Article Text

Abstract
Most patients with advanced melanoma ultimately fail immune checkpoint inhibitor (ICI) therapy because of primary or acquired resistance. There remains a critical unmet need for new therapies that function via alternative immune activation mechanisms to safely trigger an antitumor immune response in patients with ICI-refractory disease. This commentary discusses the recent failures and hope for novel intratumoral therapies under development in the advanced refractory melanoma setting, outlining key mechanistic differences that may be critical to yielding success in this difficult-to-treat population.
- melanoma
- oncolytic viruses
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Immune checkpoint inhibitors (ICIs) targeting anti-protein death (PD)-1/PD-1 ligand (L1) and/or cytotoxic T-lymphocyte-associated protein-4 have revolutionized the treatment paradigm of advanced melanoma and its adjuvant therapy. While combination ICI therapies are associated with higher objective response rate (ORR) and improved progression free survival and overall survival (OS), grade III/IV immune-related adverse events (irAEs) are also significantly increased. However, despite improved clinical outcomes with ICI, the fact remains that most patients with advanced melanoma ultimately fail to benefit from currently approved ICI mono- or combination therapy due to either primary or acquired resistance.1–4 Thus, there remains a critical need for new therapies that function via alternative immune activation mechanisms, to safely trigger an antitumor immune response in patients with ICI refractory melanoma.4–6
Intratumoral (IT) immunotherapies have been proposed to stimulate an antitumor immune response with little systemic exposure (and presumably, toxicity), making them attractive options to pair with ICI. Examples include talimogene laherparepvec (T-VEC) and the toll-like receptor (TLR)-9 agonist tilsotolimod, in combination with an ICI (pembrolizumab and ipilimumab, respectively), which have held promise in patients with advanced or anti-PD-1-refractory melanoma.7–9 However, recently announced disappointing phase III results for these agents combined with an ICI in the front-line (T-VEC with pembrolizumab in the phase 3 MASTERKEY-265 study was recommended to be halted by the Data Monitoring Committee due to futility on efficacy after an interim analysis. No new safety signals were observed.)10 11 and PD-1-refractory settings (tilsotolimod with ipilimumab failed to meet the primary endpoint of ORR, and the study was halted, given that the combination was unlikely to impact OS),12 respectively, mean that the search for more effective and well-tolerated therapies continues and that even in this period of unprecedented successes, the difficulty to move agents successfully from phase II to phase III remains an issue for the field.
The glaring question becomes why these approaches to date have fallen short, at least in the more mature and larger clinical studies that have been reported. As outlined in Smyth et al,6 for immunotherapies to stimulate a successful antitumor response, priming and activation of T cell responses in tumor tissue and an immune-promoting tumor microenvironment (TME) are essential. In the case of TLR-9, the stimulation of a single type of receptor can trigger localized inflammation and localized tumor responses,13 but this may not be sufficient to trigger the co-stimulatory signals necessary for engendering an effective durable systemic response, required to impact metastatic disease. Another approach involving a TLR-9-based agonist under clinical evaluation focuses on CMP-001, a GpG-A TLR-9 agonist, which is packaged within a virus-like particle designed to activate tumor-associated plasmacytoid dendritic cells to stimulate a CD8+ antitumor response. Preliminary results in anti-PD-1-refractory patients in combination with pembrolizumab were encouraging (ORR of 24% (18/75 patients)),14 and this different CpG type A TLR-9 agonist, combined with a different ICI (anti-PD1), may have quite different outcomes. Likewise, T-VEC (a modified herpes virus) is known to trigger a response in injected lesions but did not lead to significant improvements in OS.15 This suggests that T-VEC fails to trigger new antitumor immune responses, which could be related to immune evasion mechanisms employed by herpes virus.16
Other IT immunotherapies that could address these shortcomings are under investigation. PVSRIPO is a novel viral immunotherapy based on genetic modifications to the Sabin type 1 poliovirus (PV) vaccine, currently under investigation in advanced anti-PD-1/L1-refractory melanoma.17 18 While PVSRIPO causes immune-mediated destruction of tumor cells via infection through the PV receptor, CD155 (which is present on most solid tumors19 20 including melanoma),21 the primary mechanism by which PVSRIPO may yield an antitumor response is through non-lethal CD155-mediated infection of antigen-presenting cells of the TME. Based on this unique mechanism of action, PVSRIPO provides the contextualized signals in the TME that trigger novel antitumor immunity, including sustained type-I/III interferon (IFN) secretion. This mechanism of action differs from agonists of the pattern recognition receptors TLR 3, 4 and stimulator of interferon genes (STING), which induce an NF-κb-mediated inflammatory response (eg, production of interleukin 1 (IL-1), IL-6, IL-12 and TNF, associated with the irAE of cytokine release syndrome).10 22 23 As demonstrated in a B16 murine melanoma model, the unique signaling induced by mRIPO (murine equivalent of PVSRIPO) ultimately leads to highly functional antitumor CD8+ T cells, which, when transferred, yielded a robust antitumor response in untreated tumor-challenged mice.23 The key takeaway from these collective works is that the right kind of innate inflammation must be generated in the right context in the TME to yield a functional, T-cell-mediated, systemic antitumor immune response (see figure 1).
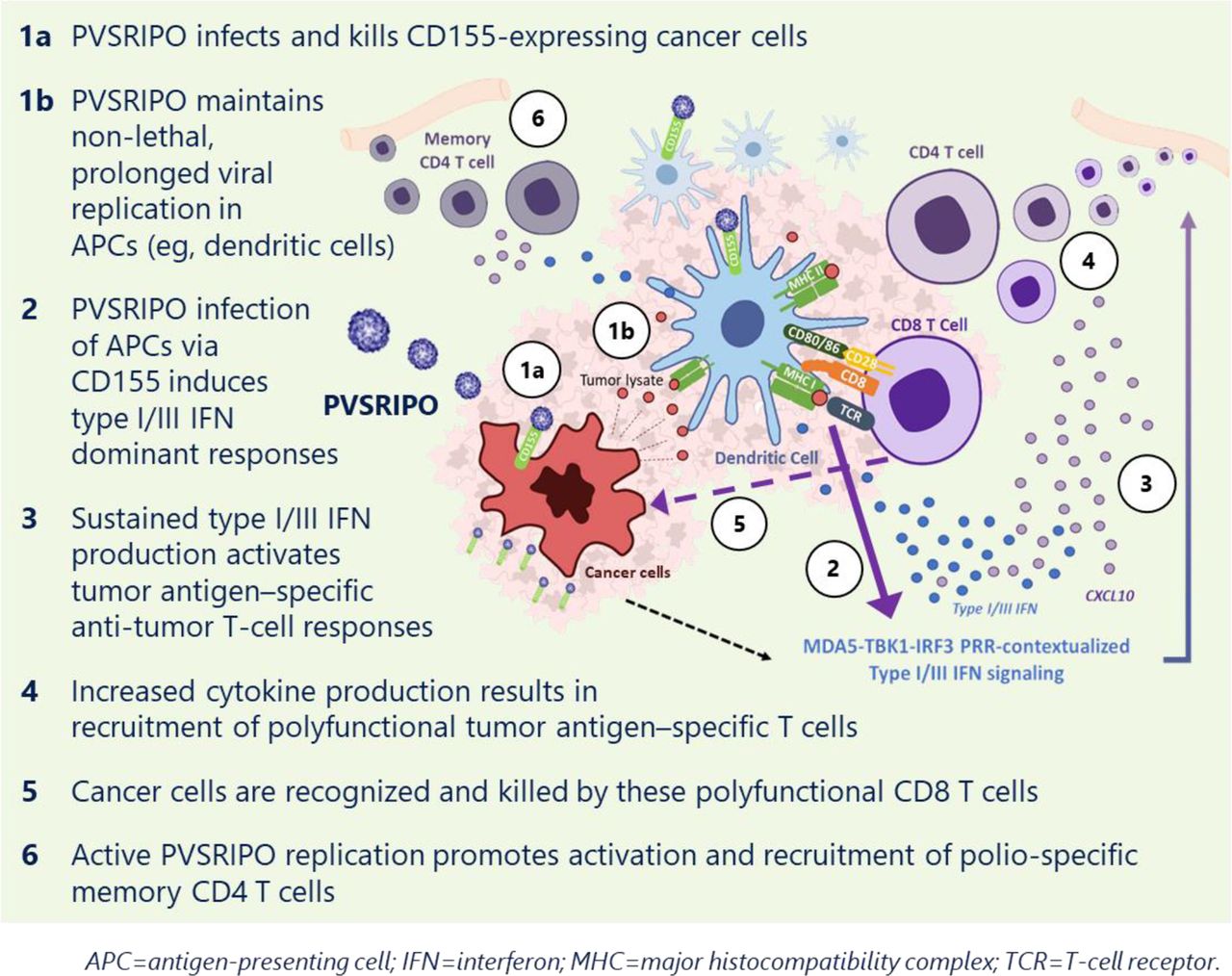
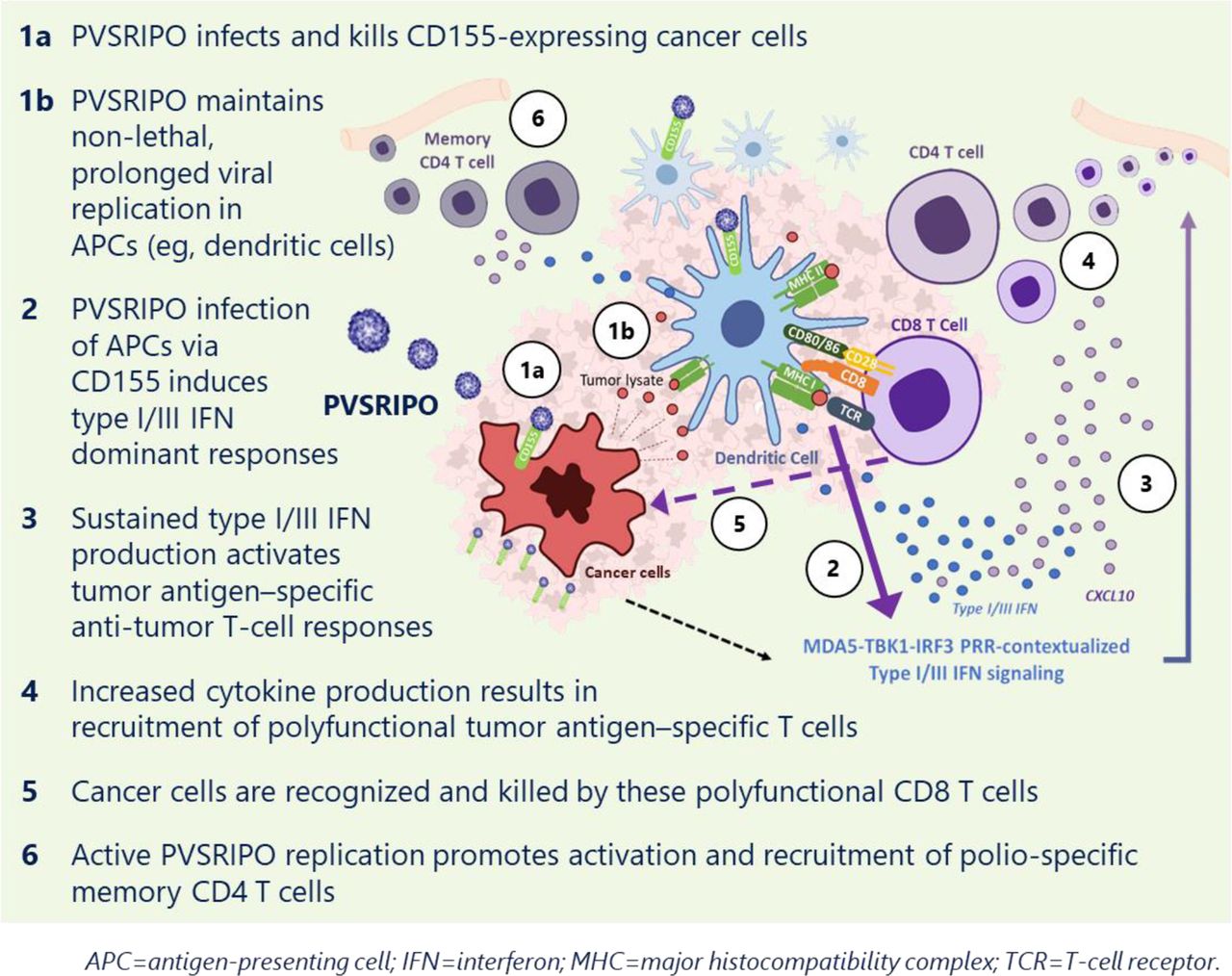{kind=link}
PVSRIPO mechanism of action.
In a recent edition of JITC, Beasley et al24 present the results of a small (n=12), single-center, phase 1 trial of PVSRIPO therapy in patients with unresectable anti-PD-1-refractory melanoma. Key inclusion criteria included the presence of injectable disease. Despite a maximum of three injections with PVSRIPO, an antitumor response in both injected and non-injected lesions was noted in 4/12 (33%) patients. Interestingly, the antitumor response was most notable in patients who had received anti-PD-1 therapy within 30 days prior to PVSRIPO treatment (three of four responders). Of the four responders, pathologic complete response was noted in two patients with in-transit metastases. In addition, 50% (6/12) of patients resuming ICI therapy after PVSRIPO treatment had durable disease control, remaining progression free at a median of 18 months follow-up. This suggests that PVSRIPO treatment may help resensitize an anti-PD-1-refractory tumor to ICI blockade.
Up to three PVSRIPO IT injections at a dose of 1×108 tissue culture infectious dose 50% given in 0.5 mL (given 21 days apart) were well tolerated. No dose-limiting toxicities and no serious or severe AE were noted; the most common AE was mild (grade 1) localized pruritus in approximately 60% of patients. Absence of systemic toxicity and the lack of viral dissemination (as shown by absence of viral shedding in the stool, the primary replication site for PV) are likely the result of pre-existing immunity resulting from prior and boosted anti-PV vaccination, which was required per protocol.
PVSRIPO in combination with anti-PD-1 antibodies, even after anti-PD-1 therapy has failed, has its own rationale: the IFN response induced by PVSRIPO leads to upregulation of PD-L1.22 A phase 2 study, LUMINOS-102 (NCT04577807), is now ongoing to characterize repeat administrations of PVSRIPO with or without PD-1 blockade in patients with advanced melanoma with confirmed anti-PD-1-refractory disease. This study includes patients with cutaneous, acral, or mucosal melanoma, including those with visceral and stable brain metastases. In the phase 1 study, although response was noted in non-injected lesions among patients with in-transit disease, two patients with M1b disease did not show response to the limited course of therapy. Thus, it will be important to determine if optimized dosing with PVSRIPO with or without PD-1 blockade can effectively impact distal metastatic lesions, which is key to improving outcomes in this patient population.
Important design considerations for the LUMINOS-102 study include a requirement of confirmed progression (cPD) with anti-PD-1 therapy per Society for Immunotherapy of Cancer guidelines25 with stratification based on lactate dehydrogenase and time since prior anti-PD-1 therapy. Patients will be randomized to PVSRIPO monotherapy every 3 weeks (injection into up to six lesions per treatment) or PVSRIPO in combination with an approved PD-1 inhibitor per approved labeling. Patients in the monotherapy arm may cross over and receive the combination of anti-PD-1 therapy any time time at cPD, at week 26 if there is no response (eg, stable disease or unconfirmed PD), or when there is partial response lasting ≥26 weeks. There is also a robust translational plan to investigate blood and tissue for markers and correlates of immune response.
Patients with unresectable advanced melanoma refractory to ICI therapy need safe and effective treatment options. The ongoing clinical trials with novel IT immunotherapies under investigation (eg, PVSRIPO, coxsackievirus A2, STING agonists, ONCR-177 (oncolytic herpes simplex virus), viruses with payload (LOAd703, RP-1), CMP-001 (CpG-A TLR9 agonist packaged within a virus-like particle)) and new oncolytic viral constructs that may yield IL-12 in the TME, with or without ICI, will need to deliver systemic antitumor immune responses to ultimately impact advanced metastatic disease and OS. Ultimately, whether novel IT therapies can deliver clinically meaningful benefit for patients with advanced refractory melanoma remains to be seen.
Ethics statements
Patient consent for publication
Acknowledgments
The author thanks Dr Andrea Kelly (Istari Oncology) for editorial assistance. Additional editorial assistance was provided by PharmaWrite, LLC (Princeton, NJ, USA), and was funded by Istari Oncology, Inc. (Morrisville, NC, USA).
References
Footnotes
Correction notice Since this article was first published, a sentence in the second paragraph has been amended for clarity. Please see the full published correction notice for details.
Contributors I have written this editorial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests My disclosures are as follows: Advisory Board, Array BiopharmaResearch funding from Merck, BMS, Pfizer.
Provenance and peer review Not commissioned; externally peer reviewed.