Article Text

Abstract
Background Immune checkpoint inhibitors (ICIs) have significantly improved outcomes for patients with numerous cancers. However, these therapies are associated with immune-related adverse events (irAEs), which are inflammatory side effects potentially affecting any organ. Cases of ICI-induced inflammatory arthritis have also been reported. In general, mild irAEs are treated with corticosteroids, while tumour necrosis factor-α (TNFα) inhibitors are reserved for refractory cases. However, prolonged use of TNFα inhibitor (TNFαi) can induce widespread, significant immunosuppression, which can negatively impact the antitumour efficacy of ICI therapy. Therefore, in clinical scenarios where patients develop severe immunotherapy-induced irAEs, an unmet need exists for alternative therapeutic strategies that are effective and without immune dampening effects.
Case reports The anti-interleukin (IL)−6 receptor antibody, tocilizumab, is a biological agent Food and Drug Administration approved for the treatment of rheumatoid arthritis and juvenile idiopathic arthritis. Here, we report on three patients who developed severe polyarthritis while receiving ICI therapy and were treated with tocilizumab. All three patients demonstrated significant clinical improvement; one patient maintained a durable antitumour response derived from checkpoint inhibition.
Conclusions These three cases suggest that anti-IL-6 receptor antibody may be an effective alternative to corticosteroids or TNFαi for the treatment of arthritis irAEs.
- arthritis
- inflammation
- TNF-alpha
- DMARDs(biologic)
Statistics from Altmetric.com
Introduction
Immune checkpoint inhibitors (ICIs) targeting programmed death protein-1 (PD-1) and cytotoxic-T-lymphocyte-antigen-4 (CTLA-4) have revolutionised cancer treatment1; however, ICI therapy can cause immune-related adverse events (irAEs), inflammation of multiple organs.2 Clinical studies demonstrated that inflammatory arthritis can be induced by ICI treatment.3–6 Current guidelines suggest using corticosteroids for mild irAEs, and high-dose corticosteroids or tumour necrosis factor-α inhibitors (TNFαi) for severe irAEs.7 8 However, both corticosteroid and TNFαi can result in serious adverse events.8 In addition, preclinical data demonstrated that TNFα inhibition may dampen ICI therapy antitumour benefits.9 Considering these limitations, alternative therapies are needed for irAEs.
Interleukin (IL)-6 is a cytokine with various biologic activities, including inflammation, immune responses and haematopoiesis.10 Notably, IL-6 is a potent inducer of Th17 cells from naïve CD4+ T cells. Th17, a helper T-cell subset that secretes IL-17, has been reported as a key mediator of many autoimmune diseases including rheumatoid arthritis, inflammatory bowel disease and colitis irAE and there has been recent interest in selectively blocking Th17 induction as a novel treatment strategy for patients with autoimmunity or irAEs.11–13
Here, we report three patients with metastatic melanoma who developed severe arthritis on ICI therapy. Owing to concerns over potentially abrogating the priming phase of antitumour immune response with prolonged TNFαi and considering the growing body of evidence suggesting the pathogenic role of Th17 cells in autoimmunity and irAE development, we treated patients with the anti-IL-6 receptor antibody, tocilizumab.14 Each patient demonstrated significant arthritis improvement.
Case descriptions
Case 1
A 71-year-old man developed metastatic melanoma in the right parotid gland in August 2014 and underwent parotidectomy with lymph node dissection followed by adjuvant radiation therapy. In April 2015, two recurrent melanoma lesions were found in the left pelvis. Treatment was initiated with ipilimumab (anti-CTLA-4 antibody) and palliative cryoablation to the painful pelvic lesions. After completing four ipilimumab treatments, he achieved a complete response (CR).
Subsequently, the patient developed fatigue with severe bilateral shoulder and hip pain. Physical examination revealed mild lethargy without active synovitis. Rheumatological workup was unremarkable except for a weakly positive rheumatoid factor (RF) (27 IU/ml, ULN: 15.9 IU/mL). His polyarthralgia and fatigue with recent ipilimumab exposure suggested arthritis irAE development, and the patient was started on prednisone (50 mg/day; weekly taper by 10 mg). This resulted in symptomatic improvement. However, shortly after the prednisone was tapered off, the patient’s symptoms recurred.
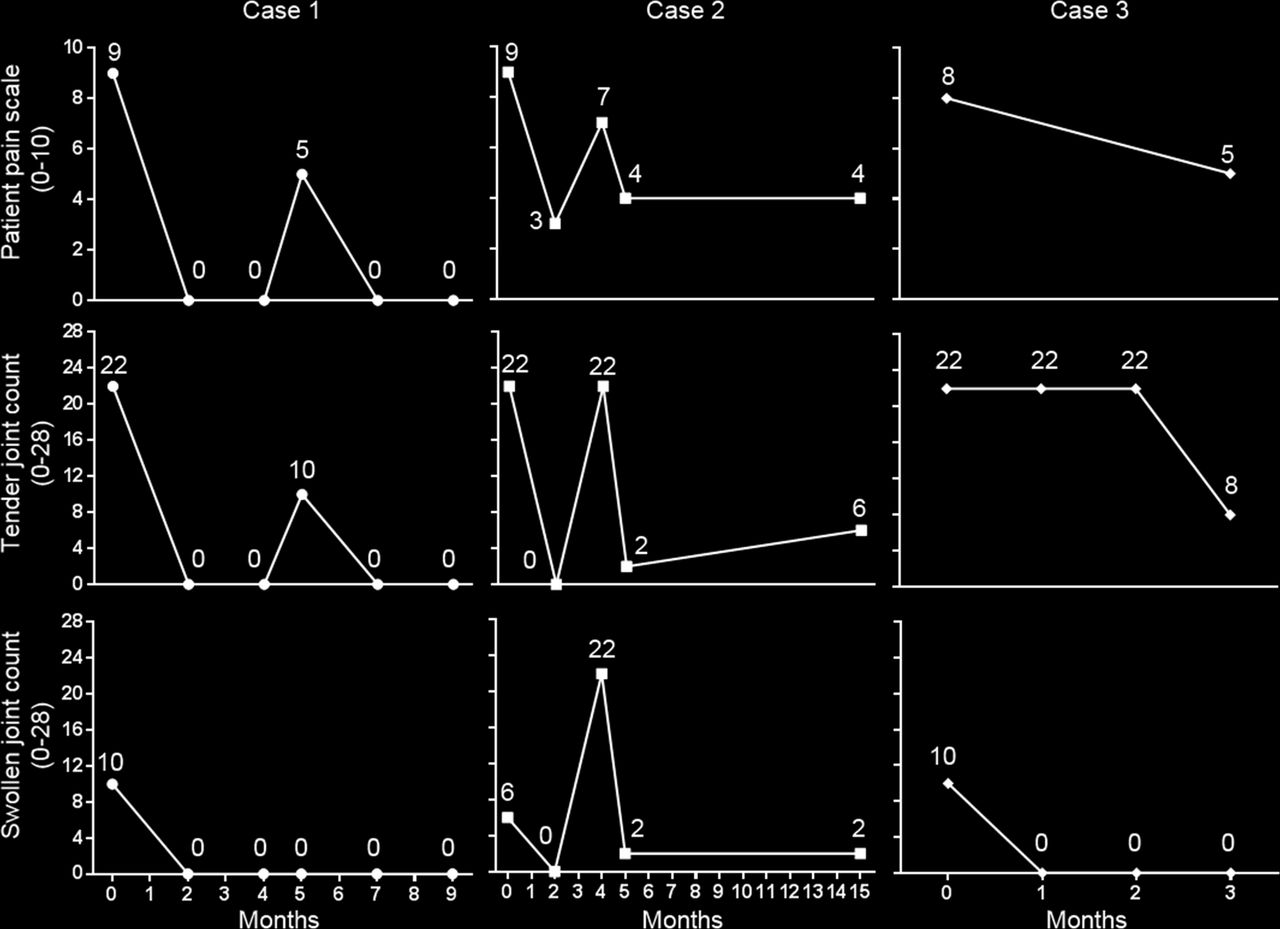
Prednisone was restarted at 40 mg/day. Unfortunately, the patient developed paroxysmal atrial fibrillation and prednisone was discontinued. In January 2016, physical examination revealed tenderness over the bilateral wrists, metacarpophalangeal joints (MCPs), proximal interphalangeal joints (PIPs) and distal interphalangeal joints (DIPs), with active synovitis on all MCPs. To avoid potential antitumour immunosuppression with TNFαi, we initiated tocilizumab (162 mg subcutaneous injection every 2 weeks). Two months later, the patient’s arthritis completely resolved. At 5 months, the patient developed bilateral MCP tenderness which responded to increasing the frequency of tocilizumab to weekly dosing (figure 1). Currently, his arthritis remains in remission with weekly tocilizumab. Prednisone has been tapered and he is currently taking 5 mg/day. Furthermore, he remains in durable CR and does not require further anticancer therapy over 18 months.

{kind=link}
Patient pain scale, tender joint counts, swollen joint counts before (baseline) and after tocilizumab treatment. Measurements performed by a rheumatologist.
Case 2
A 65-year-old man presented with metastatic melanoma of the left elbow in December 2009. He underwent surgical resection followed by adjuvant interferon-α therapy. In May 2012, he developed recurrent disease in the left ileum and received biochemotherapy (dacarbazine, vinblastine, cisplatin and IL-2) followed by radiation therapy resulting in a CR. In August 2014, recurrent disease developed in the chest wall, right thigh and left hip. The patient received four doses of ipilimumab, but experienced disease progression.
Thereafter, patient was started on pembrolizumab (anti-PD-1 antibody). Shortly after receiving the second infusion, the patient developed severe pain and swelling in multiple joints. Examination revealed severe tenderness over the bilateral wrists, MCPs, PIPs and knees with active synovitis in the wrists and knees. Antinuclear antibody (ANA), RF, anti-cyclin citrullinated antibody (anti-CCP) were negative. The patient started prednisone 40 mg/day and his symptoms improved. However, the patient failed to taper prednisone below 20 mg/day and tocilizumab (every 2 weeks) was initiated in September 2015. Eight weeks later, his arthritis significantly improved and prednisone was discontinued (figure 1).
In November 2015, the patient developed progressive tumorous disease, and was started on a clinical trial which required discontinuing tocilizumab. Shortly after, the patient experienced an arthritis flare; tocilizumab was resumed with symptom improvement (figure 1). Currently, 15 months after initiating tocilizumab, his arthritis remains well controlled. He continues to receive tocilizumab while receiving an investigational melanoma therapy.
Case 3
A 46-year-old woman developed melanoma on the lower back in 2009, and underwent surgical resection. In June 2014, she developed recurrent melanoma involving the chest wall, adrenal gland and lung. Mutational analysis revealed a BRAF-V600E mutation and she was started on BRAF-targeted therapy. In March 2015, she developed progressive disease and switched to pembrolizumab. Thereafter, patient developed right adrenal gland haemorrhage and underwent an adrenalectomy.
While on pembrolizumab, the patient developed diarrhoea secondary to colitis irAE and was treated with budesonide with symptomatic improvement. In January 2016, she developed disease progression in the left adrenal gland. At the time, the patient also reported progressive pain and swelling in multiple joints associated with morning stiffness while on pembrolizumab. Physical examination revealed tenderness on both wrists, MCPs, PIPs and ankles, with mild synovitis on PIPs. Two possible incipient erosions on hand X-rays were reported by two different radiologists in left second MCP and right third DIP joints. Laboratory evaluation revealed a positive ANA (1:640 with homogenous pattern) and positive anti-La antibody. RF and anti-CCP antibody were negative. Subsequently, tocilizumab (every 2 weeks) was initiated.
Due to melanoma progression, patient switched therapy to ipilimumab, while remaining on tocilizumab. After 3 months of therapy with tocilizumab, the patient’s joint symptoms improved. Physical examination only showed minimal tenderness over the bilateral second to fourth MCPs without active synovitis (figure 1). Interestingly, while on ipilimumab and tocilizumab, the patient denied any symptoms of colitis/diarrhoea despite being off budesonide. In November 2016, the patient underwent a left adrenalectomy due to haemorrhage. Tocilizumab was held and the patient initiated steroid supplementation for adrenal insufficiency. Repeat hand X-rays showed no radiographic progression. Unfortunately, recent imaging demonstrated melanoma progression and the patient has restarted BRAF-targeted therapy.
Demographic and clinical characteristics of each patient and the effect of tocilizumab on the arthritis irAEs are shown in table 1 and figure 1. Notably, all patients tolerated tocilizumab well without adverse events.
Demographic and clinical characteristics of each case
Discussion
ICI therapy is approved for multiple cancers and our experience with them continues to evolve. While irAEs are currently managed with corticosteroids and/or TNFαi,7 these agents have limitations.
Corticosteroids are known to suppress the ‘priming’ aspect of the immune response and, if used for a prolonged time, may abrogate the ICI-mediated antitumour benefits. In addition, high-dose and/or long-term use of corticosteroids can cause severe systemic toxicity. Despite this, corticosteroids remain the mainstay of therapy for acute irAEs.
The effects of TNFαi on ICI-mediated antitumour benefits are more complicated. Our group (unpublished data) and others have observed that one to two doses of TNFαi for colitis irAE result in faster diarrhoea resolution without negative impacts on overall survival or antitumour response.15 However, effective treatment of arthritis irAE requires prolonged TNFαi, which can potentially dampen the antitumour benefit of ICI therapy.9 Taking these therapy drawbacks into consideration, alternative strategies for treating irAEs are needed.
Although the immune mechanisms underlying irAEs have not been fully elucidated, studies suggest that Th17 cells play a prominent pathogenic role in some autoimmune diseases that resemble irAEs, such as colitis. Importantly, IL-6 promotes Th17 induction and IL-6 inhibition may rebalance the altered Th17-Treg axis without inhibiting the Th1-CD8+ T-cell subsets that govern antitumour immunity.16 We recently reported a patient with metastatic melanoma and concurrent Crohn’s disease who received pembrolizumab and tocilizumab.17 The patient achieved a melanoma CR without exacerbation of the underlying Crohn’s disease. Lastly, although outside the scope of this report, it is worth mentioning that the IL-6 signalling pathway has been shown to play a role in the tumorigenesis of multiple cancers, associated with worse prognosis, and resistance to chemotherapy/immunotherapy.18–21 Therefore, targeting this pathway for cancer treatment is an area of active investigation.22
In conclusion, to our knowledge, this case series is the first report describing that arthritis irAE can be safely managed with tocilizumab while possibly preserving ICI therapy benefits. We recognise that this is a small case series; therefore, these observations are descriptive and we cannot reliably draw definitive conclusions. However, our hypothesis that the IL-6-Th17 pathway plays a significant pathogenic role in arthritis irAE and possibly other irAEs remains intriguing and deserves further investigation in larger patient samples, and ultimately in prospective and controlled studies.
Acknowledgments
None declared.
References
Footnotes
STK, JT, MU and AD contributed equally.
Handling editor Tore K Kvien
Contributors STK, JT, MS-A, MU, DHJ and AD wrote/edited the manuscript. All authors were involved in management of each cases. All authors read and approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.