Article Text

Abstract
Objectives: To investigate factors that may influence the prevalence and timing of appearance of rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies during the preclinical phase of rheumatoid arthritis (RA) development.
Methods: 243 serial prediagnosis serum samples from 83 subjects with RA were examined for the presence of RF and anti-CCP antibodies.
Results: Of the 83 cases, 47 (57%) and 51 (61%) subjects had at least one prediagnosis sample positive for RF or anti-CCP, respectively. Gender and race were not significantly associated with the prevalence or timing of preclinical antibody appearance. Preclinical anti-CCP positivity was strongly associated with the development of erosive RA (odds ratio = 4.64; 95% confidence interval 1.71 to 12.63; p<0.01), but RF was not (p = 0.60). Additionally, as age at the time of diagnosis of RA increased the duration of prediagnosis antibody positivity for RF and anti-CCP increased, with the longest duration of preclinical antibody positivity seen in patients diagnosed with RA over the age of 40. In no subjects did symptom onset precede the appearance of RF or anti-CCP antibodies.
Conclusions: The period of time that RF and anti-CCP are present before diagnosis lengthens as the age at the time of diagnosis of RA increases. This finding suggests that factors such as genetic risk or environmental exposure influencing the temporal relationship between the development of RA-related autoantibodies and clinically apparent disease onset may differ with age.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a systemic, autoimmune, inflammatory disease affecting about 1% of the population.1 It is characterised by joint pain, stiffness and swelling, and can lead to significant morbidity and increased mortality.2
The diagnosis of RA is usually made when a person develops joint symptoms meeting the American Rheumatism Association’s 1987 revised classification criteria.3 Therefore, studies investigating the pathogenesis of disease have largely focused on people with definable symptomatic disease. However, over the past few years, it has become clear that the clinically apparent symptoms of RA are probably a late manifestation of disease-specific immune dysregulation. Supporting this, multiple studies have now shown that RA-related autoantibodies including rheumatoid factor (RF) and highly disease-specific anti-cyclic citrullinated peptide (anti-CCP) antibodies can be present years before the onset of symptoms of RA, and in some cases, combinations of autoantibodies and genetic markers can be highly predictive of future development of RA.4–10
These findings have led to an increased investigative focus on the preclinical period of the disease in order to understand the role of genetic, demographic and environmental factors on the development of RA-related autoimmunity. However, little is known about the relationship between important factors such as age, sex, race and disease severity and the preclinical appearance and behaviour of the biomarkers RF and anti-CCP antibodies.
The purpose of this current study was to use pre-RA diagnosis serum samples from a cohort of subjects with RA selected from the United States Military to investigate the relationship between age, sex, race and disease severity and the presence and timing of appearance of preclinical RA-related autoantibodies.
PATIENTS AND METHODS
Study group
The Department of Defense Serum Repository (DoDSR) was established in 1986 for the purpose of evaluating and improving the health of the United States armed forces. Samples are collected from military members at enlistment, deployment and every other year of service. Currently, the DoDSR houses over 37 million specimens.
For this analysis, the study group included members of the US Military assigned to the North Atlantic Medical Region who were seen at the Walter Reed Army Medical Center (WRAMC) Rheumatology Clinic between 1989 and 2003 with a diagnosis of RA. One hundred and fifty-six cases with RA were identified from this clinic. Of these, 83 were found to have prediagnosis serum samples available in the DoDSR, with 66 (80%) having two or more prediagnosis serum samples, and 39 (47%) having four prediagnosis samples (table 1). The remaining 73 subjects had their diagnosis of RA made before the development of the DoDSR and did not have prediagnosis serum samples available.
Of the 83 cases with prediagnosis serum samples, 81 met at least four of seven criteria for RA based on the 1987 American Rheumatism Association’s revised criteria.3 The remaining two subjects met three of seven criteria and were considered to have RA by board-certified rheumatologists.
Information on gender, race, symptom onset, age at the time of RA diagnosis, seropositivity (RF only) and the presence of radiographic erosions were obtained by chart review at the WRAMC. Based on RF testing as part of clinical management at WRAMC, 67 cases (81%) were classified as seropositive at or after the time of diagnosis (table 1). Information on radiographic erosions was available for 76 (92%) cases, with 42 cases (51%) identified as having erosions at or after the time of diagnosis. Race was categorised as non-Hispanic white, black, and other, with the other category including Hispanics and Asians.
Eighty-three control subjects without RA were selected from the DoDSR in order to provide reference levels of autoantibody measures. These subjects were matched to the cases on gender, age, race and medical region of assignment. They were also matched so that they had serum samples drawn and stored close to the time of the corresponding collections of serum samples from the cases.
All samples were de-identified before autoantibody assessment. After the autoantibody testing was completed, the DoDSR provided the coding key to link the serum samples to subject data. The study protocol was approved by the respective Institutional Review Boards at the WRAMC and the University of Colorado.
Autoantibody assays
Autoantibody assays were performed at the University of Colorado at Denver and the Health Sciences Center Rheumatology Clinical Research Laboratory. RF was measured by nephelometry using polystyrene beads coated with human and sheep γ-globulins, according to manufacturer’s specifications (Dade Behring, Newark, Delaware, USA). The ACR Classification Criteria for RA specifies that a RF level is considered positive if present in <5% of control subjects.3 Accordingly, we determined a general RF cut-off level for positivity of >15.2 IU/ml in all subjects using a 95% cut-off point in single samples from each of the 83 healthy military control subjects. Additionally, to account for possible age-related changes in RF levels, we determined age-specific cut-off points for RF positivity using the same military control samples divided into the following age categories: 20–29, 30–39, 40–49 and 50+.
The anti-CCP 2 ELISA assay was used to measure IgG antibodies to CCP (Diastat, Axis-Shield Diagnostics, Ltd., Dundee, Scotland, UK). According to the manufacturer’s specifications, a positive test was defined as a level of >5 U/ml. None of the control subjects were positive for anti-CCP. For anti-CCP, an age-specific cut-off point was not determined as no controls had levels >5 U/ml. Moreover, previous studies of unaffected control populations did not find any differences in rates of antibodies against citrullinated antigens related to age.11
Statistical analysis
The prevalence of prediagnosis antibody positivity was determined using data from all 83 cases, with a single RF cut-off point of >15.2 IU/ml. The relationship between the variables gender, race, age at time of diagnosis of RA and erosive disease to the presence of prediagnosis RF or anti-CCP was analysed using logistic regression modelling. The associations of RF or anti-CCP positivity with each of these variables are reported as odds ratios (ORs) with 95% confidence intervals (CIs) and corresponding p values.
For each antibody (RF and anti-CCP), the timing of appearance and duration of positivity in the prediagnosis period was analysed separately by a parametric Weibull survival model taking into account interval and left censorship, and using only those subjects positive for RF or anti-CCP during the preclinical period. The serum samples were analysed “backwards” in time, with the earliest appearance of antibody considered as the event. This reversal of the time axis in survival analysis is a standard method for retrospective analysis of left censored observations.12
A subset of cases was positive for RA-related antibodies in the earliest available serum sample (table 2). Thus, the true time of prediagnosis antibody positivity may have been earlier than the initial sample. We accounted for this with left censoring in the survival analysis of all subjects with prediagnosis antibody positivity, including those whose first available sample was antibody positive. In addition, we performed survival analyses using only those subjects who converted from negative to positive antibody status during the preclinical period. In both of these analyses (first sample-positive subjects and converters), survival models with interval censoring were used as it is assumed that subjects become positive for the antibody during the time interval between antibody negative and positive samples.
Survival analysis was also performed to evaluate the influence of the cases’ characteristics on the timing of prediagnosis antibody appearance. Variables considered a priori to be potential influences on the timing of preclinical autoantibody positivity were age at the time of diagnosis of RA (in 10-year intervals), sex, race, the presence of erosions and the duration of preclinical samples available. Comparisons between survival curves are reported as hazard ratios (HRs) with associated 95% CIs and p values. Additionally, an overall test for trend of increased duration of prediagnosis antibody positivity with increasing age was evaluated by including the age category as a continuous covariate in the Weibull survival model.
The sequence of appearance of RF and anti-CCP in the prediagnosis period was analysed using a parametric interval censored survival model for clustered data.13 All analyses were performed using SAS version 9.1.
RESULTS
Patient group
Table 1 presents the demographics and clinical features of the military RA cases, including age at diagnosis, gender, race, presence of erosive disease and RF positivity at diagnosis. A total of 243 prediagnosis serum samples were available from cases with a mean of 2.9 samples per case (range 1–4). Samples were available a mean of 6.6 years (range 0.1–13.7) before RA diagnosis.
Prediagnosis antibody prevalence
Of the 83 subjects with RA, 47 (57%) were RF positive and 51 (61%) were anti-CCP positive before diagnosis (tables 2 and 3). Additionally, 57 (69%) were positive for either RF or anti-CCP before diagnosis, and 41 (49%) had at least one preclinical sample positive for both antibodies. Of the RF and anti-CCP positive cases, 22/47 (47%) and 22/51 (43%), respectively, were positive for these antibodies in their earliest available prediagnosis serum sample.
Factors associated with prediagnosis antibody positivity
Prediagnosis RF or anti-CCP positivity was not significantly associated with sex, race and age at diagnosis. Prediagnosis RF positivity was not associated with the development of erosive RA; however, prediagnosis anti-CCP positivity was strongly associated with the development of erosive RA (OR = 4.64; 95% CI 1.71 to 12.63; p<0.01) (table 4). This association persisted after controlling for RF in anti-CCP positive cases.
Sequence of appearance of RF and anti-CCP in the prediagnosis period
In all subjects with prediagnosis antibody positivity, RF was present a median of 6.0 years before RA diagnosis (95% CI 4.5 to 8.0). Anti-CCP was present a median of 5.4 years before diagnosis (95% CI 4.1 to 7.1). This difference in duration of preclinical antibody positivity was not significant (p = 0.78). In analysis using only those subjects known to have converted to antibody positive status in the preclinical period, RF was present a median of 3.6 years before diagnosis (95% CI 2.7 to 4.8), and anti-CCP was present a median of 3.4 years before diagnosis (95% CI 2.6 to 4.4).
Factors affecting the timing of appearance of antibody positivity in the prediagnosis period
In univariate analysis, gender, race, and erosive disease were not significantly associated with longer duration of prediagnosis RF and anti-CCP positivity. However, increased age-at-diagnosis of RA (in 10-year intervals) was associated with longer duration of RF and anti-CCP positivity in the prediagnosis period (fig 1, tables 5 and 6).
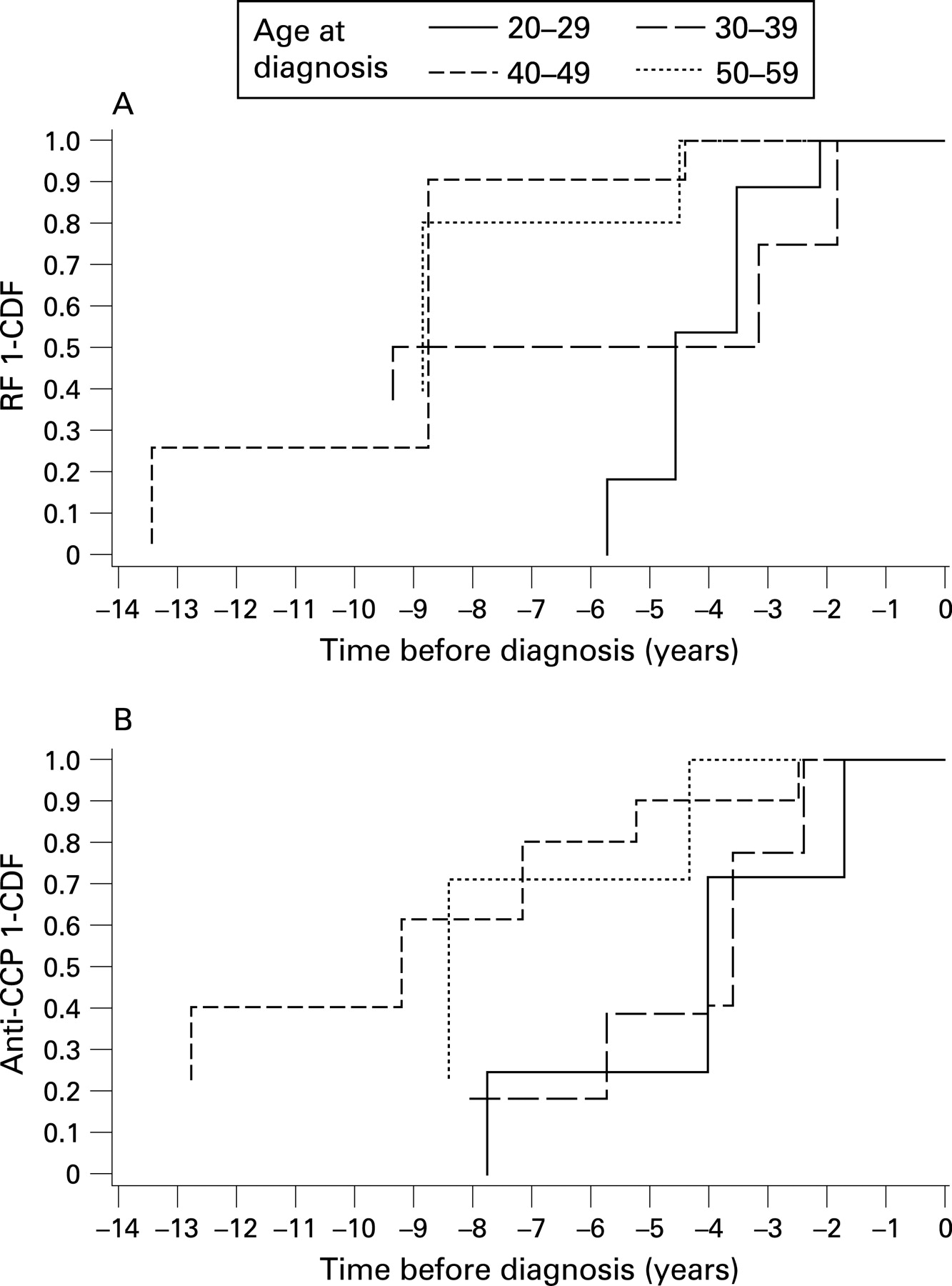
In survival analysis controlling for age, sex, and the duration of preclinical samples available, for both RF and anti-CCP, as age at diagnosis increased by 10-year intervals, the duration of preclinical antibody positivity increased (fig 1, tables 5 and 6). For RF using all subjects with prediagnosis antibody positivity (n = 47), the age group 50+ had a significantly longer duration of preclinical antibody positivity than the referent age group (20–29-year-olds) (HR = 0.14; 95% CI 0.02 to 0.83; p = 0.04) (table 5). There was also a longer duration of preclinical antibody positivity in the 30–39-year-old and 40–49-year-old age groups than in the youngest age group, although no HR reached statistical significance (table 5).
For anti-CCP, using all subjects with prediagnosis antibody positivity (n = 51), the 40–49 age group had a significantly longer duration of preclinical antibody positivity than the referent group (HR = 0.16; 95% CI 0.04 to 0.68; p = 0.02) (table 6). There was also a longer duration of antibody positivity in the 30–39 and 50+ year-old age-at-diagnosis groups than in the youngest age group, although no HR reached statistical significance (table 6).
In trend analysis, longer duration of prediagnosis antibody positivity with increased age-at-diagnosis of RA (in 10-year intervals) was significant for RF (p = 0.03) and marginally significant for anti-CCP (p = 0.07) (fig 2).

{kind=link}
{kind=link}
Univariate analysis was also performed using only subjects with preclinical antibody conversion from negative to positive. For RF converters (n = 25), the age group 40–49 had significantly longer duration of preclinical antibody positive than the age group 20–29 (HR = 0.21; 95% CI 0.06 to 0.72, p<0.01). For anti-CCP converters (n = 29), the age group 40–49 had significantly longer duration of preclinical antibody positivity than the 20–29 year-olds (HR = 0.14; 95% CI 0.04 to 0.51; p⩽0.01). In addition, trend analysis for RF and anti-CCP in these converters showed significant increase in the duration of preclinical antibody positivity with increasing age (for RF, p = 0.02; for anti-CCP, p = 0.01).
Antibody appearance in relationship to symptom onset
Symptoms of RA during the prediagnosis period were obtained by chart review and were defined as pain, stiffness or swelling in peripheral joints. Symptoms were present a median of 0.5 years before diagnosis, regardless of preclinical antibody status or age at diagnosis.
Of the 57 subjects with RF or anti-CCP present before the diagnosis of RA, 47 (82.5%) had antibodies appear before symptom onset. In the other 10 subjects, data were insufficient to determine the median time of antibody appearance before symptom onset; however, none of the subjects could be classified as reporting symptoms before the appearance of autoantibodies.
DISCUSSION
We used the resources of the WRAMC Rheumatology Clinic and the DoDSR to examine serial stored serum samples for the presence of RA-related autoimmunity in the prediagnosis period. Of the 83 cases of RA examined, 57% and 61% of subjects exhibited RF and anti-CCP antibody positivity, respectively, before diagnosis. Sex, race and age at diagnosis did not significantly influence the prevalence of preclinical antibody positivity. However, the presence of preclinical anti-CCP positivity (but not RF) was associated with a significantly increased risk for the development of erosive disease—a finding similar to that recently published by Berglin et al.14
Our reported prevalence rates of preclinical RF and anti-CCP positivity are higher than those previously reported. Nielen et al found a preclinical prevalence of RF of 28% and anti-CCP of 41%, and Rantapaa-Dahlqvist et al reported the prevalence of RF of 19% and anti-CCP of 34%.4 5 This may reflect methodological differences in RF or anti-CCP antibody testing, or study design variations such as ascertainment of diagnosis of RA and symptom data. It is also possible that these differences reflect immunological differences in RA in the differing populations or differences in genetics or exposures to risk factors for autoimmunity.15 16 Another possible explanation for this finding is that, although the military RA cases were not preferentially selected based on RF positivity, there may have been some selection bias in the original inclusion of these subjects in the military clinic from which they were chosen.
The association of the presence of preclinical anti-CCP, but not RF, with erosive disease may be explained by recent assertions that anti-CCP has a direct pathogenic role in joint inflammation. This is supported by recent work which showed that the addition of antibodies to citrullinated peptides significantly enhances joint inflammation in mouse models of collagen-induced inflammatory arthritis.17 Also, human studies have shown that anti-CCP measured after RA diagnosis may be more strongly related to erosive disease than RF.18 Interestingly, in this military RA cohort, the duration of preclinical anti-CCP positivity was not associated with a higher risk for erosive disease. This will need further exploration in future studies.
Most strikingly, we found that subjects who were older at the time of diagnosis of RA had a significantly longer duration of preclinical autoantibody positivity. This may seem at first glance to be due to the possibility of longer prediagnosis symptoms or greater duration of stored serum samples available in older military subjects with RA. However, symptoms of RA were not present earlier in older versus younger subjects, and the increased duration of preclinical antibody positivity persisted after controlling statistically for the duration of preclinical samples available.
There is controversy about whether levels of RF may increase as a result of age, with some studies showing age-associated increases and others not.19–21 In this study, using a single RF cut-off point (>15.2 IU/ml), there was a trend towards decreased RF positivity in older cases. In addition, we also evaluated the prevalence and duration of prediagnosis RF positivity using age specific cut-off points for RF determined in the military control population. Using these cut-off points, we found no significant differences in the prevalence of prediagnosis RF positivity, and in all RF positive cases as well as RF converters only, we found results similar to those in our original analysis, with the duration of prediagnosis RF positivity increasing as age at diagnosis increased in survival models and in trend analysis (data not shown). These findings are consistent in this study with a lack of confounding effect of increasing background rates of RF positivity in older subjects. For anti-CCP, current publications suggest that levels of antibodies against citrullinated proteins are not non-specifically raised in older subjects.11 In our analysis, as none of our controls had CCP levels >5 U/ml, age-specific cut-off points were not determined. Additionally, using the standardised anti-CCP cut-off point, there was a non-significant trend towards decreased anti-CCP positivity in older subjects with RA.
Several mechanisms might explain the increased duration of preclinical antibody positivity as age at diagnosis of RA increases. Biological senescence may lead to alterations in the dynamics between initial immune dysregulation and the onset of clinically apparent disease.22 Because of this, in an older person, even though RA-specific autoimmune dysregulation and autoantibody production may be present, the effector mechanisms necessary for the development of clinical disease may be impaired, leading to a longer period of time between antibody positivity and clinically apparent joint disease.
Another explanation is that the relationship between genetic factors and environmental exposures may differ as age at diagnosis changes.23 24 For example, in a subject with younger-onset disease, the genetic contributions to RA development may be greater, requiring less environmental exposures over a shorter period of time to trigger disease than someone who develops RA later in life. In addition, environmental exposures that possibly lead to RA-related immune dysregulation may differ in younger versus older disease onset age groups. For example, in subjects with disease onset at a young age there may be a robust environmental exposure, such as infection which acts as the triggering mechanism for RA, leading to a short period of time between detectable preclinical autoimmunity and clinically apparent disease. Conversely, in older patients, environmental influences on disease that are more dependent on long-term cumulative exposures such as smoking or intake of dietary components may predominate in the disease risk.15 16
Study limitations
In this military population with RA, the high prevalence of men (59%) and the low mean age at RA diagnosis (39.9 years) make this group less representative of RA in the general population. In addition, the severity of RA may have influenced resignation from the military, with younger subjects with severe disease leaving service early, leading to a preponderance of less severe disease in subjects who were older at the time of diagnosis. However, in this cohort, erosive disease was not significantly more prevalent in the younger subjects. Also, given the close evaluation of all military personnel with joint complaints, and the focus of our analysis on age at the time of diagnosis, we believe that differences in disease severity minimally influenced our findings of increasing duration of preclinical antibody positivity as age at diagnosis increased.
There are limited previous data suggesting that race may influence RA-related autoantibody positivity.25–30 In our analysis, we did not find a significant relationship between race and preclinical prevalence rates of RF or anti-CCP positivity (table 3), but it is possible that associations do exist that were not identified owing to small sample sizes and limited information, and future studies with larger numbers of subjects will need to be performed. Additionally, as tobacco smoke may be a major environmental influence on the development of RA-related autoimmunity, an analysis of the effect of smoking on the prevalence and timing of RA autoantibodies would be beneficial. Owing to the unavailability of tobacco use data in this cohort, we were unable to examine the influence of smoking on the prevalence and duration of preclinical antibody positivity, and this will have to be explored in future studies. Lastly, the sample size for this study was relatively small, and results will need to be verified in larger prospective studies which are currently underway.
CONCLUSION
Based on our findings in this study, the period of time that RF and anti-CCP are present before diagnosis lengthens as the age at the time of diagnosis of RA increases. This new finding adds to the knowledge of the preclinical period of RA development and suggests that factors such as genetic risk, environmental exposures and immune system senescence may influence the temporal relationship between the development of preclinical RA-related autoantibodies and age at symptom onset. In addition, this finding has implications for the use of autoantibody biomarkers as predictive markers for risk of development of RA in asymptomatic subjects, with antibody positivity potentially having a very different meaning for the timing of onset of symptomatic RA in a younger versus an older person. Further prospective studies are needed to characterise the genetic, epidemiological and immunological factors that influence the development of RA.
Acknowledgments
We thank Drs Sterling West and George Tsokos for informative discussions and help related to this project.
REFERENCES
Footnotes
DSM and KDD contributed equally to the study.
Funding: These studies were supported by R21 AI61479, T32 AR07534, Arthritis Foundation/American College of Rheumatology Physician Scientist Development Award, K12 RR017707, K23 AR051461 and the Smyth Professorship in Rheumatology.
Competing interests: None.
DSM participated in the design and analysis of this study and the writing of this manuscript. KDD participated in the analysis of data and preparation of the manuscript. LAP participated in the analysis of samples and data and preparation of the manuscript. AAL and AEB contributed statistical expertise in the analysis of data for this manuscript. CWW participated in subject evaluation and determination of eligibility for this study. MVR participated in the design of this study and procurement of the serum samples for analysis. WRG participated in the design of this study and procurement of the serum samples for analysis, as well as subject evaluation and determination of eligibility for this study. JMN participated in the design and analysis of this study and preparation of the manuscript. VMH participated in the design and analysis of this study, antibody testing, and manuscript preparation.
Disclaimer: The views expressed in this abstract are those of the authors and do not reflect the official policy of the Department of the Army, Department of Defence, or US Government.