Article Text

Abstract
Background Tislelizumab, an anti-programmed cell death protein-1 monoclonal antibody, demonstrated clinical activity and was well tolerated in patients with previously treated advanced HCC in the open-label, multicenter, Phase 2 RATIONALE-208 study (NCT03419897). We report exploratory analysis of the association of gene expression profiles (GEPs) with response to tislelizumab in patients with previously treated advanced HCC.
Methods Eligible patients who had received ≥1 prior line of systemic therapy for advanced HCC received tislelizumab (200 mg) intravenously once every 3 weeks and tumor response was evaluated per RECIST v.1.1. Baseline tumor sampling was optional and GEP analysis was performed using HTG EdgeSeq Precision Immuno-Oncology panel in 138 tumor samples (fresh tumor, n=6; archival tumor, n=132). Signature scores were calculated using Gene Set Variation Analysis package with publicly available gene signatures (GS). GS or genes differentially expressed between responders and non-responders (NRs) were determined using Wilcoxon rank-sum test and modified t-test with limma. Distributions of overall survival (OS) and progression-free survival (PFS) for GS subgroups (high vs low) were estimated by Kaplan-Meier method. Hierarchical clustering of NRs was achieved using 1-Pearson’s correlation and average linkage. All statistical analysis results are post-hoc exploratory and thereby p values are descriptive.
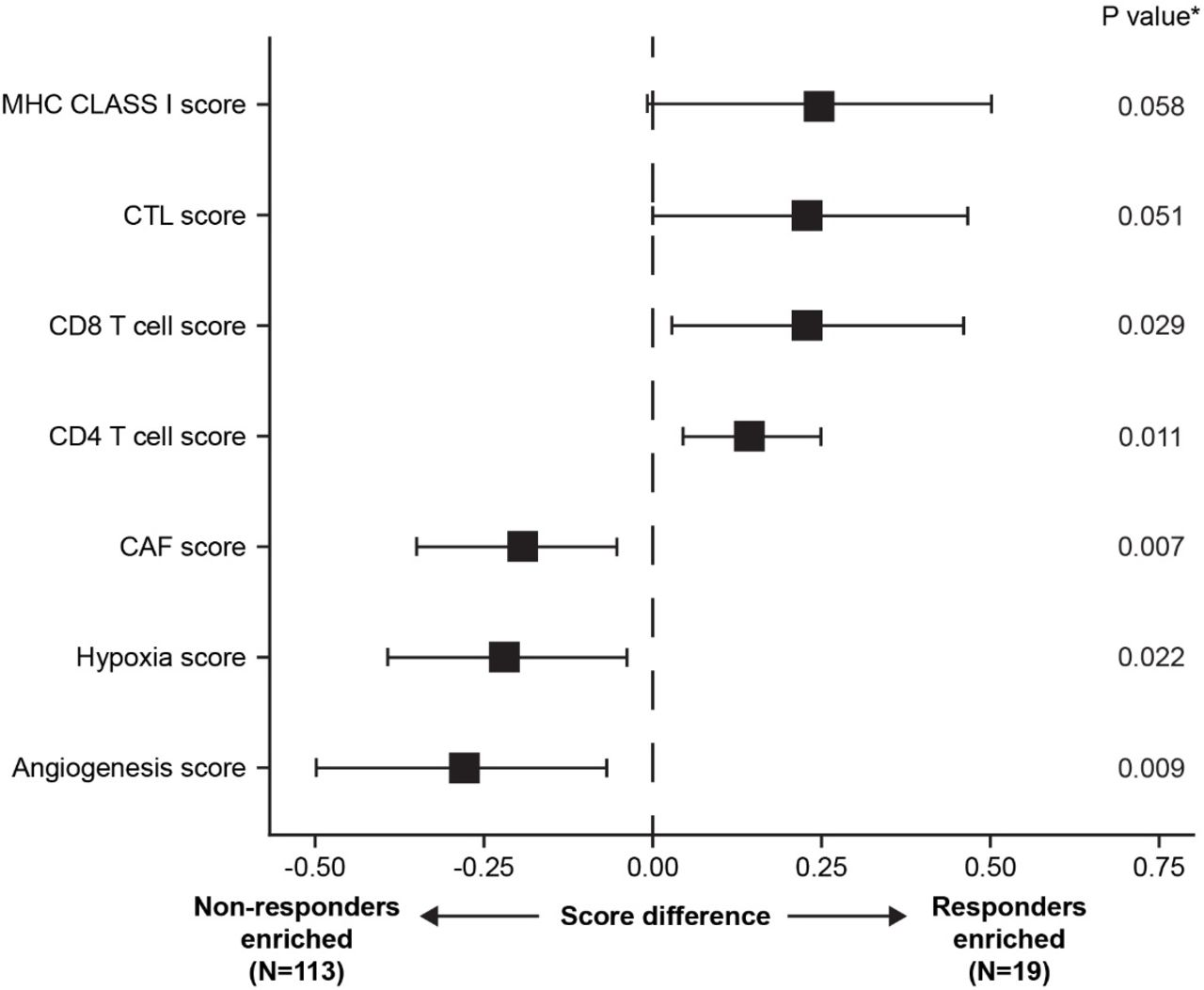
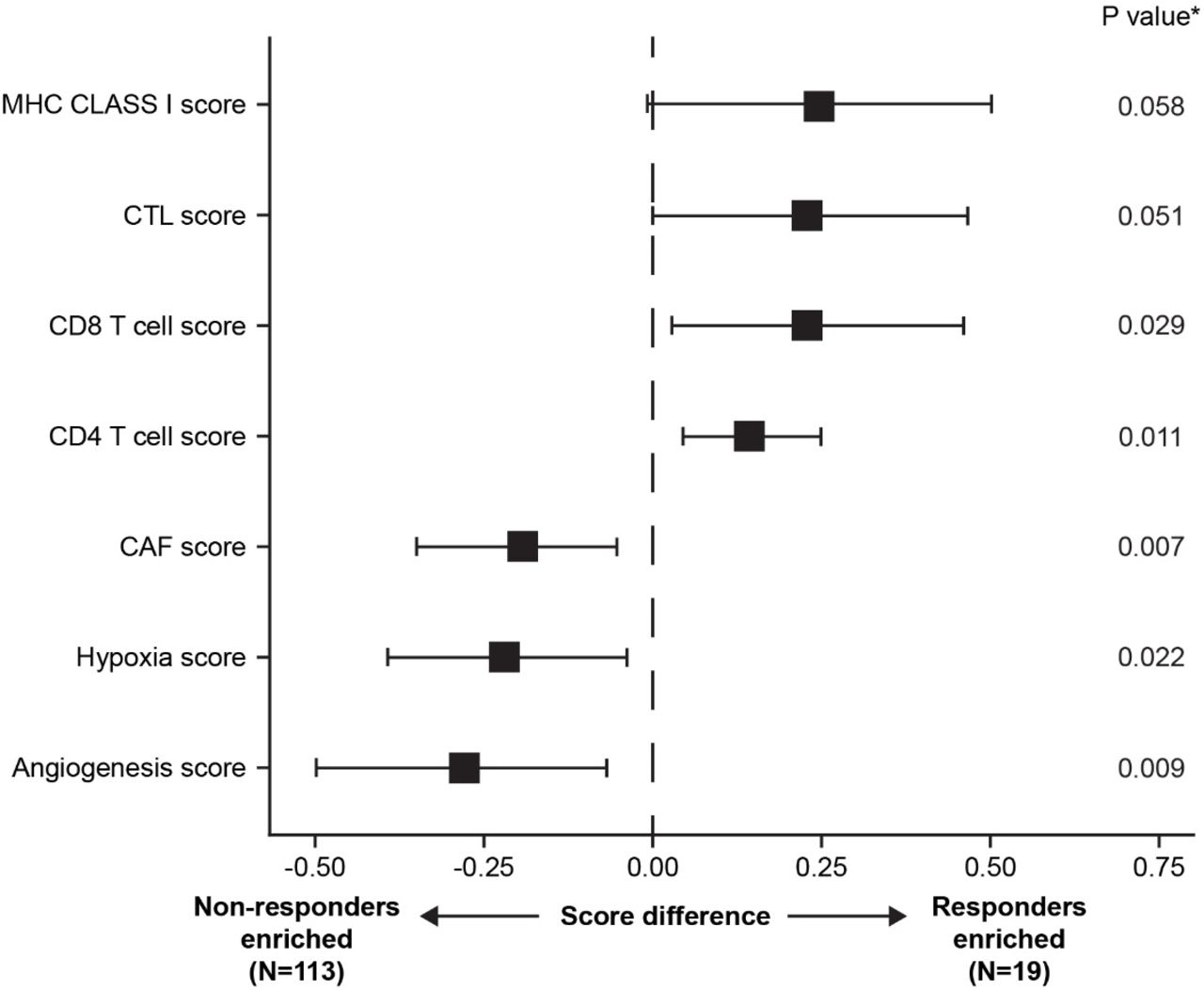
Results 249 patients were enrolled and received ≥1 dose of tislelizumab; 138 patients had evaluable GEP data, of which 132 patients had evaluable GEP and tumor response data. GEP analysis demonstrated that CD4 T cell, CD8 T cell, cytotoxic T lymphocyte and major histocompatibility complex class I signatures were enriched in responders, and cancer-associated fibroblasts, angiogenesis and hypoxia signatures were enriched in NRs (figure 1). CD8B_PDCD1_9, a novel GS identified, comprises 9 genes highly expressed in responders: CD8B, CXCL13, KLRD1, NKG7, HLA-A, HLA-G, LAG3, PDCD1 and KREMEN1. Higher objective response rate (ORR; p<0.0001, by Fisher’s exact test) and longer PFS (p=0.005, by log rank test) were observed in patients with high vs low CD8B_PDCD1_9 score (ORR: 26% vs 3%; median PFS: 2.8 months vs 1.8 months). To explore the heterogeneity of molecular features in NRs, NRs were clustered into 3 subgroups using a series of tumor-immune GS. OS and PFS for the 3 NR subgroups with distinct GS are summarized in table 1.
{kind=link}
Correlation between GS and ORR in patients with previously treated advanced HCC treated with tislelizumab monotherapy
OS and PFS of NR subgroups
Conclusions This exploratory analysis identified distinct GS associated with tumor response and resistance to tislelizumab monotherapy in patients with previously treated advanced HCC and increases our understanding of the tumor microenvironment. Further GEP analyses will be undertaken in an on-going Phase 3 study (NCT03412773).
Acknowledgements This study is sponsored by BeiGene Ltd. Medical writing support for the development of this abstract, under direction of the authors, was provided by Claire White, PhD, of Ashfield MedComms, an Ashfield Health company, and was funded by BeiGene Ltd.
Trial Registration NCT03419897
Ethics Approval This study was conducted according to the ethical principles of the Declaration of Helsinki, Good Clinical Practice guidelines, the principles of informed consent and the requirements of the public registration of clinical trials. Written informed consent was obtained from each patient prior to screening. The protocol was approved by the institutional ethics committee and was monitored by a safety monitoring committee.