Article Text

Abstract
Background Programmed death-1 (PD-1) blockade monotherapy induced durable remission in a subset of patients with relapsed/refractory classical Hodgkin lymphoma (cHL). We asked whether the anti-PD-1 agent, camrelizumab, combined with the DNA demethylating agent, decitabine, improves progression-free survival (PFS) in patients with relapsed/refractory cHL over camrelizumab alone.
Methods This extended follow-up of an ongoing randomized phase II trial analyzed PFS among patients enrolled from January 2017 through July 2018. Sixty-one patients with relapsed/refractory cHL who were clinically naïve to PD-1 blockade and had received ≥2 previous therapies were randomized 1:2 to receive either camrelizumab (200 mg) monotherapy or camrelizumab (200 mg, day 8) combined with decitabine (10 mg/day, days 1–5) every 3 weeks.
Results With a median follow-up of 34.5 months, complete remission was 79% (95% CI 63% to 90%) in the decitabine-plus-camrelizumab group versus 32% (95% CI 13% to 57%) in the camrelizumab group (p=0.001). Median duration of response was not reached in the decitabine-plus-camrelizumab group, with an estimated 63% (95% CI 46% to 75%) of patients maintaining a response at 24 months. Median PFS with decitabine-plus-camrelizumab therapy was 35.0 months (95% CI not reached) and 15.5 months (95% CI 8.4 to 22.7 months) with camrelizumab monotherapy (HR, 0.46; 95% CI 0.21 to 1.01; p=0.02). Female gender, lower tumor burden, and fewer previous therapies were favorable prognostic factors for durable remission with camrelizumab monotherapy. The PFS benefits of decitabine-plus-camrelizumab versus camrelizumab were observed in most subgroups, especially in patients with relative larger tumor burdens and those treated with ≥3 prior therapies. After decitabine-plus-camrelizumab treatment, the percentage increase of circulating peripheral central memory T-cells correlated with both improved clinical response and PFS, suggesting a putative biomarker of decitabine-plus-camrelizumab therapy for cHL.
Conclusions Decitabine-plus-camrelizumab results in longer PFS compared with camrelizumab alone in patients with relapsed/refractory cHL.
Trial registration numbers NCT02961101 and NCT03250962.
- immunotherapy
- drug therapy
- combination
- clinical trials
- phase II as topic
- t-lymphocytes
Data availability statement
Data are available upon reasonable request. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Programmed death-1 (PD-1) blockade therapy has been approved and recommended for both the treatment of patients with classical Hodgkin lymphoma (cHL) who have relapsed or progressed after autologous stem cell transplantation (ASCT) with brentuximab vedotin (BV), as well as for patients with relapsed/refractory cHL who are ineligible for transplantation.1 In fact, in patients with relapsed/refractory cHL who failed both ASCT and BV, anti-PD-1 antibodies have an objective response rate (ORR) of 65%–87%, but complete remission (CR) occurs in only 9%–22% of patients.2–5 Despite a high objective response to anti-PD-1, most patients eventually relapse with a median progression-free survival (PFS) of 11–15 months, and a long-term duration of response (DOR) only evident in a few patients.6–8 Clinical trials are in progress to evaluate new anti-PD-1-based combination therapies and to incorporate immunotherapy into earlier lines of treatment.9 10 Pembrolizumab, for example, has been employed in a post-ASCT consolidation treatment role with an estimated 18-month PFS rate of 82% in patients with relapsed/refractory cHL after frontline therapy.11 In addition, the combination of BV and nivolumab was proposed as an initial salvage therapy followed by ASCT, resulting in a CR rate of 61%.12
ASCT is the standard of care for second-line therapy in most patients with relapsed/refractory cHL. However, a number of patients are considered ASCT ineligible or have refused ASCT. Moreover, BV is not currently approved in some countries. Of those patients with relapsed/refractory cHL who have received ≥2 prior lines of systemic therapy, fewer than 10% have also been given BV while 32%–34% achieved CR with single-agent anti-PD-1 camrelizumab or sintilimab.13 14 Since the degree of clinical response might be linked to response durability, novel anti-PD-1 combination therapies are needed to achieve both higher CR rates and longer lasting remissions. This would be especially pertinent in patients unsuited for or recalcitrant to ASCT, as well as in those who have received multiple chemotherapy regimens.
Both genetic and epigenetic alterations influence the antitumor immune response.15–17 De novo DNA methylation programs promote terminal T cell exhaustion, and the fully exhausted T cells are refractory to PD-1 blockade-mediated rejuvenation. Inhibiting de novo methylation by agents targeting DNA methyltransferase (DNMT) can increase T cell responses and tumor control during PD-1 inhibitors in mice.18 19 DNMT inhibitor decitabine was initially used and regarded as a cytotoxic drug, but the intolerable toxicity limited its application. Nowadays, based on the DNA demethylation capacity of decitabine, a low dose 5-day regimen (100–135 mg/m2/cycle) has been recommended in hematological malignancies and an even lower dose (50–90 mg/m2/cycle) has been suggested as the “optimal dose” for the combination therapy of solid tumors.20–22 We conducted a two-arm, open-label, randomized phase II clinical trial in patients with relapsed/refractory cHL who failed ≥2 lines of prior therapies without a history of anti-PD-1 treatment. Using a total of 50 mg per cycle of decitabine, a higher CR rate with decitabine-plus-anti-PD-1 antibody camrelizumab compared with camrelizumab alone was reported.14 This study demonstrated a significant improvement in the 6-month PFS rate (100% with decitabine-plus-camrelizumab vs 79% with camrelizumab).14 Herein, we also present response durability in the trial population after a median follow-up of 34.5 months, investigate factors associated with CR on anti-PD-1 camrelizumab monotherapy, and explain the advantages of decitabine-plus-camrelizumab combination. Moreover, we evaluate putative biomarkers of clinical outcomes for decitabine-plus-camrelizumab.
Methods
Patients and treatment
Our study design and patient eligibility criteria have been previously reported.14 Eligible patients were 12 years of age or older, had measurable histologically confirmed relapsed/refractory cHL, an Eastern Cooperative Oncology Group performance-status of 0 or 1, and had previously received at least two or more lines of antitumor therapy while maintaining adequate hematological, hepatic, renal, pulmonary, and cardiac function. Here, we report data from patients clinically naïve to anti-PD-1 therapy. These patients were randomly assigned 1:2 to either camrelizumab (200 mg) alone or a combination of camrelizumab (200 mg, day 8) plus decitabine (10 mg/day, days 1–5), every 3 weeks. Treatment continued until confirmed disease progression, unacceptable toxicity occurred, or until a patient decided to quit the trial. Investigators could discontinue therapy in any patient with 1 year or more of sustained CR. Patients with unconfirmed disease progression could continue treatment until disease progression was clinically confirmed. All histologies were read by two pathologists.
PFS, DOR, tumor response, and safety assessments
PFS was defined as the time from initial dosing to the first documentation of disease progression or death, whichever occurred first. DOR was defined as the time from the first documented response to disease progression or death in patients who achieved either a partial or complete response. Tumor response was assessed at baseline and then every 6 weeks by ultrasound or CT, as well as at baseline and every 12 weeks by fluorine-18 deoxyglucose (18F-FDG) positron emission tomography (PET)/CT. CR assessment was confirmed by PET/CT with a Deauville score ≤3 considered to be indicative of a complete metabolic response, according to the Revised Response Criteria for Malignant Lymphomas (RRC, 2014 Lugano classification).23 24 After treatment discontinuation, PET/CT was performed every 3–6 months for survival evaluation. Adverse events (AEs) were graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 4.0. The biomarker evaluation was conducted as an exploratory analysis, to measure the percentage change in peripheral memory T cells with decitabine-plus-camrelizumab treatment versus camrelizumab alone (online supplemental methods). Blood samples were collected before each of the first five treatment cycles (Cnd0, C1d0 indicates baseline), and on day 6 following decitabine infusions in cycle 1. Blood collected was labeled with antibodies against CD8, CD4, CD45RA, CCR7, and flow cytometry data were acquired on a BD FACS Caliber instrument.
Supplemental material
Statistical analysis
The CR rates were compared between two treatment groups with two-sided 95% exact binomial CIs calculated using the Clopper-Pearson method. The efficacy evaluation was conducted in the randomized (intention-to-treat) population. Safety analyses were performed in patients who received at least one dose of treatment. Kaplan-Meier estimates were performed for analyses of PFS and DOR. Patients who were alive without disease progression or lost to follow-up were censored. The stratified log-rank test was used to detect differences between subgroups in PFS. The HRs for the decitabine-plus-camrelizumab group compared with the camrelizumab alone group as well as any associated 95% CIs were estimated using a log-rank model. A two-way repeated-measures analysis of variance was conducted to evaluate the effect of time–group interaction. The significance level was set at p<0.05.
Results
Patients
Between January 2017 and July 2018, 61 patients were randomized to receive either camrelizumab (n=19) or decitabine-plus-camrelizumab (n=42). Patient demographics and characteristics have been previously reported, and baseline characteristics were balanced between the two treatment groups.14 Briefly, 61 patients (48% relapsed; 52% refractory) with cHL were enrolled. The median time from initial cHL diagnosis to first dose in this study was 2.0 years (range, 0.5–12 years), and 64% of patients had extranodal disease at enrollment, with a median SPD (sum of the products of diameters) of 20 cm2 (table 1). Seventeen patients (28%) relapsed or progressed after ASCT, and the other 44 patients were ineligible for ASCT because of chemoresistance (31 patients), comorbidities (5 patients), and other factors (8 patients). Fewer than 10% of patients had prior BV treatment due to its unavailability in China.
Baseline demographics and disease characteristics
At data cut-off on November 8, 2020, in the decitabine-plus-camrelizumab group, 16 patients (38%) discontinued combination therapy due to disease progression, 15 patients (36%) completed treatment after having ≥1 year of sustained CR, and 8 patients (19%) remained on treatment. In the camrelizumab monotherapy group, 10 patients (53%) discontinued camrelizumab due to disease progression, 6 patients completed treatment, and none remained on treatment (figure 1). Patients who completed treatment did not receive any additional therapy until disease progression.

Consolidated Standards of Reporting Trials diagram. CR, complete remission.
Duration of response
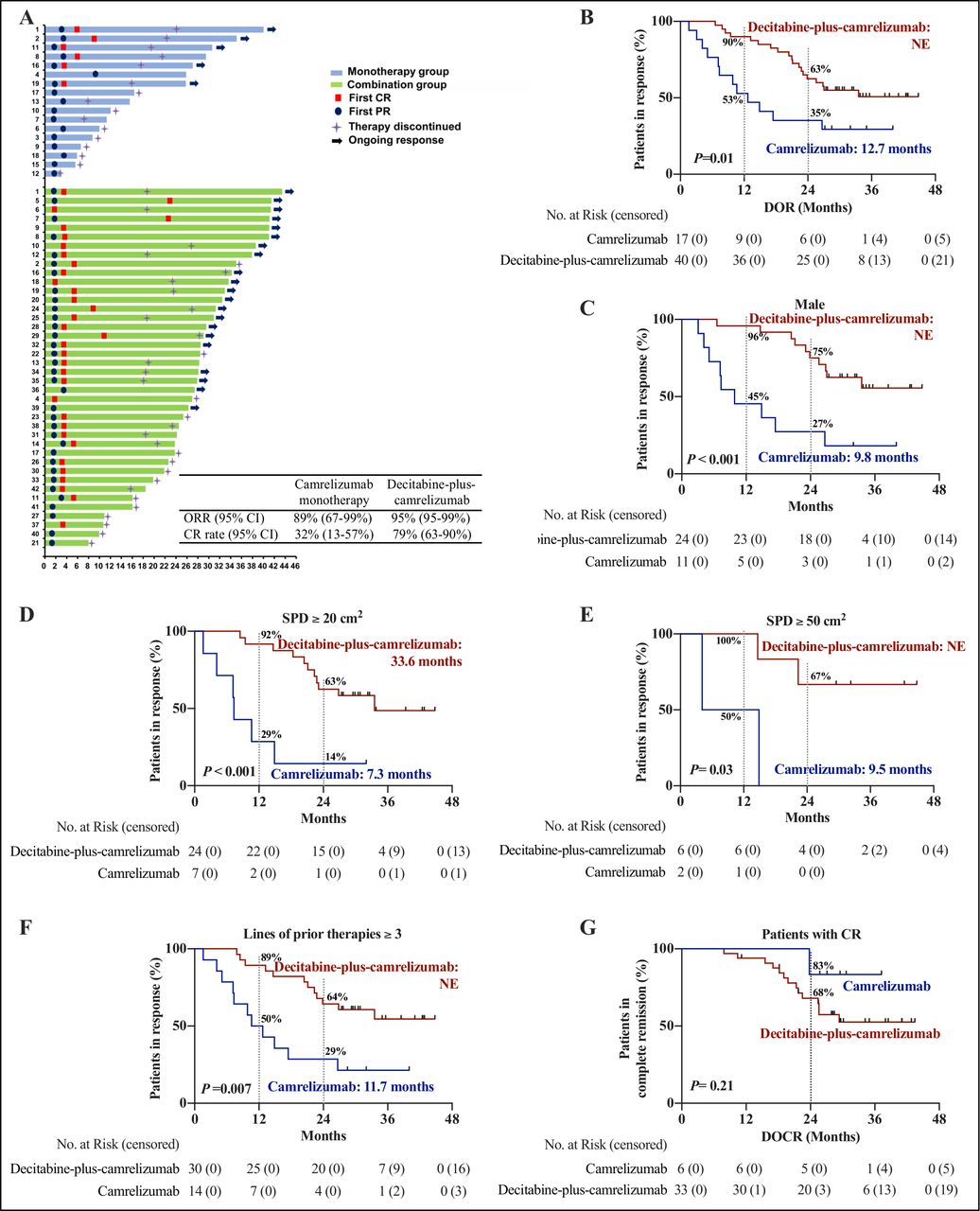
As of last follow-up, the ORR by intent-to-treat analysis was 89% (32% CR) with camrelizumab monotherapy compared with 95% (79% CR) with the decitabine-plus-camrelizumab combination (p<0.001). Importantly, additional patients achieved CR in the decitabine-plus-camrelizumab group after prolonged therapy with two patients acquiring CRs in their second year of decitabine-plus-camrelizumab treatment. Thus, our CR rate is higher than previously reported14 (figure 2A). A significantly higher CR rate with decitabine-plus-camrelizumab treatment was observed across most demographic and clinical subgroups compared with camrelizumab alone, independent of disease stage, extranodal involvement, and tumor burden at enrollment. This includes those with prior ASCT or ≥3 lines of prior therapies (online supplemental table 1).

DOR in patients with CR and PR. (A) Response onset and duration for all responders. Blue bars indicate patients in the camrelizumab group and green bars indicate patients in the decitabine-plus-camrelizumab group. The length of the bar shows the time from first dosing until the patient had a CR or PR, along with the duration of the response. The onset of first response (CR or PR) was indicated as a red square (CR) or blue dot (PR), respectively. (B) Kaplan-Meier estimates of DOR in patients with CR and PR. The red curves represent patients treated with decitabine-plus-camrelizumab and the blue those treated with camrelizumab monotherapy. The median DOR and DOR rates at 12 months and 24 months are shown. Plus signs indicate censored data. (C–F) Kaplan-Meier estimates of response duration in responders who were men (C), had tumor burden SPD ≥20 cm2 (D), SPD ≥50 cm2 (E), or with ≥3 lines of previous therapy (F). The red curves represent patients treated with decitabine-plus-camrelizumab and the blue those treated with camrelizumab monotherapy. The median DOR and DOR rates at 12 months and 24 months are shown. Plus signs indicate censored data . (G) Kaplan-Meier estimates of CR duration in patients who acquired a CR after decitabine-plus-camrelizumab or camrelizumab monotherapy. The red curves represent patients treated with decitabine-plus-camrelizumab and the blue those treated with camrelizumab monotherapy. The median duration of CR was not reached and duration of CR rate at 24 months is shown. Plus signs indicate censored data. CR, complete remission; DOCR, duration of complete remission; ORR, objective response rate; PR, partial response; SPD, sum of the products of diameters.
Patients have been followed for a median of 34.5 months (range, 28.4–42.3 months) from first dosing in this study. Among patients who achieved a PR or CR, the median DOR was not reached in the decitabine-plus-camrelizumab group and 12.7 months (95% CI 5.9 to 19.5 months) in the camrelizumab monotherapy group (HR, 0.40; 95% CI 0.17 to 0.97; p=0.01), with 2-year response duration rates of 63% (95% CI 75% to 46%) and 35% (95% CI 57% to 14%), respectively (figure 2B).
In camrelizumab monotherapy group, five patients who achieved a CR remained in remission. By comparing their baseline characteristics with the other 12 responders who later had progressive disease or withdrew from the study, we observed that female patients with smaller tumor burdens (lower median SPD) who had received fewer previous lines of therapy at enrollment seemed to achieve a longer lasting remission with camrelizumab treatment (online supplemental table 2). Strikingly, among male patients, who had relative larger tumor burdens (SPD over 20 cm2), or among those who relapsed/progressed after three or more previous systemic therapies, there were significant DOR benefits with decitabine-plus-camrelizumab combination compared with camrelizumab alone (figure 2C-F). Nearly two-thirds of patients who had an SPD ≥20 cm2 or ≥30 cm2 or ≥50 cm2 achieved response duration at 2 years after decitabine-plus-camrelizumab treatment, while no more than 20% of patients documented a response with camrelizumab alone (figure 2D,E, online supplemental figure 1). The combination therapy had both a higher CR rate and longer response duration compared with anti-PD-1 monotherapy, and we observed that the response duration in patients with CRs from the two treatment groups seemed comparable (figure 2G).
Progression-free survival
The median PFS was 35.0 months (95% CI not reached) in the decitabine-plus-camrelizumab group, as compared with 15.5 months (95% CI 8.4 to 22.7 months) in the camrelizumab group (HR, 0.46; 95% CI 0.21 to 1.01; p=0.02) (figure 3A). Two-year PFS rates on decitabine-plus-camrelizumab and camrelizumab monotherapy were 67% (95% CI 79% to 50%) and 42% (95% CI 62% to 20%), respectively. Patients with relative larger tumor burdens, such as those with SPD ≥20 cm2, ≥30 cm2 or ≥50 cm2, had 2-year PFS rates with decitabine-plus-camrelizumab treatment of 71% (95% CI 85% to 48%), 72% (95% CI 87% to 46%), and 67% (95% CI 90% to 19%), respectively. In contrast, the median PFS of the corresponding patient subsets (SPD ≥20 cm2, ≥30 cm2, or ≥50 cm2) on camrelizumab monotherapy was 10.0, 12.0, and 11.0 months, respectively (figure 3B and online supplemental figure 2). The benefits of combination treatment with respect to PFS were observed in other analytical subgroups, including patients who were men, ≥28 years old, patients with tumor SPD >20 cm2, and those who had previous ASCT or who were treated with three or more previous therapies (figure 3C).
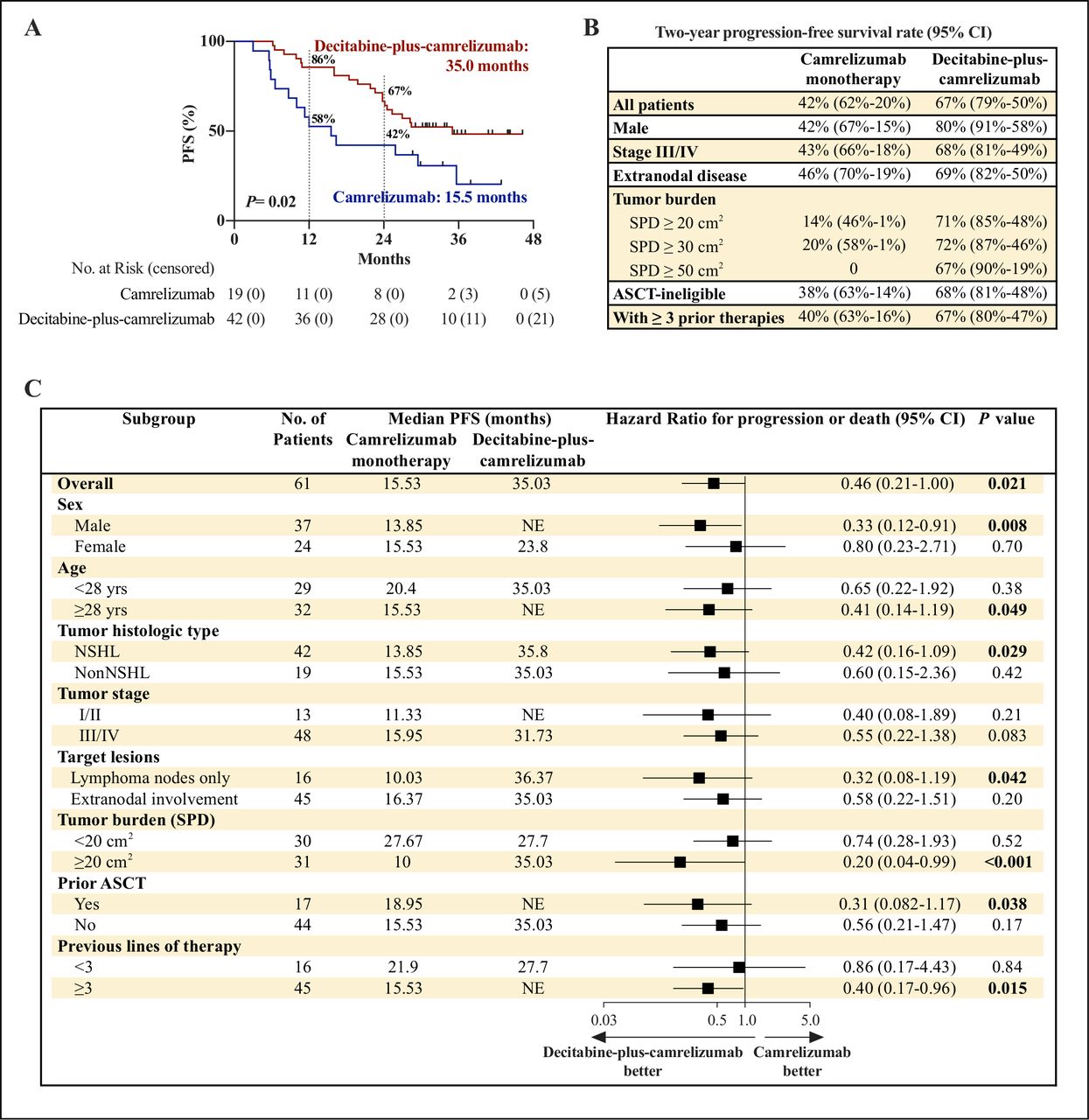
PFS analysis. (A) Kaplan-Meier estimates of PFS in all evaluable 61 patients. The red curves represent patients treated with decitabine-plus-camrelizumab and the blue those treated with camrelizumab monotherapy. The median PFS and PFS rates at 12 months and 24 months are shown. Plus signs indicate censored data. (B) Two-year PFS rates in patient subgroups according to baseline characteristics. (C) Forest plot of median PFS for patient subgroups according to baseline demographics and disease characteristics indicating favored treatment of each subgroup. ASCT, autologous stem cell transplantation; PFS, progression-free survival; SPD, sum of the products of diameters.
Putative biomarkers
In line with low-dose decitabine’s role as a DNA demethylating agent, we detected a reduced level of global DNA methylation in peripheral blood mononuclear cells from patients after decitabine-plus-camrelizumab therapy, and the methylation of LINE-1 repetitive elements were not changed in patients with camrelizumab monotherapy (online supplemental figure 3A,B). Considering the critical role of T-cell memory for durability of antitumor immunotherapy, we next used Fluorescence Activating Cell Sorter (FACS) by labeling CD45RA and CCR7 to quantitatively assay circulating naïve T-cells (Tnaive, CCR7+CD45RA+), central memory T-cells (Tcm, CCR7+CD45RA−), effector memory T-cells (Tem, CCR7−CD45RA−), and terminally differentiated effector memory T-cells (Ttemra, CCR7−CD45RA+) during treatment (figure 4A,B). We observed a prominent incremental increases in circulating CCR7+CD45RA− Tcm cells as a percentage of CD8+ or CD4+ cells following decitabine-plus-camrelizumab combination therapy compared with baseline levels (CD8+ Tcm, p<0.001; CD4+ Tcm, p=0.004), and there was a significant difference in the increase of CD8+ Tcm between the camrelizumab monotherapy and decitabine-plus-camrelizumab therapy (figure 4C,D). This was especially evident in patients who acquired a CR in the decitabine-plus-camrelizumab group (figure 4E,F). No significant effects on Tcm cells were observed in patients in the camrelizumab monotherapy group (figure 4G,H). In addition, the frequency of CD8+ naïve T-cells was markedly increased after decitabine-plus-camrelizumab treatment (p<0.001), while there were no significant differences in the ratio alteration of Tnaive, Tem, or Ttemra cells between the two groups (online supplemental figure 3C–H).
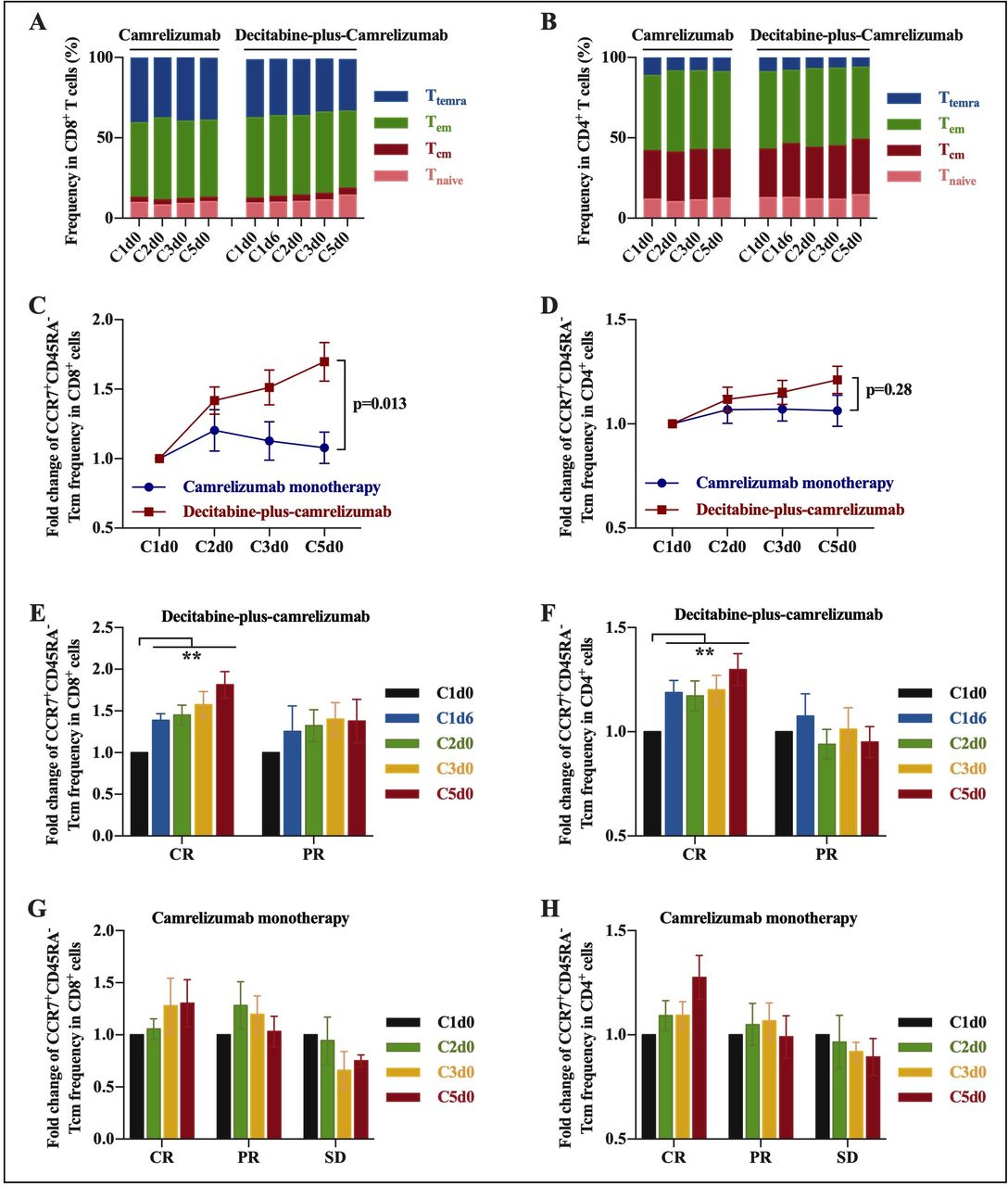
Fold change of percentages in peripheral T-cell subsets during decitabine-plus-camrelizumab or camrelizumab treatment. Peripheral blood was collected from patients at the indicated times (Cnd0 indicates before the treatment cycle, n refers to treatment cycle; C1d6 indicates the day following 5-day decitabine administration in cycle 1). (A, B) Percentages of peripheral CCR7+CD45RA+ Tnaïve, CCR7+CD45RA− Tcm, CCR7−CD45RA− Tem, and CCR7−CD45RA+ Ttemra cells in CD8+ (or CD4+) T-cells at the indicated times in the camrelizumab group or decitabine-plus-camrelizumab group, analyzed by FACS. (C, D) Fold change of percentages of peripheral CCR7+CD45RA− Tcm cells in CD8+ (or CD4+) T-cells at the indicated times compared with baseline (C1d0) in the camrelizumab group or decitabine-plus-camrelizumab group, analyzed by FACS. The two-way repeated-measures analysis of variance was conducted to evaluate the effect of time–group interaction, and p value was shown. (E, F) Fold change of percentages of peripheral CCR7+CD45RA− Tcm cells in CD8+ (or CD4+) T-cells at the indicated times compared with baseline (C1d0) among patients who had different clinical responses after decitabine-plus-camrelizumab treatment. (G, H) Fold change in percentages of CCR7+CD45RA− Tcm cells in CD8+ (or CD4+) T-cells at the indicated times compared with baseline (C1d0) among patients who had different clinical responses after camrelizumab treatment. Data represent the mean±SEM. *p<0.05; **p<0.01. CR, complete response; NSHL, Nodular Sclerosis Hodgkin Lymphoma; PR, partial response; SD, stable disease.
Baseline percentages of peripheral CD8+ and CD4+ T-cell subsets were comparable between the two treatment groups, and were not significantly associated with clinical response, except that patients with relative lower frequency of CD4+ Tcm cells had a higher CR rate compared with those with higher CD4+ Tcm levels in decitabine-plus-camrelizumab group (online supplemental tables 3 and 4). Notably, patients who had an increase in their percentage of Tcm, but not other T-cell subsets, following decitabine-plus-camrelizumab therapy as detected on C5d0 (the day before cycle 5 infusion) were more likely to have CRs (CD8+ Tcm, p=0.005; CD4+ Tcm, p=0.03) (figure 5A). The treatment of decitabine increased Tcm levels as detected on C1d6 (day 6 in the first cycle), and also was an indicator of patients likely to achieve a CR (CD8+ Tcm, p=0.02; CD4+ Tcm, p=0.023). Consistently, patients with elevated ratio of peripheral CD8+ or CD4+ Tcm cells after decitabine-plus-camrelizumab therapy had significantly longer PFS compared with those without an increase in Tcm ratios, as detected on C1d6 or C5d0 (figure 5B–E). The baseline level of Tcm, as well as baseline and on treatment ratio increase of peripheral Tem, Ttemra, or Tnaïve cells, were not significantly correlated with PFS following decitabine-plus-camrelizumab therapy (online supplemental figures 4A–H and 5A–F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association of percentage alteration in peripheral T-cell subsets with CR rate and PFS. (A) The percentage of peripheral CCR7+CD45RA− Tcm, CCR7−CD45RA− Tem, CCR7+CD45RA+ Tnaïve, and CCR7−CD45RA+ Ttemra cells in CD8+ (or CD4+) T-cells detected at C5d0 or C1d6 as compared with baseline (C1d0) with CR rate in patients after camrelizumab monotherapy or decitabine-plus-camrelizumab combination. C1d6 indicates day 6 (after 5-day decitabine treatment) in the first cycle, C5d0 indicates the day before the fifth cycle. (B–E) PFS among subgroups according to CCR7+CD45RA−CD8+, CCR7+CD45RA−CD4+ ratios detected on C5d0 or C1d6 compared with baseline with decitabine-plus-camrelizumab therapy. A p value <0.05 was considered to indicate statistical significance. CR, complete response; PFS, progression-free survival.
Safety
The most common treatment-related AEs were clinically inconsequential including reactive capillary endothelial proliferation (RCEP; 86% on combination therapy and 84% on monotherapy), a benign and reversible skin condition, and leukocytopenia (62% on combination treatment and 32% on monotherapy). The RCEP had morphological characteristics of the “red-nevus-like” or “pearl-like” pattern, most commonly appeared in the skin, and was all grade 1 or grade 2. RCEP occurred during week 3 to week 9, and complete regression of RCEP lesions was observed at a median of 15 weeks (range, 12–36 weeks) spontaneously. Grade 3 or higher treatment-related AEs occurred in 21% of patients with decitabine-plus-camrelizumab combination and 16% of patients with camrelizumab monotherapy. Grade 3–4 leukocytopenia was observed in nine patients in the decitabine-plus-camrelizumab group, the hematological toxicity was relieved itself after 1 week treatment delay and none of these patients received granulocyte colony-stimulating factor therapy, and no treatment-related infections were identified. This safety profile was consistent with our previous study,14 and the incidence and severity of AEs did not change after long-term follow-up (table 2). All of the 61 patients were alive. No treatment-related deaths occurred. The most frequent immune-related AEs in patients who received decitabine-plus-camrelizumab were rash (12%), diarrhea (10%), myalgia (10%), and hypothyroidism (7%); and the most frequent immune-related AEs in the camrelizumab monotherapy group were hypothyroidism (16%) and pneumonitis (5%) (online supplemental table 5).
Treatment-related adverse events of any grade in 5% or more in the overall population of 61 patients
Discussion
In patients with relapsed/refractory cHL, PD-1 blockade monotherapy induced a long-lasting remission in some patients, mostly women with smaller tumor burdens who had fewer lines of previous therapies. In male patients with tumor SPD ≥20 cm2 or in those had three or more lines of previous therapy, the median DOR with single-agent camrelizumab was less than 1 year. Notably, the combination of decitabine and camrelizumab therapy was tolerable and had significantly longer response duration with 63%–75% of patients remaining in response after 2 years.
Among patients with relapsed/refractory cHL following ASCT and BV, PD-1 blockade therapy had a median PFS of 11–15 months, while most patients suffered disease progression or a relapse within 2 years on anti-PD-1 monotherapy.6-8 In our study, patients who progressed after ASCT had a median PFS on decitabine-plus-camrelizumab that was not reached, and this was longer than that in patients on camrelizumab monotherapy. However, less than 10% of patients in our study had previous BV therapy, and the efficacy of decitabine-plus-camrelizumab in patients who progressed or relapsed after ASCT and BV cannot be determined. Several anti-PD-1 combination therapies have been tried in an attempt to achieve better clinical outcomes.11 12 Anti-PD-1 combined with BV is now used as the first salvage therapy after transplantation for patients with relapsed/refractory disease, and it has proven to be potentially efficacious.12 In a phase I/II trial, patients who had relapsed after at least one line of therapy, which included 34% who had prior ASCT, received a combination therapy of BV with ipilimumab, nivolumab, or triplet therapy. The 1 year PFS was 61% in the BV-plus-ipilimumab group, 70% in the BV-plus-nivolumab group, and 80% in the triplet therapy group.25 By contrast, the 1-year PFS rate with decitabine-plus-camrelizumab therapy was 86%, which was comparable to that of BV-combined anti-PD-1 immunotherapy. Thus, decitabine-plus-camrelizumab combination may be an extremely effective regimen for patients with relapsed/refractory cHL who progressed/relapsed after ASCT, especially if they had no access to BV therapy. For the BV-treated patients, decitabine-plus-camrelizumab might also be an option since that the patient who had previous BV therapy achieved a CR and had an ongoing response for more than 3 years after decitabine-plus-camrelizumab therapy.
For patients with relapsed/refractory cHL who are ineligible for ASCT, whose treatment options are limited and who have a poor prognosis, the combination of BV and PD-1 blockade therapy has demonstrated improved clinical outcome.26 For patients with relapsed/refractory cHL who progressed after salvage chemotherapy with BV, and who were ineligible for ASCT (cohort 2) in the Keynote 087 study, pembrolizumab treatment resulted in a median PFS of 11.1 months and a 2-year PFS rate of 18.2%. Pembrolizumab also resulted in 2-year PFS rates of 41.6% and 35.7% in patients who progressed after ASCT with (cohort 1) and in those without BV (cohort 3), respectively.8 Two phase III clinical trials comparing pembrolizumab to BV or nivolumab-plus-BV to BV in patients with relapsed/refractory cHL who were ineligible for ASCT or failed ASCT (NCT02684292 and NCT03138499) are ongoing. In this current study, the 2-year PFS rate of decitabine-plus-camrelizumab in ASCT-ineligible patients was 68% versus 38% in the camrelizumab group. Bulky disease at diagnosis, extranodal disease, first CR duration of <1 year, and a prolonged interval from time of diagnosis to transplantation were seemingly inversely related to long-term survival rates after ASCT.27 28 We found that in patients with a relatively larger tumor burden (tumor SPD ≥20 cm2), and in those who had ≥3 previous therapies, decitabine-plus-camrelizumab combination produced a significantly greater clinical response and response durability compared with camrelizumab alone.
The benefits in DOR and PFS from the addition of decitabine to PD-1 blockade therapy might also be associated with a higher CR rate since patients who attained a CR on the combination therapy had a longer response duration than those with a PR. A total of 39 patients in our study achieved CRs, of whom 21 patients had 1 year or more of long-lasting CRs and discontinued treatment, including 15 after decitabine-plus-camrelizumab and 6 after camrelizumab monotherapy. Eight patients on combination therapy are still on treatment. As of data cut-off in November 2020, 12 patients in the decitabine-plus-camrelizumab group and 5 patients in the camrelizumab group have had a durable remission that has allowed discontinuation of all drugs after the first year without the initiation of any new treatment including ASCT therapy. Since several patients with CR are still on treatment, we do not know what proportion of patients may derive a potential cure with camrelizumab-based immunotherapy. Longer term follow-up observation is necessary. Additionally, we noticed that a small number of patients who acquired a CR with decitabine-plus-camrelizumab had a short duration of their response, and that the duration of their CR was not significantly different than in patients receiving camrelizumab alone. We anticipate that novel optimized epigenetic-immunotherapy regimens may attain a longer lasting response in even more patients with relapsed/refractory cHL.
To investigate putative biomarkers for predicting the clinical response to decitabine-plus-camrelizumab, we showed that the percentage increase in peripheral T central memory cells with combination therapy was directly associated with CR and prolonged PFS. Importantly, these T central memory cells can be detected and monitored as early as day 6 of the first cycle. Additionally, in camrelizumab monotherapy group, patients with increased CD8+ Tcm ratio on C5d0 might probably acquire a CR while not significantly (p=0.13, figure 5A); and also had longer PFS compared with those without an increase in Tcm ratio (p=0.2, online supplemental figure 5G,H). Exhausted T cells, including memory-like exhausted T cells that respond to PD-1 inhibitors, belong to a unique heterogeneous T-cell subset that ultimately differentiates into terminal exhausted T cells, which are by and large resistant to anti-PD-1-induced rejuvenation but can still exhibit distinct epigenetic profiles of memory-like exhausted T cells.29–31 Low-dose DNA demethylating agents can modulate a T-cell’s epigenetic status and enhance the anti-tumor activity of PD-1/PD-L1 blockade therapy in mice models.19 32 Our results suggest the importance of decitabine-mediated T-cell reprogramming during PD-1 blockade therapy. Nevertheless, whether decitabine treatment promotes Tcm cells expansion of healthy cells or protects from apoptosis is not clear. In addition, further validation in larger studies regarding the use of circulating Tcm alterations as a function biomarker for response to decitabine-plus-camrelizumab is needed. Finally, the detailed mechanism underlying the improved efficacy of decitabine-combined anti-PD-1 in relapsed/refractory cHL is worthy of further investigation.
In conclusion, decitabine-plus-camrelizumab was well-tolerated and showed improved clinical outcomes in patients with relapsed/refractory cHL. After a median follow-up of 34.5 months, there was a notable DOR and PFS benefit with decitabine-plus-camrelizumab compared with camrelizumab alone. This advantage of decitabine-plus-camrelizumab was evident widely among cHL patients, especially in those with relative large tumor burden, and in those who progressed after ASCT or who were ineligible for transplantation.
Data availability statement
Data are available upon reasonable request. The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Ethics approval
The study was performed in accordance with the ethical principles of Good Clinical Practice, the Declaration of Helsinki, and applicable local regulatory requirements. The protocol was approved by the institutional review board of the Chinese PLA General Hospital (S2016-127-01). All patients provided written informed consent.
Acknowledgments
The authors are grateful for the nurses and staff in the Department of Bio-therapeutic at the First Medical Centre in the Chinese PLA General Hospital.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
YL, CW, XL and LD contributed equally.
JN and WH contributed equally.
Contributors CW, MC, LD, XL, FS, and JL were involved in the acquisition of data. JN, YL, ML, and QM were involved in analysis and interpretation of data. JN and MB were involved in writing and revision of the manuscript. WH and QY were involved in supervision. All authors read and approved the final manuscript.
Funding This work was funded under the auspices of the National Key Research and Development Program of China (2019YFC1316205 to JN), National Natural Science Foundation of China (31991171, 81872479, 31870873, 81830002, 82022057, 81903153 and 81803071), and with Fostering Funds from the Chinese PLA General Hospital’s National Excellent Young Scholar Science Fund (2017-YQPY-001, 2020-JQPY-001).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.