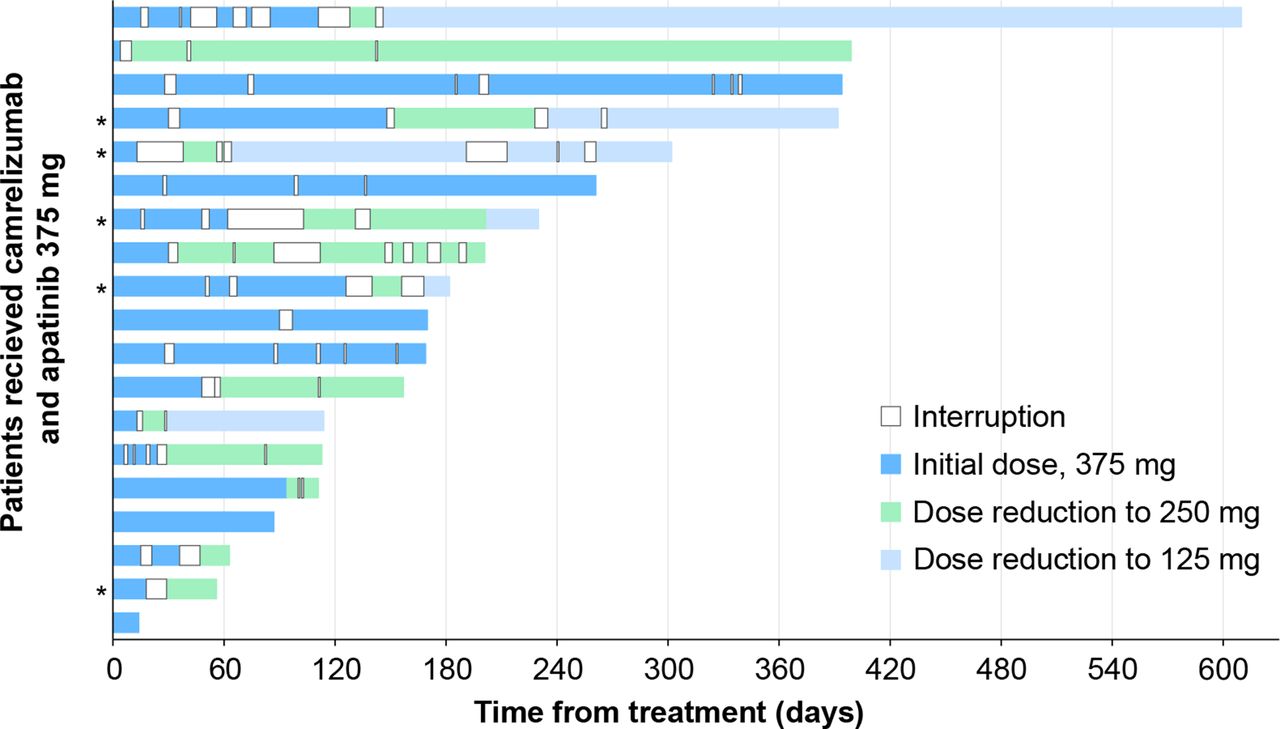
Treatment interruption and dose reduction of apatinib in the 375 mg group. Apatinib administration was interrupted in all 19 patients due to adverse events but was never resumed in two patients as the prespecified criteria for treatment resumption were not met, and the two patients progressed before the cut-off date. The 5 patients with intrahepatic cholangiocarcinoma were labeled with asterisks (*), and the other 14 patients with hepatocellular carcinoma were unlabeled.
All 28 patients among the four dose groups had at least one treatment-related adverse event (TRAE, table 2). TRAEs occurring in ≥50% of patients included hypertension (20 patients, 71.4%), decreased white blood cell count (16 patients, 57.1%), increased aspartate aminotransferase (16 patients, 57.1%), decreased platelet count (16 patients, 57.1%), decreased neutrophil count (15 patients, 53.6%), and proteinuria (14 patients, 50.0%). Grade ≥3 TRAEs occurred in 26 patients (92.9%), with the most frequent ones being hypertension (nine patients, 32.1%), decreased neutrophil count (five patients, 17.9%), and decreased platelet count (four patients, 14.3%). One patient (3.6%) in the 375 mg dose group died of pneumonia, and this AE was considered as treatment-related. A total of 15 patients (53.6%) had interrupted treatment or had reduced apatinib dose due to TRAEs (online supplemental table S1), and 1 patient (3.6%) in the 375 mg dose group had their treatment discontinued because of a TRAE (decreased platelet count).
Supplemental material
TRAEs
Serious TRAEs were observed in four patients (14.3%), including herpes zoster (one patient, 3.6%), decreased platelet count (one patient, 3.6%), pneumonitis (one patient, 3.6%), upper gastrointestinal hemorrhage (one patient, 3.6%), and anemia (one patient, 3.6%); all of them occurred in the 375 mg group. Among them, three patients (10.7%) had grade ≥3 serious TRAEs, including decreased platelet count (one patient, 3.6%), pneumonitis (one patient, 3.6%), and anemia (one patient, 3.6%).
Reactive cutaneous capillary endothelial proliferation (RCCEP) occurred in six patients (21.4%), of which one patient presented concomitant reactive capillary endothelial proliferation in the gingiva. As of data cut-off, the RCCEP in four patients had been relieved, and the reactive capillary endothelial proliferation in the gingiva in one patient had been relieved.
Immune-related adverse events (irAEs) were reported in 11 (39.3%) patients, and three patients had grade ≥3 irAEs (online supplemental table S2). The most frequently occurring irAEs included increased aspartate aminotransferase, hypothyroidism, and reactive capillary endothelial proliferation (two patients, 7.1% for each).
Preliminary efficacy
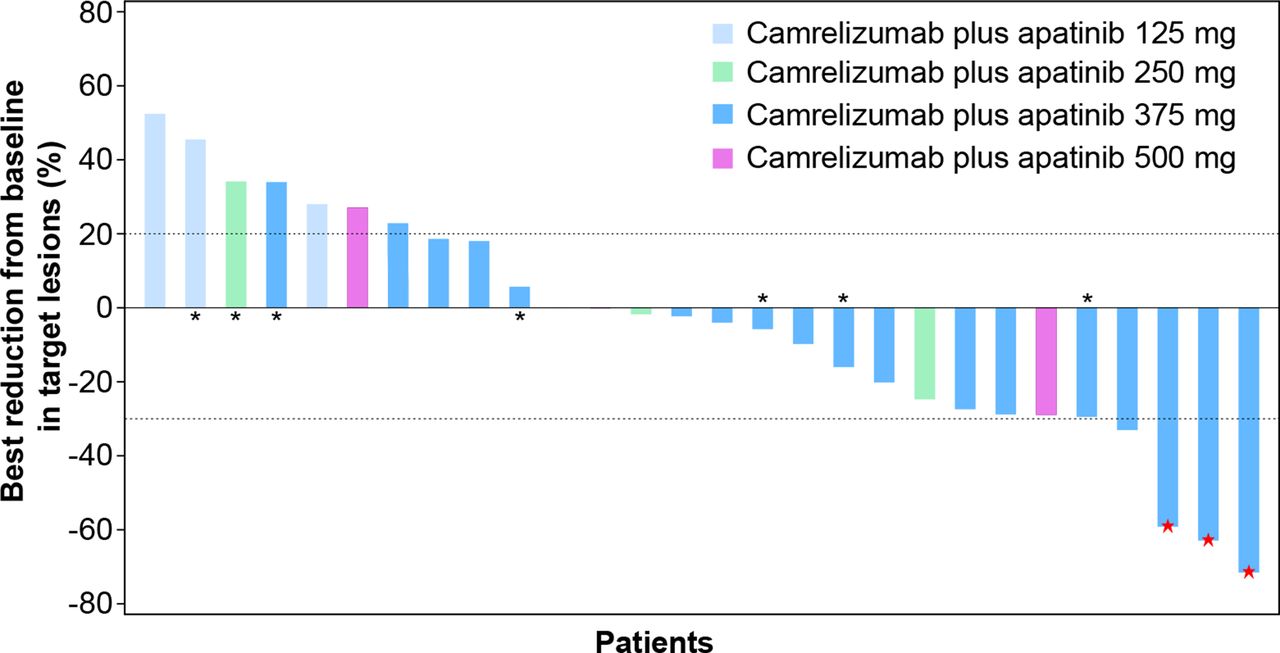
As of July 15, 2019, no patient achieved CR; 3 patients (10.7%) achieved PR, 16 patients (57.1%) had stable disease, and 9 patients (32.1%) had progressive disease as their best response. The ORR and DCR were 10.7% (95% CI 2.3% to 28.2%) and 67.9% (95% CI 47.6% to 84.1%), respectively. The best percentage changes from baseline in size of target lesions are presented in figure 3. The three patients who exhibited PR all had HCC, with a median time to response of 3.7 months (range, 1.8–3.7). The DoR was 7.2+ months, 11.3 months, and 16.4+ months, respectively. As of data cut-off, two of these patients (66.7%) are still in response.
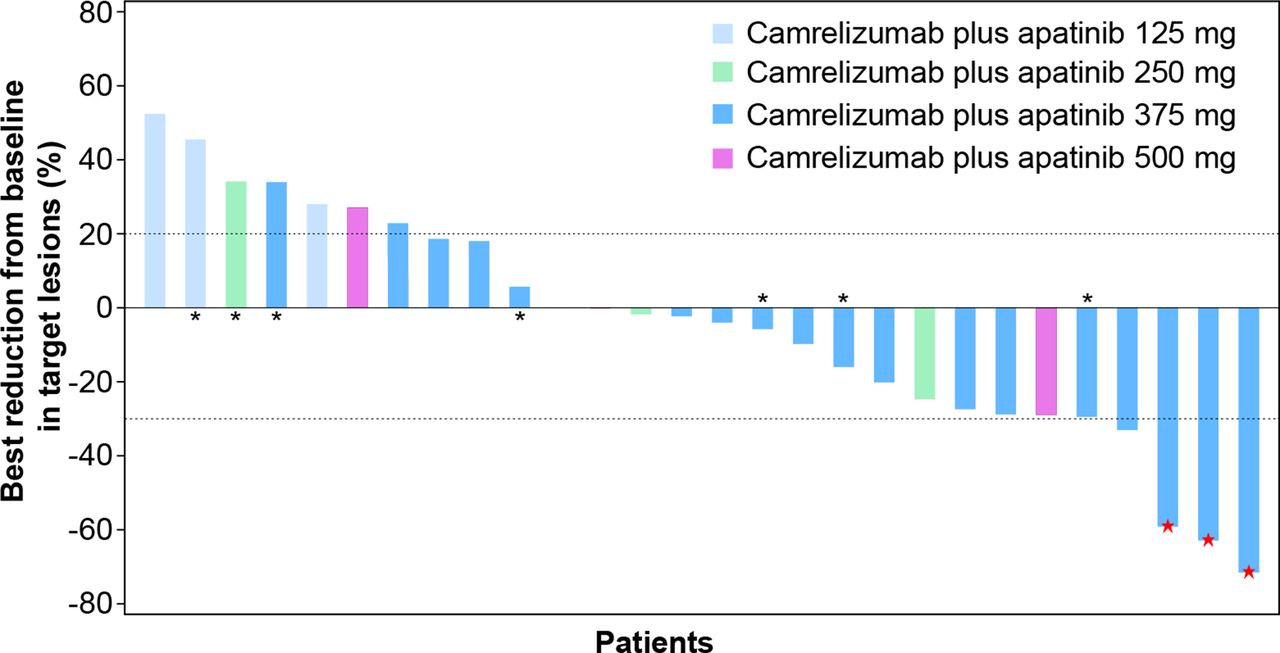
Best percentage changes from baseline in terms of the target lesion sizes. The red stars represent the patients with confirmed partial response. The seven patients with intrahepatic cholangiocarcinoma were labeled with asterisks (*), and the other 21 patients had hepatocellular carcinoma.
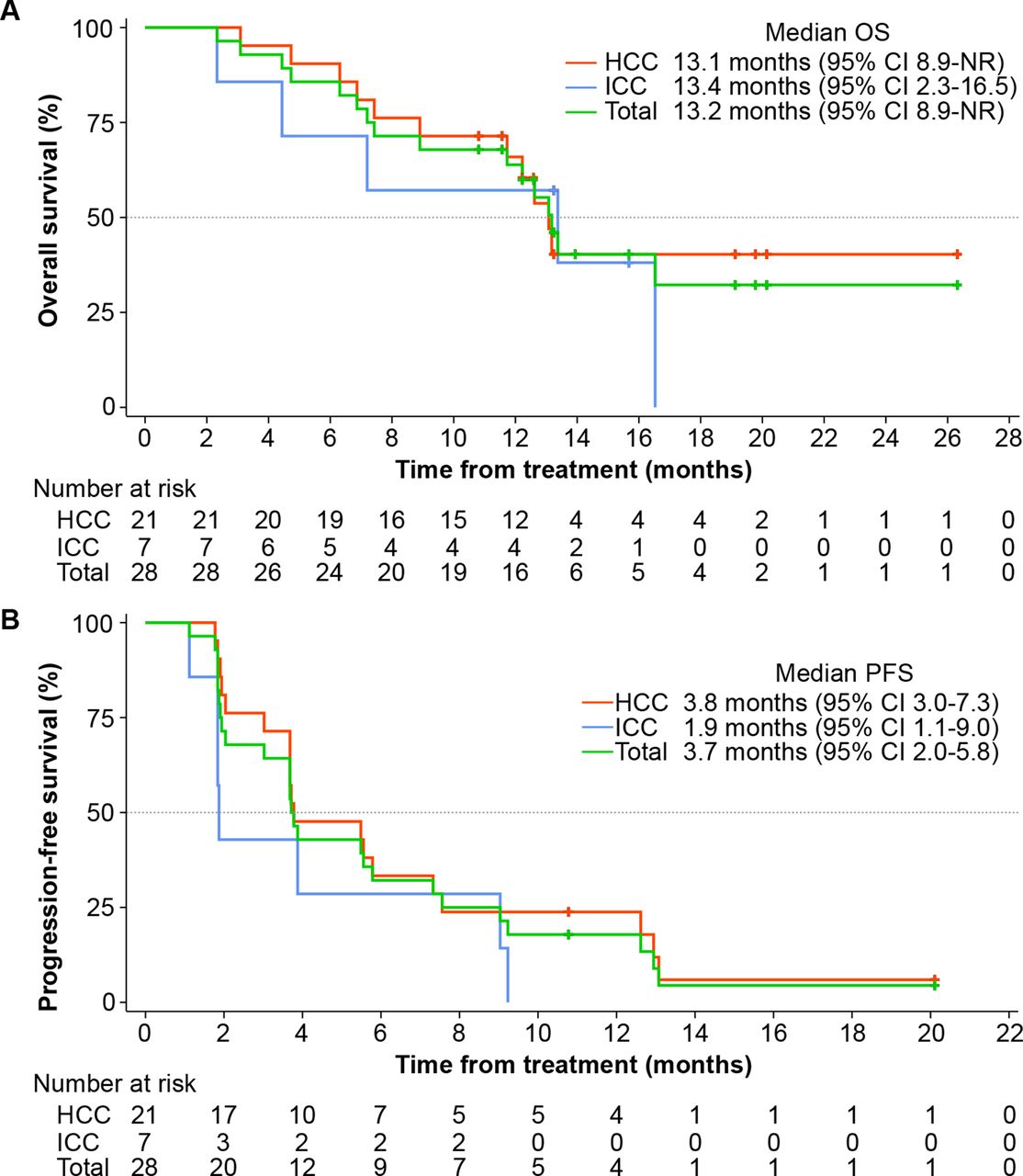
As of the data cut-off date, 16 patients (57.1%) died and 12 patients (42.9%) were undergoing survival follow-up. The mOS was 13.2 months (95% CI 8.9 to not reached), of which the mOS for HCC and ICC was 13.1 months (95% CI 8.9 to not reached) and 13.4 months (95% CI 2.3 to 16.5), respectively (figure 4A). The 6-month OS rate was 85.7% (95% CI 66.3% to 94.4%) and the 12-month OS rate was 63.9% (95% CI 43.2% to 78.7%). The 6-month OS rates for HCC and ICC were 90.5% (95% CI 67.0% to 97.5%) and 71.4% (95% CI 25.8% to 92.0%), respectively, and the 12 month OS rates were 65.9% (95% CI 41.4% to 82.2%) and 57.1% (95% CI 17.2% to 83.7%), respectively. Both mPFS and mTTP were 3.7 months (95% CI 2.0 to 5.8); both mPFS and mTTP of HCC were 3.8 months (95% CI 3.0 to 7.3); and both mPFS and mTTP of ICC were 1.9 months (95% CI 1.1 to 9.0) (figure 4B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) OS and (B) PFS. HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; NR, not reached; OS, overall survival; PFS, progression-free survival.
Discussion
The treatment of PLC has entered a new era through immunotherapy. Based on the results of the CheckMate-040 and KEYNOTE-224 trials, the US Food and Drug Administration conditionally approved nivolumab and pembrolizumab as the second-line therapy for advanced HCC in 2017 and 2018, respectively. However, two confirmatory pivotal phase III studies in 2019, CheckMate-459 and KEYNOTE-224, did not achieve the preset main research endpoints.7 8 Therefore, combined immunotherapy, including those in combination with antiangiogenic targeted drugs and systemic chemotherapy, has become the main strategy to improve the efficacy of ICI monotherapy. The prospect of combination with antiangiogenic targeted drugs is particularly promising. At present, the results of several clinical studies of ICIs combined with antiangiogenic drugs in the treatment of advanced HCC are encouraging. In a phase III study of atezolizumab (PD-L1 monoclonal antibody) and bevacizumab (VEGF monoclonal antibody) in the first-line treatment of advanced HCC (IMbrave150), the ORR of the combined therapy reached 33%, with the main endpoints of the study being mPFS of 6.8 months and mOS, which had not yet been achieved, making it the first phase III study in which the first-line efficacy was better than that of sorafenib.13 In addition, in 2020, the American Society of Clinical Oncology (ASCO) and ASCO–Gastrointestinal Cancers reported phase Ib data of patients with advanced HCC treated with pembrolizumab combined with lenvatinib and nivolumab, respectively. The ORRs of the combined treatment were as high as 46.3% and 76.7%, respectively, and the mOS of pembrolizumab in combination with lenvatinib was 20.4 months, which was nearly twice that of sorafenib.14 15
As new class I drugs independently developed in China, both camrelizumab and apatinib are effective in the monotherapy of Chinese patients with advanced HCC. A phase II study of Chinese patients with advanced PLC by Qin et al showed that the efficacy of camrelizumab was similar to that of comparable foreign drugs, with an ORR and mOS of 14.7% and 13.8 months, respectively,16 despite the patient’s baseline demographics being more complex. In 2020, ASCO published the results of a randomized, double blind, placebo controlled, multicenter phase III study of apatinib in the second-line treatment of advanced HCC in China,17 and the mOS (8.7 months vs 6.8 months) and ORR (10.7% vs 1.5%) in the apatinib group were significantly better than those in the placebo group. Therefore, camrelizumab monoclonal antibody in combination with apatinib has strong clinical data to support the treatment of PLC.
In previous basic experiments, we observed that the tumor inhibition rates of camrelizumab (3 mg/kg) combined with apatinib (200 and 100 mg/kg) in human PD-1 transgenic mice reached 63.1% and 87.3%, respectively, which were significantly higher than those in the control group, and that the curative effect of low-dose apatinib seemed to be better. In the current study, a fixed dose of camrelizumab monoclonal antibody (3 mg/kg, intravenously, Q2W) was used to explore the MTD of apatinib for combination therapy. Although 375 mg was determined as the MTD of apatinib during the dose-escalation phase, three patients with DLTs were observed in the dose-expansion phase, and treatment was therefore interrupted in all patients. The proportion of patients with reduced dose who experienced AEs within 2 months after administration reached 42.1%. Basic studies have found that high-dose or long-term anti-VEGF therapy can even aggravate hypoxia and immunosuppression of the tumor microenvironment.18 Therefore, considering safety and efficacy, we recommend a lower dose of apatinib (250 mg, QD) in further combination studies.
No unexpected TRAEs were reported in this study, and the common grade ≥3 TRAEs were hypertension (nine patients, 32.1%), decreased neutrophil count (five patients, 17.9%), and decreased platelet count (four patients, 14.3%). The overall incidence rate was similar to that reported in studies using apatinib alone in the treatment of PLC.12 17 Combined with camrelizumab, apatinib did not significantly increase the incidence of TRAEs. On the other hand, RCCEP is a skin immune-related adverse reaction caused by the camrelizumab monoclonal antibody, and its incidence is significantly higher than that of other PD-1 monoclonal antibodies, which could reach 66.8% in HCC; however, it is positively correlated with the curative effect.19 There is a large proportion of proliferative vascular endothelial cells with high expression of VEGF-A and VEGFR-2 in RCCEP lesions, indicating that the pathogenesis may be related to the VEGFR-2 signal pathway.20–22 The incidence of RCCEP in this study was 21.4%, which was significantly lower than that of camrelizumab, and which may be related to the specific VEGFR-2 inhibition of apatinib.
In this study, seven patients with ICC (25.0%) with poor prognosis were included, and the three patients who achieved PR were all patients with HCC (a total of 21 cases), with an ORR of 14.3%. A phase I study of camrelizumab combined with apatinib in the treatment of advanced HCC, gastric cancer, and esophagogastric junction cancer by Xu et al recruited 16 patients with PLC (all were HCC), whose ORR, DCR, and mPFS were 50.0%, 93.8%, and 5.8 months, respectively.23 These findings are dramatically different from those in our study, which is numerically similar to the efficacy of a study on durvalumab combined with ramucirumab as a posterior line in the treatment of patients with advanced HCC, with an ORR of 11%, a DCR of 61%, and an mPFS of 4.4 months.24 Compared with camrelizumab monotherapy, camrelizumab in combination with apatinib as second-line treatment for PLC showed higher DCR (67.9% vs 44.2%), longer mPFS (3.7 vs 2.1 months), and higher 6-month OS rate (85.7% vs 74.4%).11 Therefore, the combination with apatinib has the potential to further improve camrelizumab efficacy.
PLC has a high degree of heterogeneity, and there are obvious differences between Eastern and Western PLC. This study is only exploratory in nature, and hence there are some limitations, such as small sample size and not having a single pathological type among the patients. Therefore, the analysis of correlation of PD-L1 and efficacy was not included in this study, and it is necessary to be cautious when comparing our findings with those of other similar studies. Our conclusions need to be verified in further prospective studies with larger sample sizes. The lack of tumor response assessment according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) guideline may also be considered as a limitation. In addition, the pathogenesis of PLC remains unclear, and there is currently no recognized driving gene and molecular typing; thus, no biomarkers related to prognosis were included in this study, which is worthy of further exploration in future research.
In summary, for patients with advanced PLC, camrelizumab in combination with apatinib can achieve controllable safety and good efficacy, thereby providing a new treatment option with clinical benefits for patients with advanced PLC. This study demonstrated that the combination of apatinib has the potential to further improve the efficacy of camrelizumab, which provides a reference basis for further studies. Therefore, we are currently conducting a confirmatory phase III study, namely, the international multicenter randomized phase III study of camrelizumab combined with apatinib in the first-line treatment of advanced HCC.
Acknowledgments
We thank the investigators, site personnel, and patients for participating in this trial. This study was sponsored and funded by Jiangsu Hengrui Medicine Co., Ltd. We thank Xiao Zhang (Jiangsu Hengrui Medicine) for his input on statistical analyses. Medical writing support was provided by Tengfei Zhang, PhD (medical writer at Jiangsu Hengrui Medicine), according to Good Publication Practice Guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design of the study: KM, SQ, LW, and JZ. Collection and assembly of clinical data: KM, SQ, ZC, YL, and LW. Collection and execution of correlative studies: KM, SQ, ZC, YL, and LW. Data analysis and interpretation of results: KM, SQ, LW, and JZ. Writing and revision and final approval of the manuscript: all authors.
Funding This work was supported by Jiangsu Hengrui Medicine Co., Ltd.
Competing interests LW and JZ are employees of Jiangsu Hengrui Medicine Co., Ltd.
Patient consent for publication Not required.
Ethics approval The study protocol and all amendments were reviewed and approved by the ethics committee of each study site. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. The institutional review boards or independent ethics committees of all participating centers approved the protocol and amendments. All patients provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Any additional data pertaining to this manuscript are available from the corresponding author upon reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.