Article Text

Abstract
Background Although immune checkpoint inhibitors (ICIs), especially programmed cell death protein 1 (PD-1)/programmed death ligand 1 (PD-L1) axis blockers, exhibit prominent antitumor effects against numerous malignancies, their benefit for patients with prostate cancer (PCa) has been somewhat marginal. This study aimed to assess the feasibility of B7-H3 or HHLA2 as alternative immunotherapeutic targets in PCa.
Methods Immunohistochemistry was performed to evaluate the expression pattern of PD-L1, B7-H3 and HHLA2 and the infiltration of CD8+ and Foxp3+ lymphocytes in 239 PCa tissues from two independent cohorts. The correlations between B7-H3 and HHLA2 and clinicopathological features, including the presence of CD8+ and Foxp3+ tumor-infiltrating lymphocytes (TILs), were explored.
Results HHLA2 expression was much higher than PD-L1 expression but lower than B7-H3 expression in PCa tissues. High expression of both B7-H3 and HHLA2 was significantly associated with higher Gleason score and tumor stage, lymph node metastasis and dismal overall survival (OS) and cancer-specific survival (CSS). Moreover, a high B7 score, defined as high B7-H3 expression and/or high HHLA2 expression, was an independent prognostic predictor for PCa. Of note, a high B7 score was negatively correlated with CD8+ TILs. Importantly, a new immune classification, based on the B7 score and CD8+ TILs, successfully stratified OS and CSS in PCa.
Conclusions Both B7-H3 and HHLA2 have a critical impact on the immunosuppressive microenvironment, and the B7 score could be used as an independent prognostic factor for PCa. The B7 score combined with CD8+ TILs could be used as a new immune classification to stratify the risk of death, especially cancer-related death, for patients with PCa. These findings may provide insights that could improve response to immune-related comprehensive therapy for PCa in the future.
- costimulatory and inhibitory T-cell receptors
- prostatic neoplasms
- tumor biomarkers
- tumor microenvironment
Data availability statement
Data are available on reasonable request. None.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- costimulatory and inhibitory T-cell receptors
- prostatic neoplasms
- tumor biomarkers
- tumor microenvironment
Introduction
Based on cancer statistics, prostate cancer (PCa) is a leading cause of morbidity and mortality worldwide.1 For localised PCa, radical prostatectomy with/without radiation is the main therapeutic strategy.2 However, androgen deprivation therapy (ADT) continues to be the mainstay of therapy for patients presenting with advanced PCa or failing primary treatment, and most of them can be managed to varying degrees.3 4 Unfortunately, the majority of PCa cases ultimately succumb to tumor development despite the castration levels of testosterone after several years of response, referred to as castration-resistant PCa (CRPC). Treatment options for CRPC have been limited for decades. Even the next-generation antiandrogen enzalutamide provides only a palliative form of care to most patients with CRPC.5 In light of this, there is a crying need to explore new therapeutic schedules for potentiating or superseding existing treatments.
With the extensive investigation of the immune microenvironment within tumors, it is evident that tumor cells can evade immune surveillance via inhibitory checkpoint proteins (ICPs) that promote T cell exhaustion. Programmed death ligand 1 (PD-L1), a member of the B7 superfamily, is one of the most well-known ICPs. Elevated expression of PD-L1 on tumor cells is observed in numerous cancer types, and immune checkpoint inhibitors (ICIs) that block the PD-1/PD-L1 axis confer prominent and durable clinical responses across cancer types, such as melanoma, lung cancer and renal cancer.6–8 The clinical benefit of PD-1/PD-L1 blockers has been reported to be correlated with high PD-L1 expression.9 10 However, unlike the aforementioned cancer types, PD-L1 expression in PCa is rare and there are not sufficient data to warrant treatment of PCa patients with PD-1/PD-L1 axis inhibitors.11–13 Therefore, exploring other immune checkpoints as potential immunotherapeutic targets for most patients with PCa is worthwhile.
B7-H3 (CD276), another B7 superfamily member, is aberrantly expressed in the majority of human malignancies. However, the prognostic significance of B7-H3 is somewhat inconsistent among different tumors.14–17 Moreover, the function of B7-H3 in the immune response is debatable, as both coinhibitory and costimulatory roles within tumors have been demonstrated.18–21 These apparent discrepancies may potentially be associated with the composition of tumor-infiltrating immune cells (TIICs) within different tumors. In terms of PCa, previous studies suggested that B7-H3 is overexpressed by PCa cells and that high expression of B7-H3 is significantly associated with more aggressive phenotypes and a worse prognosis.22 However, the correlation between TIICs and B7-H3 has yet to be studied, which perhaps determines the availability of B7-H3 blockers for PCa treatment.
HERV-H LTR-associating 2 (HHLA2, B7-H7/B7-H5) is a newly identified B7 family member. Similar to B7-H3, the precise physiological function of HHLA2 has not yet been fully elucidated, as both stimulatory and inhibitory properties of HHLA2 have been reported.23 24 Overexpression of HHLA2 has been demonstrated in several cancer types and was found to be correlated with a dismal prognosis in cholangiocarcinoma, lung cancer and renal cancer but associated with a favorable prognosis in pancreatic cancer.25–28 In addition, in our previous study, positive HHLA2 staining was observed in three out of nine PCa tissues.29 However, the clinical relevance of HHLA2 in PCa needs to be further explored.
The aim of this retrospective study was to evaluate the expression pattern and clinical significance of B7-H3 and HHLA2 and their correlations with tumor-infiltrating lymphocytes (TILs) in with PCa. In addition, we attempted to establish a novel immune classification based on B7-H3 and HHLA2 expression, and the density of tumor-infiltrating T cells.
Methods
Patients and samples
We conducted a retrospective study of patients with PCa treated with radical prostatectomy at Sun Yat-sen University Cancer Center (126 cases, named training cohort) from January 2005 to December 2014, or at Sun Yat-sen Memorial Hospital (113 cases, named validation cohort) from January 2009 to December 2013. Oral consent was obtained from each patient in both cohorts. Formalin-fixed, paraffin-embedded tissue blocks were available from all cases and H&E-stained tumor slides were used to confirm the Gleason score, tumor stage and lymph node status by two senior pathologists according to the American Joint Committee on Cancer 2009 tumour, node, metastases classification for PCa. Imaging examination was used to determine distal metastasis. Overall survival (OS) was calculated from prostatectomy to death or the last follow-up, which was December 31, 2019. Cancer-specific survival (CSS) was defined as the time from prostatectomy to death from PCa or the last follow-up.
Immunohistochemistry
In line with our previous study,30 briefly, formalin-fixed PCa tissue sections were paraffinized in xylene and hydrated in a diluted alcohol series. Then, antigen retrieval was accomplished with sodium citrate buffer (10 mM, pH 6.0) using a microwave for 10 min. After that, the sections were immersed in H2O2 (0.3%) for 15 min to reduce activity of endogenous peroxidase. Following blocking with goat serum, the sections were incubated with corresponding primary antibodies (anti-PD-L1: Cell Signaling Technology (CST) #13684; anti-B7-H3: CST, #14058; anti-HHLA2: clone 566.129; anti-CD8: CST, #85336; anti-Foxp3: CST, #12653) at 4℃ overnight. Then, after washing for three times using phosphate buffered saline (PBS), the sections were subsequently incubated with secondary antibody for 1 hour. Finally, the sections were visualized using a DAKO EnVision Detection System (Dako) and counterstained with hematoxylin.
Assessment of PD-L1, B7-H3 and HHLA2 expression and the density of infiltrated immune cells
All sections were assessed by two independent pathologists blinded to the clinical profiles of the patients, and discrepancies were resolved after consensus. PD-L1 positivity in this study was defined as PD-L1 staining in ≥1% of tumor cells.31 Both B7-H3 and HHLA2 immunostaining in tumor cells were semi-quantified using the H-score on account of the percentage of positive staining and the staining intensity. In detail, the staining intensity was divided into four levels as follows: absent (0), weak (1), moderate (2) and strong (3) (online supplemental figure S1A,B). The H-score of each case was determined by multiplying the staining intensity by the corresponding percentage of positive cells. The H-score range was 0 to 300. An H-score >0 was defined as positive expression and the cut-off values for differentiating high and low B7-H3 and HHLA2 expression were 120 and 80 determined by X-tile program, respectively.
Supplemental material
The infiltration extent of CD8+ and Foxp3+ TILs was evaluated according to the mean of counts in five independent high-power fields (400×) within mesenchyme, which represented the densest immune cell infiltrates. The mean value was considered the cut-off point for marker stratifications in this study.25
Statistical analysis
The distribution of clinicopathological parameters, including the densities of different sets of immune cells over B7-H3 or HHLA2 expression categories, was evaluated using χ2 or Fisher’s exact test. The OS and CSS curves were depicted with the Kaplan-Meier method, and the intergroup differences were examined using a log-rank test. Cox proportional hazard regression analysis was performed for univariate and multivariate analyses. All statistical analyses were performed using SPSS V.24.0 (Chicago, Illinois, USA) or GraphPad Prism V.8 (La Jolla, California, USA) software.
Results
Clinicopathological characteristics of patients with PCa
The basic clinicopathological characteristics of 239 patients with PCa from two independent cohorts are summed up in online supplemental table 1. The mean age at operation was 66 years (range, 42–86) in the training cohort and 69 years (range, 52–89) in the validation cohort, respectively. At the end of follow-up, 36 (28.6%) patients died, including 25 (19.8%) cases died from tumor progression in the training cohort. The median follow-up time was 88.5 months (range, 4–171). The 5-year and 10- year OS rates were 81.4% and 64.7%, respectively, and the 5-year and 10-year CSS rates were 85.0% and 73.2%, respectively. In the validation cohort, 22 (19.5%) patients died, including 15 (13.3%) cases died from tumor progression, and the median follow-up time was 78.0 months (range, 1–126). The 5-year and 10-year OS rates were 84.2% and 78.5%, respectively, and the 5-year and 10-year CSS rates were 87.8% and 85.4%, respectively.
PD-L1, B7-H3 and HHLA2 expression in PCa
To evaluate the expression spectrum of PD-L1, B7-H3 and HHLA2 in PCa tissues from the two cohorts, immunohistochemistry (IHC) was performed, and typical IHC photomicrographs of PD-L1, B7-H3 and HHLA2 expression are presented in figure 1A. PD-L1 was positively stained in 10 (8.2%) cases in the training cohort and 6 (5.3%) cases in the validation cohort (figure 1B). However, B7-H3 was widely expressed in 105 (83.3%) PCa cases in the training cohort and 98 (87.6%) cases in the validation cohort (figure 1C). In terms of HHLA2, positive staining of HHLA2 was detectable in 87 (69.0%) and 77 (68.1%) PCa cases in the two cohorts, respectively (figure 1D). These data demonstrate that B7-H3 and HHLA2 are more frequently expressed in PCa tissues, compared with PD-L1 expression.
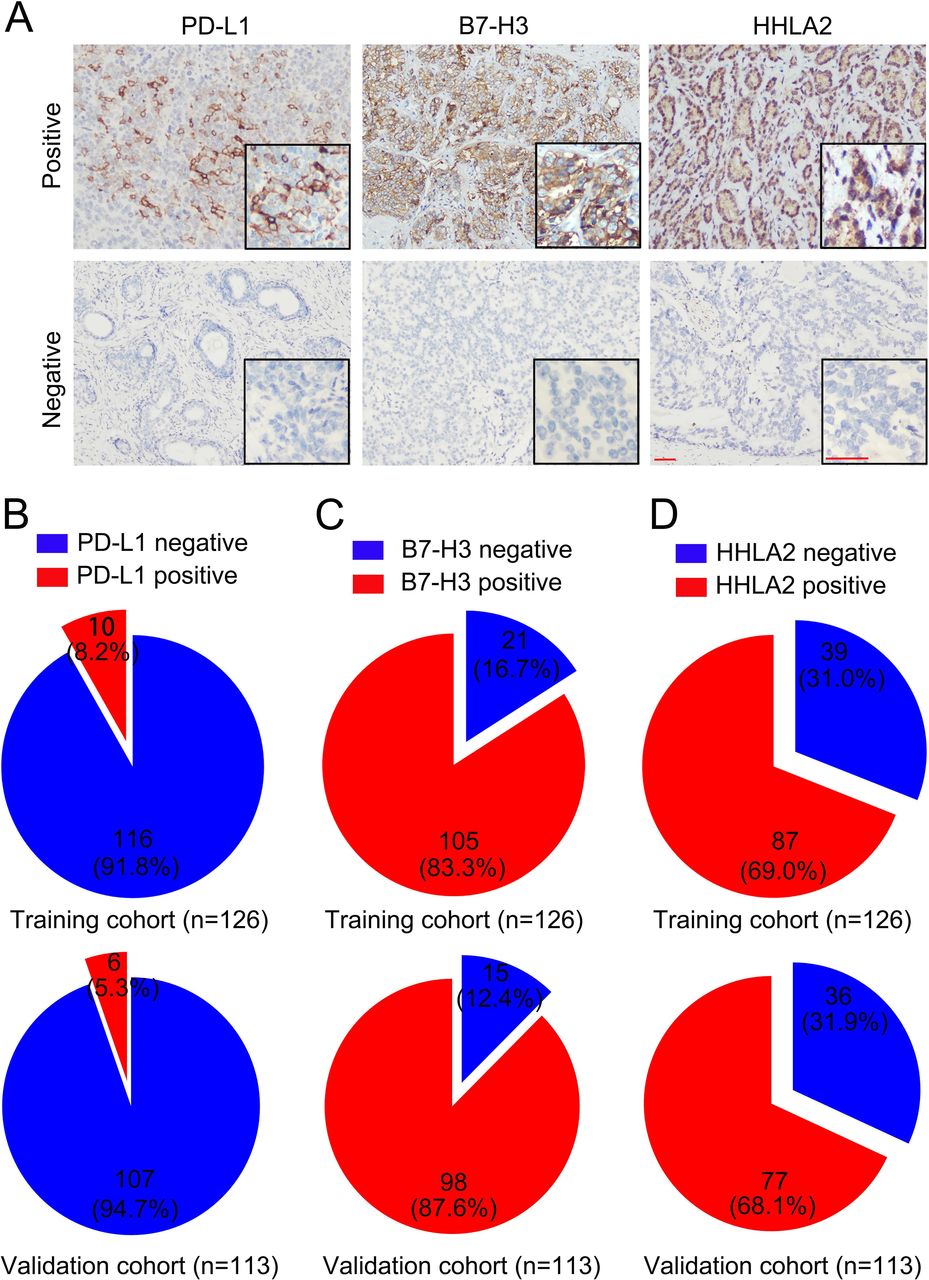
Programmed death ligand 1 (PD-L1), B7-H3 and HHLA2 expression in prostate cancer (PCa) tissue sample. (A) Representative immunohistochemical staining of PD-L1, B7-H3 and HHLA2 within tumor, scale bar, 50 µm. (B) The positive rate of PD-L1 in PCa tissues were 8.2% and 5.3% in indicated cohorts, respectively. (C) The positive rate of B7-H3 in PCa tissues were 83.3% and 87.6% in indicated cohorts, respectively. (D) The positive rate of HHLA2 in PCa tissues were 69.0% and 68.1% in indicated cohorts, respectively.
Association between B7-H3 and HHLA2 and clinicopathological factors in patients with PCa
To evaluate the clinical relevance of B7-H3 and HHLA2, the patients with PCa were segregated into two groups according to the optimal cut-off value for the H-score of B7-H3 (H-score=120) or HHLA2 (H-score=80). As detailed in table 1, high B7-H3 expression (H-score ≥120) was significantly associated with advanced Gleason score (p=0.032 and p=0.006, respectively) and tumor stage (p=0.006 and p=0.001, respectively) in both cohorts. Furthermore, high expression of B7-H3 was also significantly correlated with lymph node metastasis in the training cohort (p=0.001, table 1). Similarly, in both cohorts, increased HHLA2 expression (H-score ≥80) displayed a significant correlation with advanced Gleason score (p=0.001 and p=0.028, respectively), tumor stage (p=0.049 and p=0.031, respectively) and lymph node metastasis (p=0.002 and p=0.046, respectively) (table 1). Of note, significant associations were detected between B7-H3 and HHLA2 expression in both cohorts (p=0.002 and p=0.020, respectively, table 1). Taken together, these data show that high expression of both B7-H3 and HHLA2 might be associated with worse clinicopathological features.
The correlation of B7-H3 and HHLA2 expression with clinicopathological features in both cohorts
Correlation between B7-H3, HHLA2 and TILs in PCa
Microphotographs of CD8+ and Foxp3+ TILs are shown in figure 2A. The density of CD8+ TILs was much higher than the density of Foxp3+ TILs in both cohorts (p<0.001 in both cohorts, figure 2B). In both cohorts, significantly higher densities of CD8+ TILs were detected in tumors with low B7-H3 or HHLA2 expression than in tumors with high B7-H3 or HHLA2 expression (training cohort: B7-H3, p<0.001, HHLA2, p<0.001; validation cohort: B7-H3, p<0.01, HHLA2, p<0.001; figure 2C–D). Conversely, no significant differences in Foxp3+ TILs were observed between tumors with high B7-H3 expression and tumors with low B7-H3 in either cohort (figure 2E–F). Similarly, no significant correlation was observed between HHLA2 expression and Foxp3+ TILs in the training cohort (figure 2E). However, a high density of Foxp3+ TILs was significantly associated with high HHLA2 expression in the validation cohort (p<0.01, figure 2F). These results indicate that both B7-H3 and HHLA2 might account for the immunosuppressive environment within PCa tissues.

The association of B7-H3 or HHLA2 expression with tumor-infiltrating lymphocytes (TILs). (A) Representative micrographs of CD8 and Foxp3 expression within the tumor, scale bar, 50 µm. (B) Scatter plot depicted the density of CD8+ or Foxp3+ TILs in indicated cohorts. (C–D) The counts of CD8+ TILs in tumors with different B7-H3 or HHLA2 expression in indicated cohorts. (E–F) The counts of Foxp3+ TILs in tumors with different B7-H3 or HHLA2 expression in indicated cohorts. Error bars indicate median with SEM, **p<0.01, ***p<0.001, ns, no significance.
The prognostic significance of B7-H3 and HHLA2 in patients with PCa
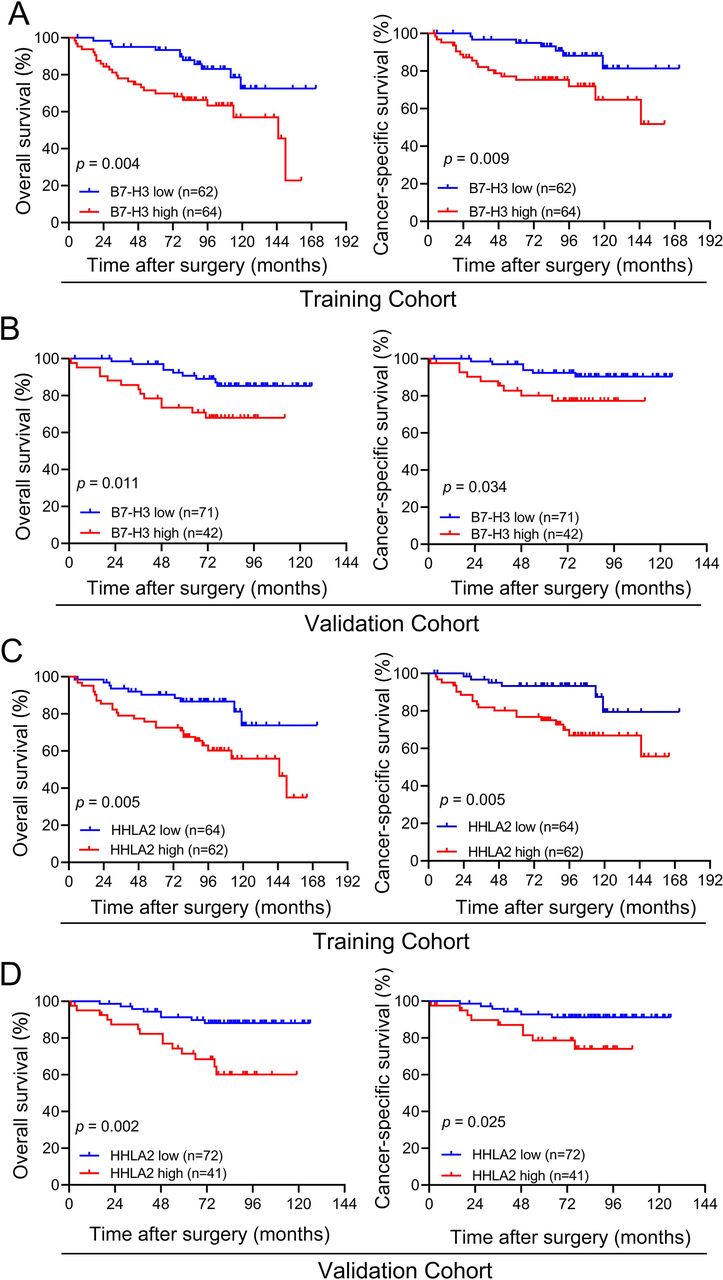
Given the prevalence of B7-H3 and HHLA2 overexpression, a univariate analysis of OS and CSS was generated to evaluate the prognostic significance of B7-H3 and HHLA2 expression. Interestingly, high B7-H3 expression conferred a greater than twofold increase in the risk of mortality, especially CSS, in both cohorts (OS: training cohort, HR=2.70, 95% CI=1.33 to 5.50, p=0.006; validation cohort, HR=2.85, 95% CI=1.21 to 6.68, p=0.016; CSS: training cohort, HR=3.01, 95% CI=1.26 to 7.24, p=0.014; validation cohort, HR=2.90, 95% CI=1.03 to 8.17, p=0.043; table 2). Similarly, Kaplan-Meier analyses demonstrated that patients with high B7-H3 expression had shorter OS and CSS than those with low expression of B7-H3 in both cohorts (for the training cohort, OS: p=0.004, CSS: p=0.009; for the validation cohort, OS: p=0.011, CSS: p=0.034; figure 3A–B).

Association of B7-H3 or HHLA2 expression with overall survival (OS) and cancer-specific survival (CSS) depicted by Kaplan-Meier survival curves. (A–B) OS and CSS according to B7-H3 expression in indicated cohort. (C–D) OS and CSS according to HHLA2 expression in indicated cohort.
Univariate analysis of prognostic factors correlated with OS and CSS
In line with the results for B7-H3, patients with high HHLA2 expression demonstrated significantly lower OS, especially CSS, than patients with low HHLA2 expression in both cohorts (OS: training cohort, HR=2.73, 95% CI=1.31 to 5.69, p=0.007; validation cohort, HR=3.70, 95% CI=1.55 to 8.83, p=0.003; CSS: training cohort, HR=3.44, 95% CI=1.37 to 8.65, p=0.008; validation cohort, HR=3.06, 95% CI=1.09 to 8.62, p=0.034; table 2). Furthermore, high HHLA2 expression was demonstrated to contribute to shorter survival of patients with PCa in both cohorts (for the training cohort, OS: p=0.005, CSS: p=0.005; for the validation cohort, OS: p=0.002, CSS: p=0.025; figure 3C–D).
Multivariate analysis revealed that neither B7-H3 nor HHLA2 were independent risk factors for OS and CSS in the training cohort (table 3). However, HHLA2 was identified as an independent risk factor for OS in the validation cohort (HR=3.15, 95% CI=1.10 to 9.00, p=0.032, table 3).
Multivariate analysis of prognostic factors correlated with OS and CSS with regard to B7-H3 and HHLA2
Association of B7 score with prognosis and tumor-infiltrating immune cells
A previous study demonstrated that extensive infiltration of CD8+ TILs can independently predict a favorable prognosis in PCa.32 Considering the close correlation between B7-H3 and HHLA2 and the infiltration of CD8+ TILs, it is confusing that neither B7-H3 nor HHLA2 were independent prognostic factors. To further determine the relationship between B7-H3 and/or HHLA2 expression and the prognosis of patients with PCa, we attempted to generate a potential tool for predicting survival, based on the expression of B7-H3 and HHLA2. The patients with PCa were presorted into four groups according to the expression of B7-H3 and HHLA2 as follows: group I (B7-H3low/HHLA2low), group II (B7-H3low/HHLA2high), group III (B7-H3high/HHLA2low) and group IV (B7-H3high/HHLA2high). In both cohorts, Kaplan-Meier analysis demonstrated that patients in groups II–IV experienced shorter OS and CSS than patients in group I (online supplemental figure S2A,B). However, no significant difference was detected among patients in groups II–IV in both cohorts (online supplemental figure S2A,B). Thus, we then divided the patients into two groups: low B7 score, B7-H3low/HHLA2low; high B7 score, B7-H3low/HHLA2high, B7-H3high/HHLA2low or B7-H3high/HHLA2high. As shown in online supplemental table S2, a high B7 score was significantly associated with advanced Gleason score (p=0.040 and p=0.001, respectively) and tumor stage (p=0.022 and p=0.002, respectively) in the two cohorts. Moreover, a high B7 score was significantly correlated with lymph node metastasis in the training cohort (p=0.010, online supplemental table S2). Kaplan-Meier analysis also demonstrated that high B7 score significantly stratified OS and CSS in both cohorts (for the training cohort, OS: p=0.001, CSS: p=0.004; for the validation cohort, OS: p<0.001, CSS: p=0.002; figure 4A,B). More importantly, in a multivariate analysis, patients with high B7 score were still over four times more likely to die, especially from tumor-related factors, after adjusting for possible confounding variables in the training cohort (OS: HR=4.33, 95% CI=1.29 to 14.56, p=0.018; CSS: HR=4.54, 95% CI=1.03 to 20.02, p=0.046; table 4). In the validation cohort, the B7 score was an independent predictor for OS and tended to be an independent predictor for CSS (OS: HR=10.76, 95% CI=1.41 to 82.50, p=0.022; CSS: HR=6.52, 95% CI=0.82 to 52.09, p=0.077; table 4). Of note, a high B7 score was inversely associated with a high density of CD8+ TILs (p<0.001 in both cohorts, figure 4C). However, no correlation was detected between Foxp3+ TILs and B7-H3 or HHLA2 expression in either cohort (figure 4C).

The correlation of B7 score with overall survival (OS), cancer-specific survival (CSS) and tumor-infiltrating immune cells (TILs). (A–B) OS and CSS according to B7 score in indicated cohort. (C) The counts of CD8+ and Foxp3+ TILs in tumors with different B7 score in indicated cohorts. Error bars indicate median with SEM, **p<0.01, ***p<0.001, ns, no significance.
Multivariate analyses of prognostic factors correlated with OS and CSS with regard to B7 score
To sum up, these data indicate that the combination of B7-H3 and HHLA2 expression might have better prognostic value in patients with PCa.
Development of a novel immune classification based on the B7 score and CD8+ TILs
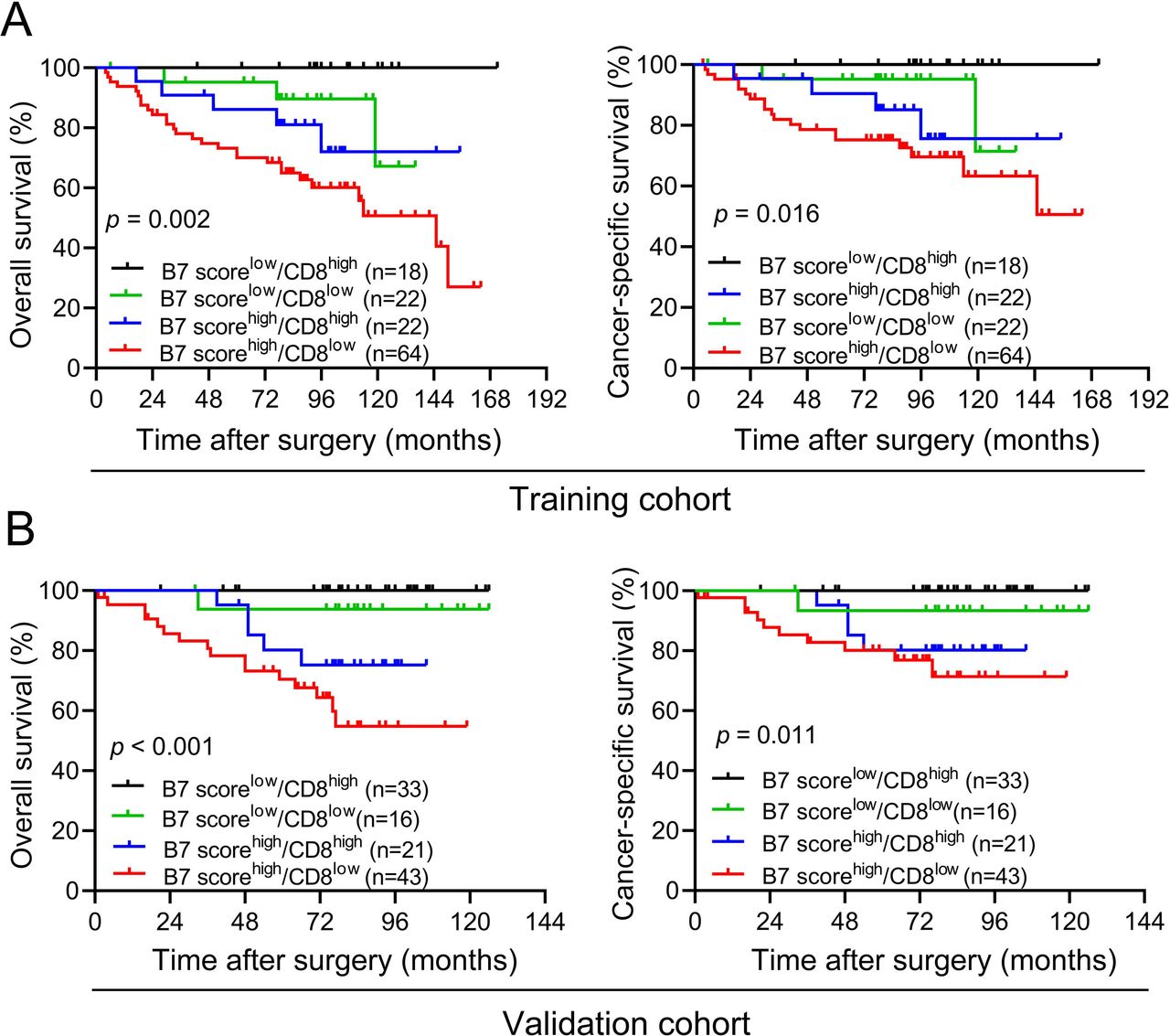
Based on the above findings, we developed a novel immune classification scheme according to the B7 score and the density of CD8+ TILs. Specifically, the patients with PCa were classified into four immune types: immune type I (low B7 score, high CD8+ TILs), immune type II (low B7 score, low CD8+ TILs), immune type III (high B7 score, high CD8+ TILs) and immune type IV (high B7 score, low CD8+ TILs). The proportions of patients with PCa with immune types I, II, III and IV were 14.3% (18/126), 17.5% (22/126), 22% (22/126) and 50.8% (64/126), respectively in the training cohort. Of 113 patients with PCa from the validation cohort, 29.2% (n=33) belonged to immune type I, 14.2% (n=16) belonged to immune type II, 18.6% (n=21) belonged to immune type III and 38.1% (n=43) belonged to immune type IV. According to the Kaplan-Meier analysis, immune type IV was more significantly correlated with the poorest OS and CSS among patients with the four immune types in both cohorts (figure 5A–B). Conversely, immune type I was significantly correlated with improved OS and CSS in both cohorts, even no death was observed during the follow-up (figure 5A–B). However, no difference in OS and CSS was found between immune type II or III in either cohort (figure 5A–B). These data demonstrate that this novel immune classification might provide direction for predicting prognosis and immunotherapy results.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association of new immune classification with overall survival (OS) and cancer-specific survival (CSS) depicted by Kaplan-Meier survival curves. (A–B) OS and CSS according to new immune classification in indicated cohort.
Discussion
As far as we know, this is the first comprehensive study measuring the expression pattern of three different B7-family member ligands (PD-L1, B7-H3 and HHLA2) in two sizeable cohorts of patients with PCa. We found that positive HHLA2 staining was much more frequent than positive PD-L1 staining, but relatively less prevalent than positive B7-H3 staining. Moreover, our results are the first to demonstrate that high HHLA2 expression is significantly correlated with worse clinicopathological features, including higher Gleason score, tumor stage and lymph node metastasis, and shorter OS and CSS, in keeping with the clinical relevance of B7-H3 in PCa, which has been described in our previous studies and was confirmed in present study.33 34 These data indicate that both B7-H3 and HHLA2 might mediate immune evasion in PCa and are potential targets for immunotherapy.
Although both B7-H3 and HHLA2 have similar immunological functions and our data showed a significant association between B7-H3 and HHLA2, simultaneous overexpression of B7-H3 and HHLA2 was detected in only 31% of the PCa cases in the training cohort and 18% of the PCa cases in the validation cohort. These results suggest that overexpression of B7-H3 or HHLA2 may inhibit the activation and proliferation of T cells via non-redundant/exclusive inhibitory pathways. Given the infrequent co-overexpression of B7-H3 and HHLA2, we were the first to evaluate the prognosis of patients with PCa by combining B7-H3 with HHLA2. We found that a high B7 score, including B7-H3low/HHLA2high, B7-H3high/HHLA2low or B7-H3high/HHLA2high, was significantly associated with detrimental clinicopathological features and a poor prognosis. Furthermore, it was an independent prognostic factor for OS and CSS. These data indicate that B7-H3 combined with HHLA2 displays better value in predicting the prognosis of patients with PCa. These findings might also direct immunotherapy for PCa in the future. Specifically, simultaneous blockade of the B7-H3 and HHLA2 pathways may be an optimal therapeutic schedule for patients with PCa with high B7-H3 and HHLA2 expression. However, for patients with overexpression of one marker, a single inhibitor targeting the corresponding maker may be sufficient.
Accordingly, there is still no consensus on the immunological function of B7-H3 and HHLA2 because both protumor and antitumor roles of these proteins have been postulated. For example, a previous study indicated that B7-H3 was involved in suppression of interferon-γ secretion. Consistently, antagonizing B7-H3 increased CD8+ T cell aggregation and antitumor response in mouse models.35 36 However, paradoxically, in another early study, B7-H3 was suggested to be a costimulator of T cells, facilitating cytokine production.18 Likewise, HHLA2 has been proved to promote T cell growth and cytokine secretion via an AKT-dependent signaling cascade.24 In contrast, HHLA2 was also reported to inhibit the proliferation both CD4+ and CD8+ T cells and reduce cytokine production by T cells.23 The paradoxical dual function of both B7-H3 and HHLA2 among heterogeneous malignancies may be resulted from differential expression of corresponding activating or inhibitory ligands on immune cells or differential infiltration of sets of immune cells. In this study, we comprehensively evaluated the association between HHLA2 and B7-H3 and the TILs. Overexpression of both B7-H3 and HHLA2 was significantly associated with fewer CD8+ TILs. High expression of HHLA2 was also accompanied by prominent Foxp3+ TILs in the validation cohort. These data demonstrate that both B7-H3 and HHLA2 are associated with a suppressive immune microenvironment within PCa. Meanwhile, enoblituzumab, an anti-B7-H3 monoclonal antibody, exhibited antitumor activity in preclinical tumor models of PCa.37 Thus, it is convincing that both B7-H3 and HHLA2 mainly perform immunosuppressive functions within PCa tissues.
Recently, with the advent of precision medicine, numerous immune classifications have been proposed for guiding immunotherapy. Among them, the proposed theory from Teng et al has been widely recognized across cancer types.38 According to this theory, tumors are classified into four categories as follows: tumors with adaptive immune resistance, tolerance, immunological ignorance and intrinsic induction, based on PD-L1 expression and TIL infiltration. However, this immunophenotype is not suitable for some ‘cold’ cancers, most notably PCa because of the low to no PD-L1 expression. To optimize this immunophenotype, we replaced PD-L1 expression with a new B7 score and examined the potential prognostic impact of the combined B7 score and CD8+ TIL status in patients with PCa. Our data indicate a significant association between stratification based on the B7 score and CD8+ TILs and OS and CSS. For example, patients with a high B7 score and less CD8+ TIL infiltration may be considered as a ‘super-cold’ tumor, which is insensitive to existing clinical immunotherapy and associated with the poorest prognosis. However, it is possible that patients with low B7 scores and high CD8+ TIL infiltration do not require subsequent adjuvant ADT and/or chemoradiotherapy, because of their favorable prognosis. Taken together, these results may have important implications for the design of immunotherapy studies in the future.
The present study has several limitations. First, as a retrospective study, selection bias is inevitable. However, dual-center cohorts would make our data more convincing. Second, the expression level of the immune makers evaluated in the present study were dichotomized as high or low according to the corresponding cut-off values, which were only based on the H-score in both cohorts. Thus, to increase reliability, a larger sample size cohort is needed to identify the exact cut-off. Last, despite the significant correlations among immune markers, the exact colocalization among immune markers is still unclear. Thus, multiple immunofluorescence assays are needed to confirm the associations among different immune markers.
In summary, we demonstrated that both B7-H3 and HHLA2 were associated with immunosuppressive microenvironment, and the B7 score could be used as an independent prognostic factor for PCa. Most importantly, we established a new immune classification on the basis of B7 score and CD8+ TILs, which might significantly stratify OS and CSS in patients with PCa.
Data availability statement
Data are available on reasonable request. None.
Ethics statements
Ethics approval
This study was approved by the Clinical Research Ethic Committee of Sun Yat-sen Memorial Hospital (SYSEC-KY-KS-2020-201) and Sun Yat-sen University Cancer Center (2021-FXY-139).
Acknowledgments
This work was supported by grants from Guangdong Science and Technology Department (2017B030314026). We would like to thank Dr Jian-chang Fu and Dr Yuan-zhong Yang from Department of Pathology, SYSUCC for their assistance in IHC score.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
QZ, KL, YL and KY contributed equally.
Contributors Conception and design: HH, JH and KX. Performed the experiments: QZ and KL. Acquisition and interpretation of data: all authors. Drafting the article: QZ and YL. Manuscript reviewing, editing and approval of the manuscript: all authors.
Funding This study was supported by the National Natural Science Foundation of China (81672550, 81974395, 81702527, 81802527); Guangdong Basic and Applied Basic Research Foundation (2019A1515011437); Guangzhou Science and Technology Cooperation Program (Foreign Research and Development Cooperation) (201807010087); Sun Yat-sen University Clinical Research 5010 Program (2019005); Guangdong Provincial Clinical Research Center for Urological Disease (2020B1111170006); Sun Yat-sen Clinical Research Cultivating Program (201702) to HH, KL or YL.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.