Article Text

Abstract
SARS-CoV-2 infection and the resulting COVID-19 have afflicted millions of people in an ongoing worldwide pandemic. Safe and effective vaccination is needed urgently to protect not only the general population but also vulnerable subjects such as patients with cancer. Currently approved mRNA-based SARS-CoV-2 vaccines seem suitable for patients with cancer based on their mode of action, efficacy, and favorable safety profile reported in the general population. Here, we provide an overview of mRNA-based vaccines including their safety and efficacy. Extrapolating from insights gained from a different preventable viral infection, we review existing data on immunity against influenza A and B vaccines in patients with cancer. Finally, we discuss COVID-19 vaccination in light of the challenges specific to patients with cancer, such as factors that may hinder protective SARS-CoV-2 immune responses in the context of compromised immunity and the use of immune-suppressive or immune-modulating drugs.
- vaccination
- review
- immunogenicity
- vaccine
- immunity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Based on compelling efficacy and safety data, vaccines against SARS-CoV-2 have been approved by regulatory agencies of an increasing number of countries worldwide. Because patients with malignancies were excluded from most trials that tested SARS-CoV-2 vaccines, data on safety, tolerability and efficacy in this vulnerable patient population are currently scant. Multiple studies have shown that patients with cancer have an increased risk of morbidity and mortality from COVID-19, including a 30-day mortality of 30% in hospitalized patients with COVID-19 and cancer compared with 21% in those without cancer.1 2 Consequently, the benefits of SARS-CoV-2 vaccination are likely to substantially outweigh the potential risks of vaccine-related adverse events; hence, patients with cancer should be considered a high-priority subgroup for COVID-19 vaccination, including those participating in clinical trials of cancer therapeutics. Potential (temporary) exception from vaccination might apply to patients undergoing stem cell transplantation or adoptive cell therapy, in agreement with the general recommendations of delaying vaccination following highly immunosuppressive therapies. Herein, we provide an overview of mRNA-based vaccines including their safety and efficacy. Extrapolating from insights gained from a different preventable viral infection, we review existing data on immunity against influenza A and B vaccines in patients with cancer. In addition, we discuss COVID-19 vaccination in light of the challenges specific to patients with cancer, such as factors that may hinder protective SARS-CoV-2 immune responses in the context of compromised immunity and the use of immune-suppressive or immune-modulating drugs.
mRNA-based vaccination: a focus on SARS-CoV-2 mRNA vaccines
Advantages of in vitro transcribed mRNA vaccines
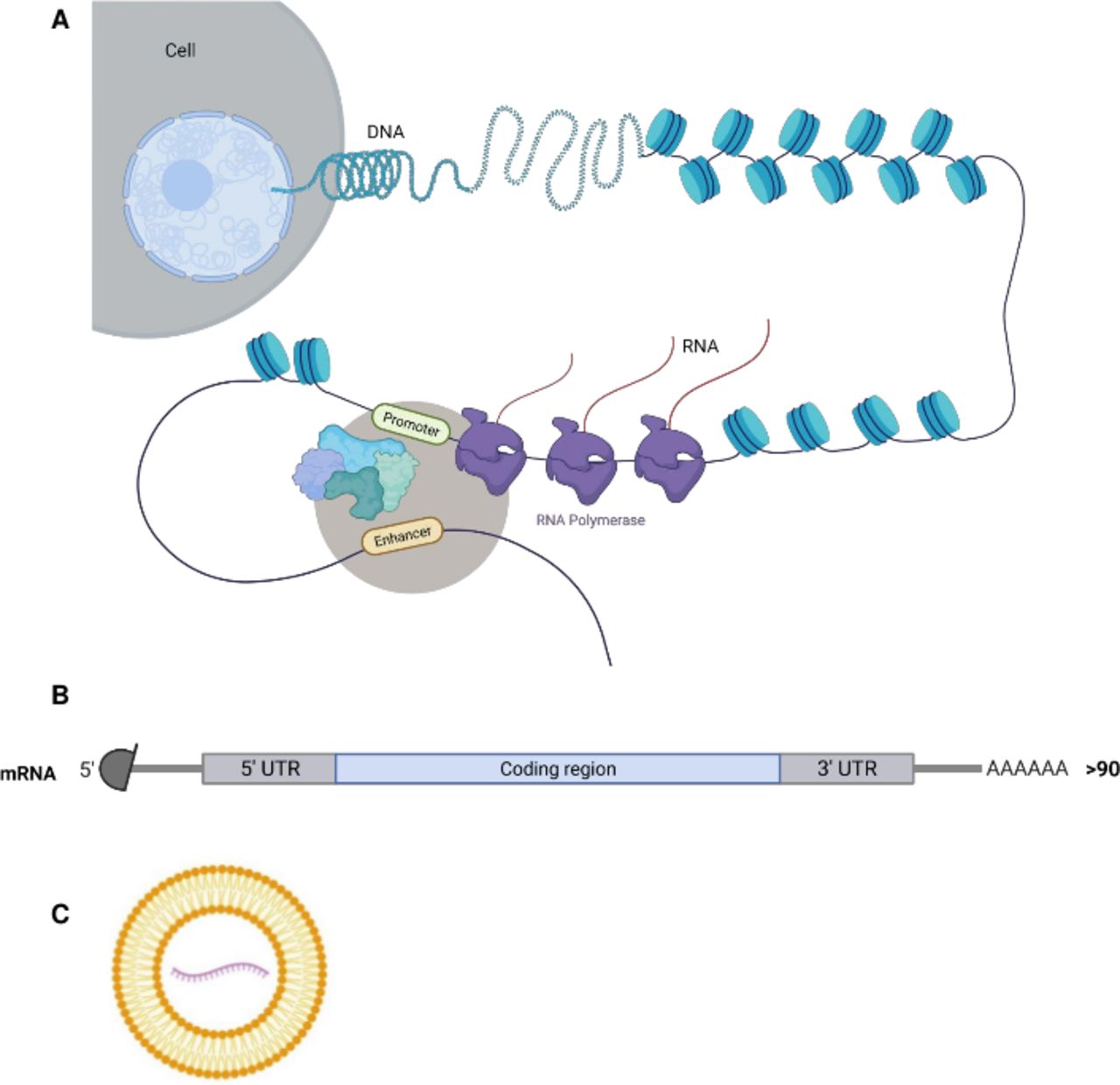
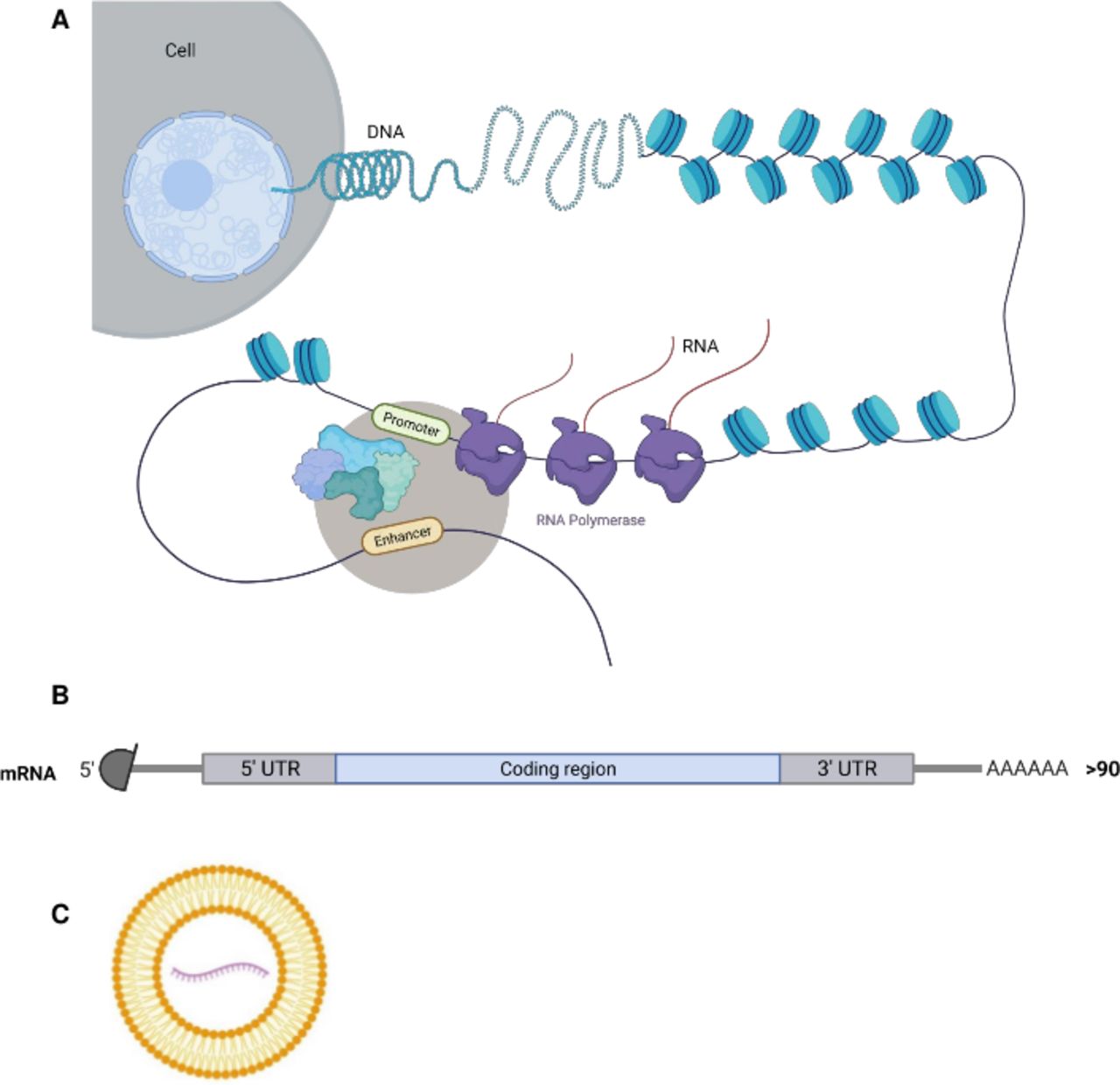
The main advantage of the non-replicating in vitro transcribed (IVT) mRNA vaccine is safety (figure 1). Notably, this natural molecule cannot replicate, is active in the cytosol (and not in the nucleus) and is rapidly and completely degraded by RNases abundantly present in cells, tissues and biological fluids. Thus, unlike recombinant adenoviruses and similar to proteins, there is no risk of persistence, recombination or alteration of the human genome with this vaccine format.3–7 Although they are quickly degraded in vivo, the mRNA molecules are extremely physicochemically stable in the absence of RNases in vitro. They can be frozen, thawed, lyophilized and resuspended.3 In fact, RNA is the only biological molecule that can be heated up to 95°C without losing its activity. Other biological molecules, including double-stranded DNA, protein, and also viruses, lose their functionality when heated up to 95°C. Thus, counterintuitively, mRNA is the most stable biological molecule for the production of vaccines. The liposomes currently used to make mRNA vaccines in order to optimize vaccine delivery are not as stable; this explains why available mRNA vaccines must be stored under low temperature.
{kind=link}
In vitro transcribed (IVT) mRNA-based vaccines. (A) The DNA in the nucleus is transcribed into mRNA by RNA polymerases. The same process is used for in vitro production of mRNA. The recognition of a specific promoter allows the transcription of the desired synthetic mRNA in vitro. (B) The mRNA structure (natural and synthetic) of eukaryotes consists of a 5′ Cap structure (7-methylguanosine linked from its 3′ with a triphosphate bond to the 5′ of the first nucleotide), a 5′ untranslated region (5′ UTR), the coding sequence starting with AUG and ending on a stop codon, and a 3′ UTR followed by a poly-A tail of usually more than 90 residues. (C) The SARS-CoV-2 IVT mRNA-based vaccines from Moderna and BioNTEch/Pfizer use a liposome-based delivery vehicle. (Note: This figure was generated using images from BioRender.)
Synthetic mRNA that can be purified easily and efficiently (if needed, highly purified by High Performance Liquid Chromatography (HPLC)8) only codes for a single antigen, which limits the risk of triggering immunity against irrelevant antigens, as is the case with proteins (ie, contaminants, misfolded proteins) or adenoviruses (vector proteins).
Another feature of the IVT mRNA vaccine is the speed and simplicity of its production: any DNA sequence preceded by an adequate promoter (usually from the bacteriophages T7 or SP6) is efficiently transcribed in vitro by the recombinant RNA polymerase (usually T7 or SP6) .1 Over 1000 molecules of mRNA are produced in vitro from one molecule of DNA, within a few hours. All products of transcription (DNA, RNA polymerase, nucleotides) are of bacterial or chemical origin. Thus, the IVT mRNA is vegan. In addition to easing religious or philosophical issues, this feature also reduces the risks of allergies or the development of immune responses to contaminants from cell cultures.
History of the IVT mRNA vaccine
The prejudice in the scientific and medical communities that mRNA is unstable has largely hindered the development of mRNA-based drugs over the last 20 years. The SARS-CoV-2 pandemic in 2020 provided a final turnaround of this misconception and allowed mRNA vaccines to demonstrate their potential (ie, their rapid and easy production, safety and efficacy) and become the first vaccine format to be approved against SARS-CoV-2 infections, less than a year after the initial publication of the viral sequence.9 Although the use of IVT mRNA in vaccines is relatively new (first described in 1993, injected into Steve Pascolo8—a healthy volunteer that received the vaccine, then chief security officer and qualified person for good manufacturing practices production at CureVac—and patients with cancer in the mid-2000s,10–12 and first licensed in 2020), the use of mRNA for vaccination predates this by decades: the vaccines against yellow fever, mumps, measles and rubella are attenuated RNA viruses that function after subcutaneous injection by delivering their mRNA into host cells, which produce virus antigens and trigger an immune response. These long-standing vaccines are therefore ‘natural’ mRNA vaccines, while the newly approved anti-SARS-CoV-2 vaccines are ‘synthetic’ mRNA vaccines. However, both rely on the same basic mechanism: the production of viral proteins by human cells using injected mRNA. In the last 20 years, the optimization of IVT mRNA molecules and liposomal formulations have turned the IVT mRNA vaccine into a very potent format.9 13–15 Indeed, since 2003, IVT mRNA has been investigated in clinical trials, primarily as a vaccine format against malignancies.10–13 16 17
Anti-SARS-CoV-2 IVT mRNA vaccines
Experience with the earlier coronaviruses SARS-CoV and MERS-CoV has shown that the spike protein is present at the virus surface in a prefusion conformation and changes conformation after entering the infected cell. It was demonstrated that the substitution of lysine 986 and valine 987 with two consecutive prolines stabilizes the prefusion conformation. This so-called ‘PP-Spike’ induces neutralizing antibodies more efficiently than wild-type spike protein.18 The currently used vaccine IVT mRNA produced in vitro is in all cases coding for PP-Spike, whereas the AstraZeneca vaccine (AZD1222) codes for the wild-type spike, potentially explaining the difference in protection against variants between the mRNA vaccines and the AstraZeneca vaccine. It is condensed into liposomes, which are currently made of four different lipids and are related to a liposomal RNA formulation that was approved in 2018: the drug Patisiran (Onpattro), which is based on liposomal delivery of small inhibitory RNA (siRNA) for the treatment of a genetic neurological disease. This entails intravenous injection of 30 mg per dose every 3 weeks for the treatment of polyneuropathy due to hereditary transthyretin-mediated amyloidosis. In early 2020, five non-replicating mRNA vaccines were tested for vaccination against COVID-19: three from BioNTech (BNT162a1, made with unmodified nucleotides and BNT162b1 and BNT162b2, both containing pseudoUridine) in association with Pfizer, one from CureVac (CvNCoV, made with unmodified nucleotides) and one from Moderna (containing pseudoUridine). PseudoUridine modification abolishes the innate immune stimulation by RNA (ie, the triggering of Toll-like receptors),19 allowing the use of IVT mRNA for non-immunogenic (non-vaccine) protein expression. However, as reported in 2017, modified mRNA can also be used in mRNA vaccines (an observation that is currently not fully explained).20 Whether modified (pseudoUridine) or unmodified mRNA is best for an IVT mRNA vaccine is not yet clear (BioNTech has not yet published the results obtained with its unmodified mRNA vaccine, BNT162a1). Although the first injections of an anti-SARS-CoV-2 IVT mRNA vaccine (and the world’s first injection of an experimental anti-SARS-CoV-2 vaccine in humans) were performed in volunteers by Moderna in March 2020, the first approval of an anti-COVID-19 vaccine was for BioNTech’s mRNA vaccine (Comirnaty) in December 2020. BioNTech/Pfizer and Moderna mRNA vaccines provide over 90% protection against COVID-199 15 and also protect against the new variants (although neutralizing the variant identified in South Africa requires lower dilutions of sera than those used to neutralize the other variants).21 In Israel, where more than 50% of people have been vaccinated with the BioNTech/Pfizer vaccine, a study of over 1 million people (596,618 vaccinated and 596,618 non-vaccinated) shows the vaccine to be 92% effective against infection, 94% effective against symptomatic COVID-19, 87% effective against hospitalization and 92% effective against severe disease (data were obtained 7 days or more after the second dose).22 Thus, the BioNTech/Pfizer vaccine is highly effective not only in prevention of disease but also transmission. The occurrence of adverse effects is reported to be lower for the Pfizer/BioNTech vaccine compared with the Moderna vaccine.23 Although very rare moderate-to-severe thrombocytopenia and thrombotic complications have been associated with vaccination against SARS-CoV-2 with the AstraZeneca recombinant adenovirus vector ChAdOx1 nCov-19,24 such association was not observed with the two approved and broadly used mRNA vaccines. The mediators of this complication are platelet-activating antibodies against platelet factor 4. It is postulated that interactions between the adenovirus and platelets or free DNA in the adenovirus vaccines could pay a role in this pathogenesis. On this basis, it is understandable that this complication is unlikely following injections of mRNA vaccines. The third mRNA vaccine, developed by CureVac, showed promising results in phase I and is now being tested in phase III clinical trials. The results are anticipated in the first half of 2021. If this vaccine is approved by regulatory agencies, it will add immediately to the available stocks of hundreds of millions of doses of IVT mRNA-based vaccines. The upscaled production capacities of the three major mRNA vaccine companies, namely, BioNTech, Moderna and CureVac, should allow the vaccination of a large part of the world population safely and efficiently before the end of 2021.
Influenza vaccines in immunosuppressed adults with cancer
Patients with cancer often experience preventable viral infections, including influenza A and B, which can result in substantial morbidity and mortality. Patients with hematological or solid cancers undergoing chemotherapy and/or bone marrow transplant are at increased risk of influenza‐related complications.25 26 Subjects at highest risk include those with impaired cell‐mediated and antibody‐mediated immunity, as reflected by a decrease in the number or function of T and B lymphocytes.27 28 Influenza immunization has been shown to decrease the risk of influenza infection in patients with intact immunity.29 In patients with cancer, although altered humoral and cellular immunity has been reported,30 active immunization confers protective immunity against several infections, including non-influenza infections, at similar rates to healthy individuals, which results in decreased duration and severity of the infection and potentially improved morbidity and mortality.31 Patients with solid tumors and certain hematological malignancies are able to mount a serological response to influenza vaccine; however, it is unclear to what extent this response protects from influenza infection or its complications.32 Comparisons related to the efficacy of the influenza vaccination in adult patients with cancer during chemotherapy versus that in patients not undergoing active treatment showed protective hemagglutination inhibition (HAI) antibody titers with fourfold rise in antibody titer in pre and post-vaccination immune assay. Serological responses to influenza vaccination in adults receiving chemotherapy were weaker compared with those who had completed chemotherapy.33–35 When immunity in response to influenza vaccination was compared in patients with cancer receiving chemotherapy and healthy adults, serological responses in patients receiving chemotherapy were found to be weaker. However, patients with cancer on active chemotherapy were still able to mount protective HAI titers.30 33 36 37 In patients with lymphoma, some studies found that immunization had no benefit in providing adequate seroconversion; hence, those studies did not recommend influenza vaccination in these patients.38 39
With the increasing use of immune checkpoint inhibitors (ICIs) in routine oncology practice and in light of their different mode of action as compared with cytotoxic chemotherapy, the question about the immunogenicity of the influenza vaccine in these patients can be raised. Keam and colleagues showed that the seroprotection and seroconversion rates were significantly higher for all strains—except for the H1N1 strain—in patients receiving ICIs compared with those receiving cytotoxic chemotherapy.40 Although humoral responses, including seroprotection and seroconversion, have been widely used as markers of influenza vaccine immunogenicity, several studies have underscored the importance of influenza-specific T cells in eliminating influenza infection. In a separate study evaluating cell-mediated immune responses elicited by vaccination, defined as the increase of polyfunctional CD4+ and CD8+ T cells reacting to both H1N1 and H3N2 strains of influenza, patients with cancer receiving ICI had significantly higher frequencies of influenza-reactive polyfunctional T cells.41
Safety is paramount when it comes to vaccination of the healthy population, but also is of particular importance in vulnerable patient groups. Sommer et al showed that the use of inactivated vaccines in patients with cancer is safe, but the ability of a patient with cancer to mount an immune response is affected by timing between vaccine and chemotherapy administration.42 The authors of the study emphasized that vaccines should be administered at a minimum of 2 weeks before or after chemotherapy administration for optimal benefit to the patient. The ideal timing for vaccination remains, however, highly controversial. With regard to safety of influenza vaccination in patients undergoing anti-programmed cell death protein-1 (PD-1) therapy (nivolumab or pembrolizumab), Chong et al showed no increase in incidence or severity of immune-related adverse events (IRAEs) within either approximately 2 months of ICI treatment or in newly treated patients. Indeed, the IRAE rates were comparable to those from published clinical trials and did not vary with order of administration.
SARS-CoV-2 vaccines: specific considerations in patients with cancer
Patients with cancer are at increased risk of developing severe COVID-19 and will therefore likely derive substantial benefit from vaccination against SARS-CoV-2.21 43 44 Seminal phase 3 trials leading to Emergency Use Authorization of vaccines against SARS-CoV-2 have largely excluded patients with cancer.9 15 The increased risk from COVID-19 that is associated with a cancer diagnosis is likely determined by a host of variables including the type of cancer, the stage, the specifics of the cancer-directed therapy, and non-cancer-related comorbidities, among others. Given the lack of a more nuanced understanding as to which of the cancer-related variables impact outcomes from COVID-19, patients with cancer have been advised to receive SARS-CoV-2 vaccines independent of details of their cancer diagnosis or treatment. There is also a concern that the immunosuppressive states in patients with cancer may be conducive to evolution of SARS-CoV-2 in a given host, thereby promoting the emergence of variants, providing further support to prioritize patients with cancer for SARS-CoV-2 vaccination.45 Studies investigating the efficacy, immunogenicity, and safety of SARS-CoV-2 vaccination in patients with cancer both prospectively and retrospectively have been initiated at a number of institutions around the world. Many of these studies include systemic efforts to assess vaccine-specific humoral and cellular immune responses including their strength and duration. Results from these studies are expected to provide insights into how SARS-CoV-2-specific immune responses induced by vaccination are impacted by anticancer therapies including radiotherapy and systemic treatments such as chemotherapy, targeted therapy, immunotherapy, or hormonal therapy. The immune modulatory effects of cancer-directed therapies that are not primarily designed to target the immune system have recently come into focus as these ‘non-immune’ anticancer interventions are being tested extensively in combination with ICIs and other immunotherapies. In the context of cancer vaccines, there is evidence that frequencies of immunosuppressive myeloid cells are elevated in patients with cancer and that chemotherapy can have a favorable impact on the strength of vaccine-induced immune responses as well as clinical benefit by reducing CD14+HLA-DR+myeloid-derived suppressor cells (MDSCs).46 The sequencing of chemotherapy in relation to vaccination had an impact on the extent of MDSC numbers reversal. In the context of ICI, recent preclinical studies have demonstrated that PD-1 pathway blockade can compromise the formation of vaccine and/or vaccine-specific memory T cells, raising the potential concern that ICI may compromise the generation of durable SARS-CoV-2-specific T cell responses.47–49 From a clinical evaluation, BNT162b2 mRNA COVID-19 vaccine appears to have a good short-term safety profile in patients with cancer treated with ICIs.50 While these systematic studies will provide important new insights relevant to cancer immunology and related fields, at this point they do not have any practical relevance; there are a number of practical aspects that will (and should) primarily drive decision-making as it relates to SARS-CoV-2 vaccinations for patients with cancer. In other words, while it will be interesting to learn about vaccine-induce immune response in specific ‘cancer scenarios’, since the overarching goal is to vaccinate the entire population as soon as possible, there is also a general consensus that patients with cancer as a group should be prioritized, that is, vaccinated as soon as possible, the establishment of further subcategories or priority groups of patients with cancer also seems impractical. Nevertheless, particularly for patients with cancer who are actively receiving cancer-directed therapy, there are a number of circumstances that warrant more specific considerations regarding timing of SARS-CoV-2 vaccination and therapy as well as testing.
SARS-CoV-2 vaccination in the context of immunosuppression
Immunosuppressive states can arise from the cancer itself, the cancer-directed therapy, or immune suppressive treatments given for various cancer-related conditions. Conceptually, cancer patients with additional immunosuppressive conditions or cancer types associated with specific immunosuppressed states such as certain hematologic malignancies should be prioritized given the increased risk of adverse outcomes from COVID-19 that is associated with immune suppression. However, this reality should also be weighed against the concern that a suppressed immune system may be compromised in building an effective response against SARS-CoV-2 on vaccination and the vaccine should not be delayed due to a mildly immunosuppressed state associated with cancer. Initial studies have revealed low antibody titers after full courses of SARS-CoV-2 mRNA vaccines in large proportions of patients with B cell malignancies.51 This inability to mount a sufficient serologic response appears to be particularly pronounced in patients with chronic lymphocytic leukemia and those who have received anti-CD20 antibody therapy within 1 year of vaccination.51 Nevertheless, the available data are still quite limited; furthermore, the serologic response status may not provide a full assessment of a patient’s immune response to SARS-CoV-2 vaccination and the role of T cell–mediated immunity in protecting from SARS-CoV-2 is relatively poorly defined. In the absence of more definitive data, patients with B cell malignancies should receive SARS-CoV-2 vaccination independent of whether they are on active therapy. One exception is the setting of chimeric antigen receptor T cells cell therapy, where most centers currently recommend to hold vaccination until 3 months after completion of the treatment. We envision that future studies will provide more guidance with regard to the most suitable testing strategies or additional vaccinations, for example, with a different type of vaccine or additional booster.
Corticosteroids and other immunosuppressive agents given in the context of anticancer therapy
Corticosteroids are routinely administered to patients with cancer for various reasons including prospective mitigation of expected chemotherapy toxicities, control of central nervous system edema, antiemesis, or the treatment of immune-related toxicities resulting from ICI. In the context of cancer vaccines, we and others have found that administration of dexamethasone prior to or during the priming phase of vaccination blunted the successful induction of vaccine-specific immune responses, possibly because of systemic depletion of lymphocytes.52 53 Since corticosteroids and other immunosuppressive therapies are often given for defined, relatively brief periods, oncology care providers should consider delaying SARS-CoV-2 vaccination until a corticosteroid treatment course has been completed or the dose has been reduced to ≤10 mg of prednisone equivalent. An anticipated relatively common scenario is a patient with cancer who receives ICI and develops immune-related toxicities requiring treatment temporary treatment with corticosteroids or other immunosuppressive agents such as tumor necrosis factor-α inhibitors, calcineurin inhibitors, or mycophenolate mofetil.
Immunosuppressed state in the context allogeneic-stem cell transplantation
Patients who have received a hematopoietic stem cell transplant (HSCT) require revaccinations against a variety of pathogens due to loss of immunity from previous vaccines against infectious organisms after transplant.54 Because of the profoundly immunosuppressed state immediately after transplantation post HSCT, vaccines are typically not administered until day 100 after transplantation. While vaccines are generally less effective in HSCT recipients compared with healthy individuals, they are nonetheless recommended.55 Based on this practice and rationale, SARS-CoV-2 vaccination should not be administered until the 100 day mark after HSCT; given the lack of any previous vaccine-induced immunity against SARS-CoV-2, the ongoing COVID-19 pandemic, and the relatively high morbidity and mortality of COVID-19, consideration should be given to prioritize SARS-CoV-2 vaccination over the standard revaccinations in patients who received an HSCT.
Emerging observations and challenges as patients with cancer begin to widely receive SARS-CoV-2 vaccines
Cancer imaging
Increased size of axillary, subpectoral, and subclavian lymph nodes after SARS-CoV-2 vaccination detected clinically or on radiographic imaging performed for screening, diagnostic, or monitoring purposes in patients with cancer have been reported.56 Although current reports are largely anecdotal and reactive lymphadenopathy observed in the clinical trials were rare and only observed clinically, the rate and degree of lymphadenopathy noted after SARS-CoV-2 vaccination appears to be higher compared with other vaccines, for example, influenza vaccines. This observation would be consistent with the relatively high rate of local and systemic toxicities such as injection site pain and influenza-like symptoms reported with the mRNA-based SARS-CoV-2 vaccines. The median duration of lymphadenopathy is not known yet and will likely vary widely across patients and with different vaccine platforms. While reactive lymphadenopathy is expected as a vaccine-specific immune response is triggered in the draining lymph nodes, it can complicate the correct interpretation of radiographic images or lead to additional diagnostic workup and anxiety for the patient. In some circumstances, it may be advisable to schedule radiographic imaging studies prior to SARS-CoV-2 vaccination or delay such testing until 6–10 weeks after the vaccination. Alternatively, communication about the timing of SARS-CoV-2 vaccine and imaging among providers will be important.
Radiation recall phenomenon
From our own practice and emerging reports in the literature, there are anecdotal observations of radiation recall phenomenon (RRP) in patients with cancer who received SARS-CoV-2 mRNA vaccines after completion of radiotherapy.57 In these initial observations, RPP manifested as erythema, edema, pruritus, burning sensation, and/or mild skin exfoliation in skin areas corresponding to the radiated sites. Symptom onset ranged from several days to several months after completion of radiation. The condition is a relatively uncommon acute inflammatory skin reaction that occurs in a skin area that is overlapping with a previous radiotherapy treatment field and has been described as being triggered primarily by chemotherapeutic drugs, but also other therapies including antibiotics.58 While the etiology and pathophysiology of RRP are incompletely understood, inflammatory cytokines may play a role.59 Even though the incidence of this phenomenon in the context of SARS-CoV-2 is not yet known, clinicians should be aware and consider educating their patients about it.
Conclusions
Ideally, prospective clinical trials should demonstrate that mRNA-based SARS-CoV-2 vaccines are effective and safe in patients with cancer. While this might prove impractical, future vaccine studies may be designed in a suitable way to include cohorts of vulnerable subjects—including patients with cancer —to provide precious insights for further clinical implementation. Currently, it is speculated that neutralizing antibodies could be a proxy measure of protection from developing COVID-19 . However, this still needs to be verified, and other factors—including cellular immune responses—might also exert a protective role. While awaiting results from prospective studies aimed at providing a more nuanced understanding of SARS-CoV-2 vaccines in patients with cancer, cancer care providers should consider the currently remarkable efficacy and safety of mRNA-based SARS-CoV-2 vaccination in the general population when advising their patients on SARS-CoV-2 vaccination in order to reduce COVID-19-associated morbidity and mortality in this particularly vulnerable patient population.
Ethics statements
References
Footnotes
ER and SP contributed equally.
Contributors ER, SP and PO conceived, discussed, and wrote this manuscript jointly.
Funding This work was funded by the University of Zurich (URPP “Translational Cancer Research"), the Department of Dermatology at the University Hospital of Zurich, the Swiss National Science Found NRP 78 program, grant number 4078PO_198321 and the EU grant NEWmRNA (Horizon 2020 research and innovation programme No. 965135).
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.