Article Text

Abstract
Background Merkel cell carcinoma (MCC) is a rare, aggressive skin cancer associated with poor survival outcomes in patients with distant metastatic disease (mMCC). In an initial analysis from JAVELIN Merkel 200, a phase 2, prospective, open-label, single-arm trial in mMCC, avelumab—a human anti–programmed death-ligand 1 (PD-L1) monoclonal antibody—showed promising efficacy and a safety profile that was generally manageable and tolerable. Here, we report the efficacy of avelumab after ≥1 year of follow-up in patients with distant mMCC that had progressed following prior chemotherapy for metastatic disease.
Patients and methods Patients received avelumab 10 mg/kg by 1-h intravenous infusion every 2 weeks until confirmed disease progression, unacceptable toxicity, or withdrawal. The primary endpoint was best overall response. Secondary endpoints included duration of response (DOR), progression-free survival (PFS), and overall survival (OS).
Results Patients (N = 88) were followed for a minimum of 12 months. The confirmed objective response rate was 33.0% (95% CI, 23.3%-43.8%; complete response: 11.4%). An estimated 74% of responses lasted ≥1 year, and 72.4% of responses were ongoing at data cutoff. Responses were durable, with the median DOR not yet reached (95% CI, 18.0 months-not estimable), and PFS was prolonged; 1-year PFS and OS rates were 30% (95% CI, 21%-41%) and 52% (95% CI, 41%-62%), respectively. Median OS was 12.9 months (95% CI, 7.5-not estimable). Subgroup analyses suggested a higher probability of response in patients receiving fewer prior lines of systemic therapy, with a lower baseline disease burden, and with PD-L1–positive tumors; however, durable responses occurred irrespective of baseline factors, including tumor Merkel cell polyomavirus status.
Conclusions With longer follow-up, avelumab continues to show durable responses and promising survival outcomes in patients with distant mMCC whose disease had progressed after chemotherapy.
Trial registration Clinicaltrials.gov identifier: NCT02155647.
- Javelin
- Avelumab
- Merkel cell carcinoma
- Pd-L1
- 2 L
- Second-line
- 2 L +
- Second-line or later
- CI
- Confidence interval
- CR
- Complete response
- DOR
- Duration of response
- DRR
- Durable response rate
- ECOG
- Eastern Cooperative Oncology Group
- FDA
- Food and Drug Administration
- HIV
- Human immunodeficiency virus
- MCPyV
- Merkel cell polyomavirus
- MMCC
- Metastatic Merkel cell carcinoma
- NE
- Not estimable
- NR
- Not yet reached
- ORR
- Objective response rate
- OS
- Overall survival
- PD
- Progressive disease
- PD-1
- Programmed death-1
- PD-L1
- Programmed death-ligand 1
- PFS
- Progression-free survival
- PR
- Partial response
- RECIST
- Response Evaluation Criteria In Solid Tumors
- SLD
- Sum of target lesion diameters
- UV
- Ultraviolet
Open AccessThis article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Statistics from Altmetric.com
Introduction
Merkel cell carcinoma (MCC) is a rare, aggressive skin cancer associated with clonal integration of Merkel cell polyomavirus (MCPyV), accumulation of UV-induced DNA mutations, immunosuppression, and old age [1, 2]. Up to 12% of patients with MCC have distant metastatic disease (mMCC), which has a poor prognosis [1, 3], and progression to mMCC is frequent in patients with local or regional disease (up to 21%) [4]. Although no prospective clinical trials of chemotherapy have been conducted and no regimen has been specifically approved for mMCC treatment, platinum/etoposide combinations have been widely used and achieve relatively high objective response rates (ORRs); response duration, however, is short and no clear survival advantage has been reported [5, 6], highlighting the need for alternative treatments. Recently, clinical trials with immune checkpoint inhibitors targeting the programmed death-ligand 1 (PD-L1)/programmed death 1 (PD-1) interaction have shown clinical activity and durable responses in patients with advanced MCC [7–9]. Based on findings from an open-label, single-arm, prospective, phase 2 trial [8], avelumab—a human anti–PD-L1 monoclonal antibody—became the first treatment approved by the US Food and Drug Administration (FDA) for patients with mMCC [10]. Here, we report updated efficacy data for avelumab with ≥1 year of follow-up in patients with mMCC that had progressed after ≥1 prior line of chemotherapy for metastatic disease.
Methods
Study design and patients
The procedures for analysis and design of the JAVELIN Merkel 200 trial (NCT02155647) were reported previously [8]. Briefly, patients with histologically confirmed stage IV MCC that had progressed following ≥1 prior line of chemotherapy for metastatic disease, were enrolled. Eligible patients were adults aged ≥18 years who had Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, an estimated life expectancy of ≥3 months, ≥1 unidimensional measurable lesion by Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1 [11], and adequate hematological, hepatic, and renal function. Patients who received previous therapy with immune checkpoint inhibitor or concurrent anticancer treatment, systemic treatment with corticosteroids, or those with HIV, immunosuppression, previous organ transplant, hematological malignancies, or clinically significant comorbidities were excluded. Patients were not selected based on tumor PD-L1 expression or MCPyV status. Patients received avelumab 10 mg/kg by 1-h intravenous infusion every 2 weeks until confirmed disease progression, unacceptable toxicity, or occurrence of any other criterion for withdrawal.
Outcomes and statistical analysis
The primary endpoint was best overall response—defined as complete response (CR), partial response (PR), stable disease, or progressive disease per RECIST v1.1—and was evaluated by an independent review committee every 6 weeks. Secondary endpoints included duration of response (DOR), progression-free survival (PFS), and overall survival (OS), and a post hoc analysis was carried out to determine the 6-month durable response rate (DRR) [8]. Time-to-event endpoints were analyzed by Kaplan-Meier methods; medians were calculated with corresponding CIs using the Brookmeyer-Crowley method. Safety data are summarized in aggregate for this report and are reported elsewhere [10, 12].
Results
Baseline characteristics of the 88 patients enrolled and treated with avelumab were reported previously [8]. Briefly, median age was 72.5 years (range, 64.5-77.0), 65 patients (74%) were male, 47 patients (53.4%) had visceral disease at baseline (ie, any lesions identified in sites other than skin, eye, or lymph nodes by independent review), 49 (55.7%) and 39 (44.3%) had an ECOG performance status score of 0 or 1, and 52 (59.1%), 26 (29.5%), and 10 patients (11.4%) had received 1, 2, or ≥3 prior lines of anticancer treatment, respectively.
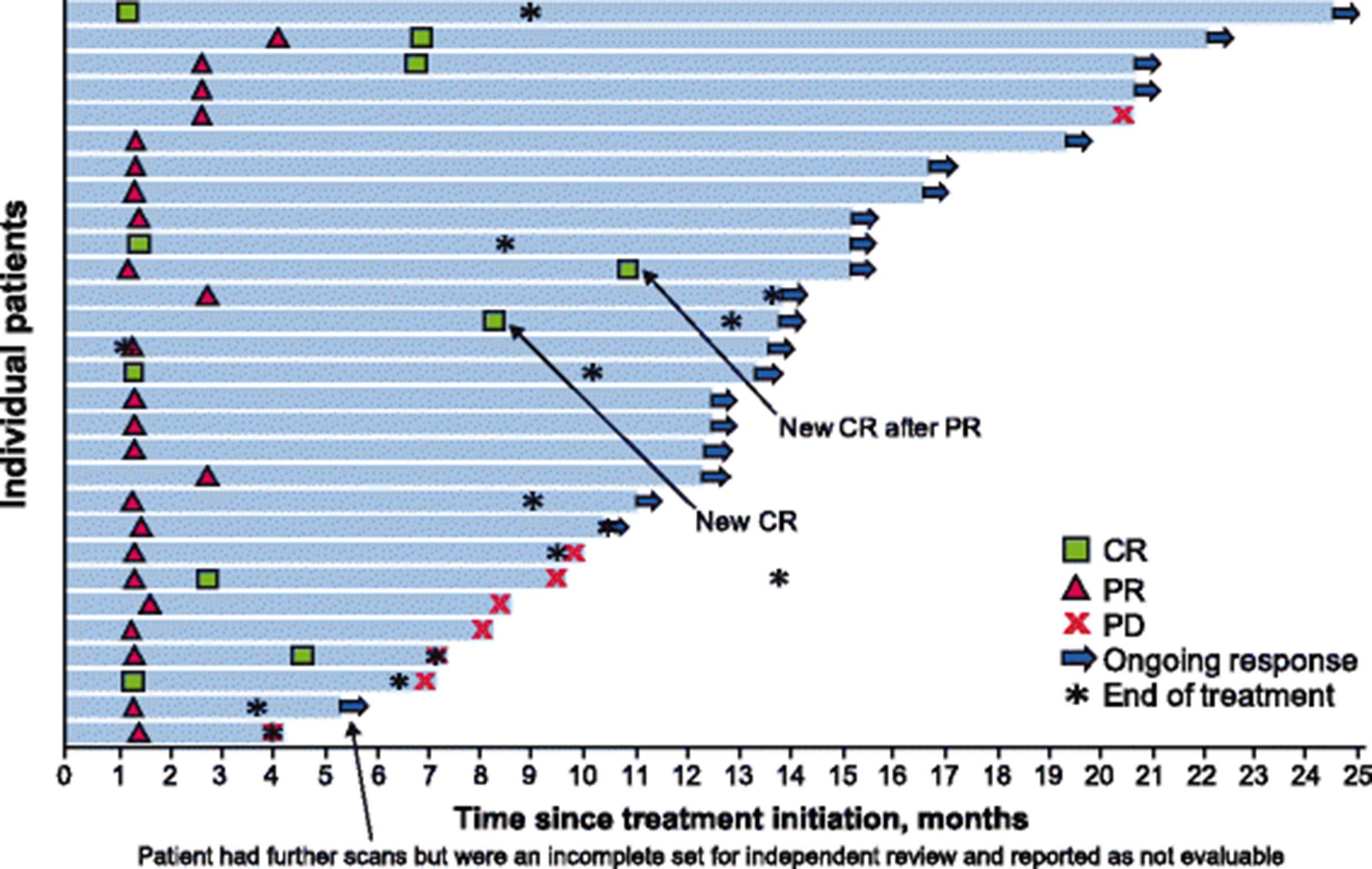
As of September 3, 2016 (data cutoff date), median follow-up was 16.4 months (range, 12.1-25.4). Treatment was ongoing in 19 patients (21.6%), and 69 patients (78.4%) had discontinued treatment—mostly due to disease progression (n = 44 [63.8%]) or adverse events (n = 7 [10.1%]), which were treatment-related in 6 patients and included ileus and transaminitis. Ten patients (11.4%) had a confirmed CR, including 2 new CRs since the primary analysis [8], and 19 patients (21.6%) had a PR, resulting in an ORR of 33.0% (95% CI, 23.3%-43.8%) (Table 1). Median time to response was 6.1 weeks (range, 6-36), with 22 of 29 responses (75.9%) observed 6 weeks after treatment initiation. Responses were ongoing at data cutoff in 21 of 29 patients (72.4%), including in 9 patients (31.0%) who had reached the end of treatment (Fig. 1). Responses were durable, with the median DOR not yet reached; the lower bound for the 95% CI was 18.0 months, and the longest observed DOR was 23.3 months in a patient with ongoing response (Table 1, Fig. 1). The estimated proportion of responses with a duration ≥1 year was 74% (95% CI, 53%-87%). The 6-month DRR was 30.6% (95% CI, 20.9%-40.3%), and the overall proportion of patients in response at 1 year after treatment initiation was 23.9% (95% CI, 15.4%-34.1%).
Efficacy of avelumab after ≥6 months and ≥1 year of follow-up
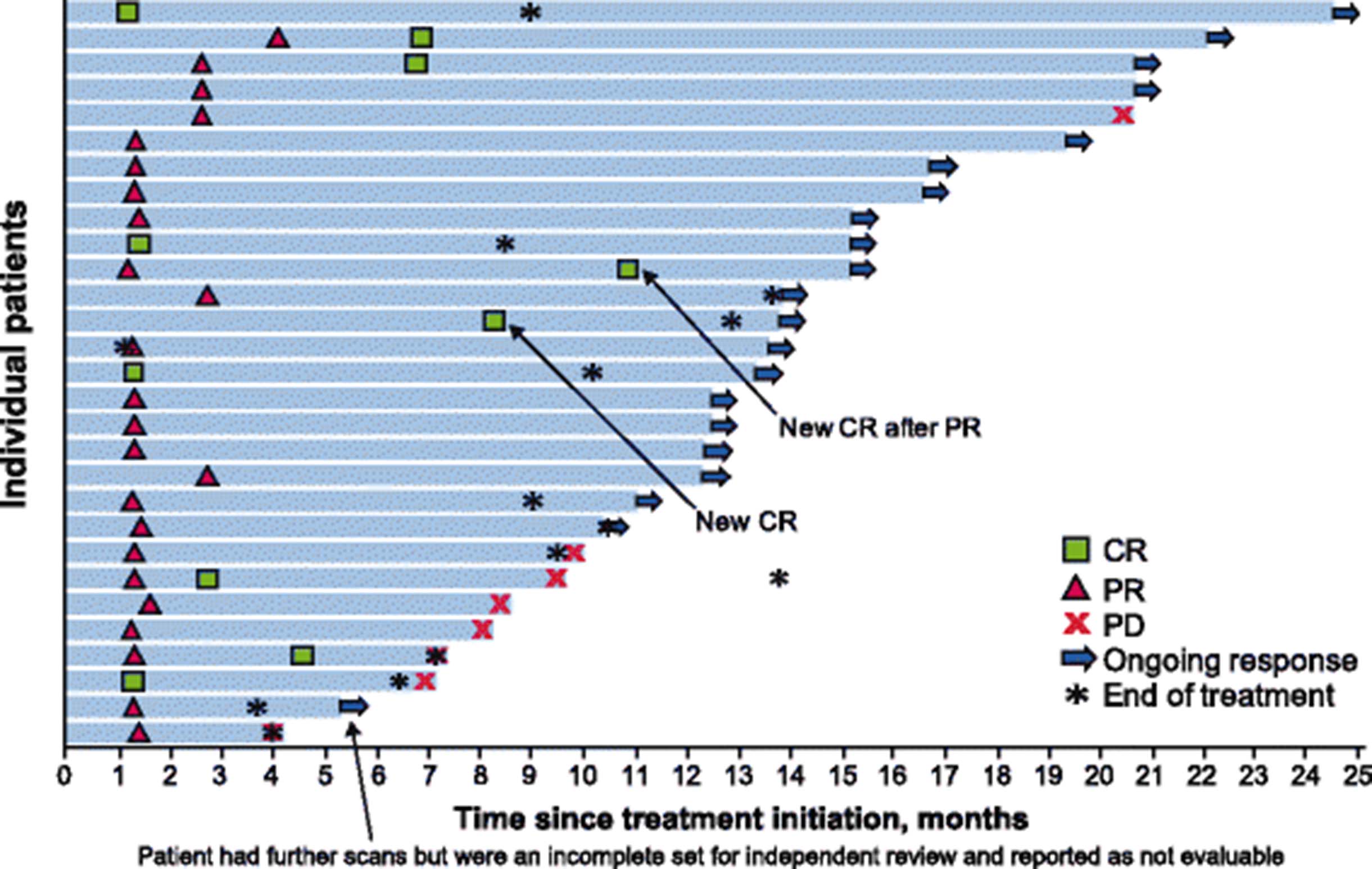
Clinical activity of avelumab in patients with mMCC at ≥1 year of follow-up. Time to and duration of response and duration of treatment in 29 patients with a confirmed response. CR, complete response; DOR, duration of response; PD, progressive disease; PR, partial response
The 1-year PFS rate was 30% (95% CI, 21%-41%), and median PFS was 2.7 months (95% CI, 1.4-6.9); the maximum time reported at cutoff was 24.5 months (Fig. 2a). For illustrative purposes, Kaplan-Meier estimates of PFS from recent studies of second-line or later chemotherapy for mMCC are also depicted [13–15]. Median OS was 12.9 months (95% CI, 7.5-not estimable), and the 1-year OS rate was 52% (95% CI, 41%-62%) (Fig. 2b).
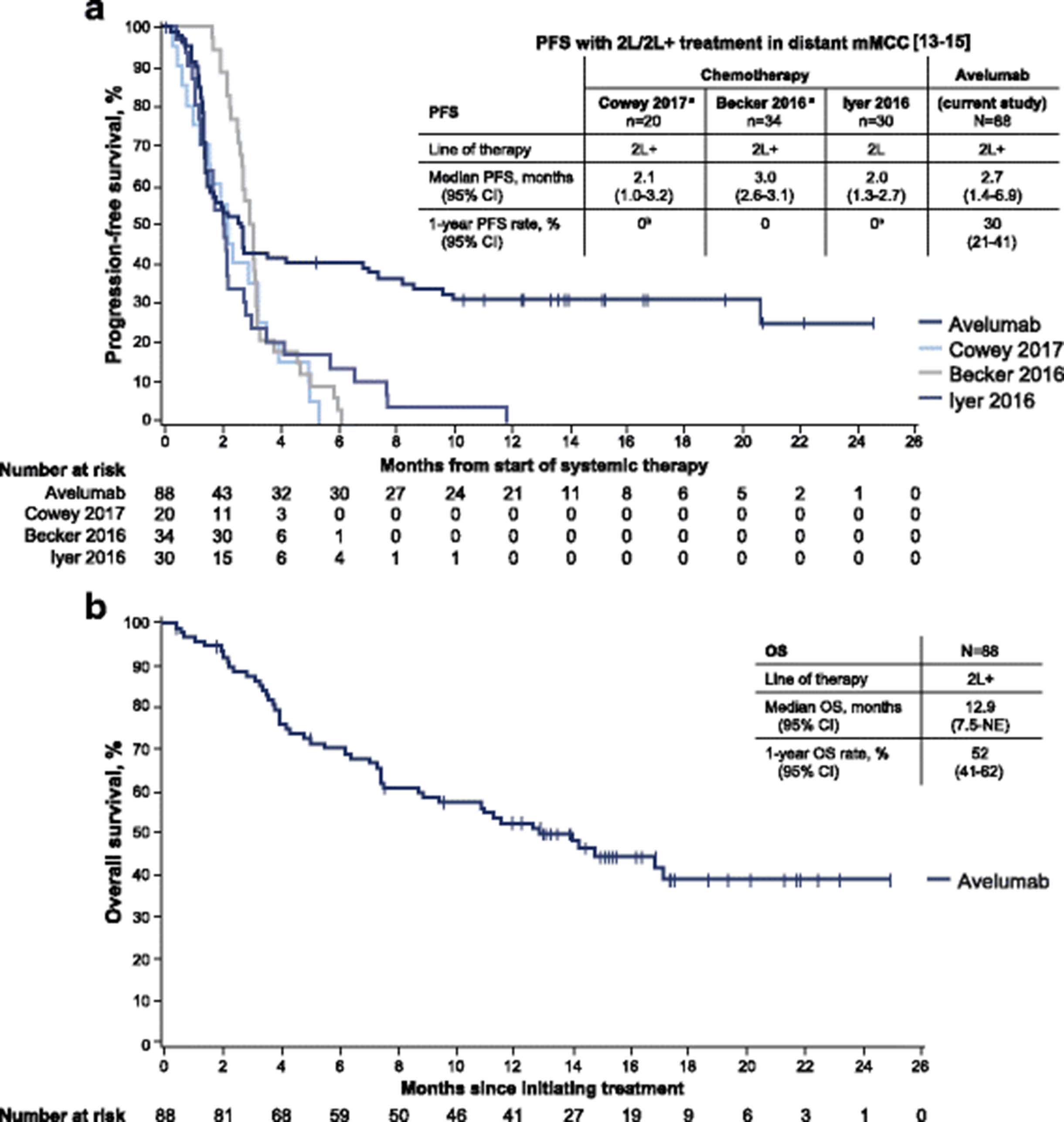
Survival outcomes in patients with mMCC receiving avelumab. Kaplan-Meier estimates of (a) progression-free survival (PFS) and (b) overall survival (OS). Vertical lines indicate censored events. Also depicted in (a) are Kaplan-Meier estimates of PFS for recent retrospective studies of second-line (2 L) or second-line and later (2 L+) chemotherapy in patients with mMCC [13–15]. NE, not estimable. a Includes both immunocompetent and immunocompromised patients. All patients progressed; therefore, none were censored. b PFS rate at 6 months was 0%. c One patient with PR had PFS lasting 354 days; 95% of patients receiving second-line chemotherapy had progressed at 230 days
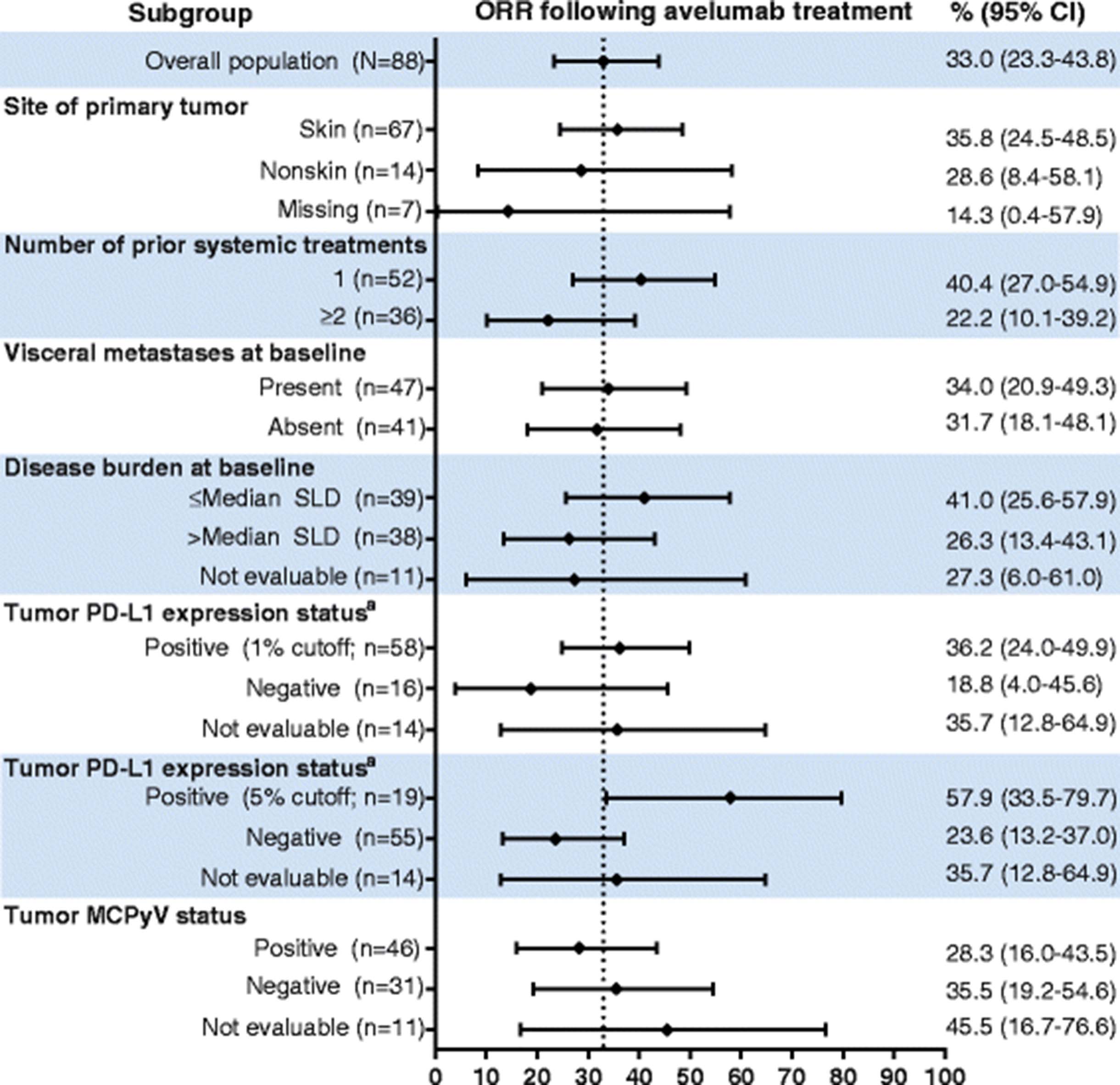
Subgroup analyses showed trends for higher ORR in patients who received fewer prior lines of anticancer treatment (1 vs ≥2 prior lines, 40.4% vs 22.2%), with lower disease burden (sum of target lesion diameters ≤ median vs > median, 41.0% vs 26.3%), and with PD-L1–positive tumors (1% threshold by immunohistochemistry, 36.2% vs 18.8% for PD-L1–negative tumors; 5% threshold by immunohistochemistry, 57.9% vs 23.6% for PD-L1–negative tumors) (Fig. 3). The proportions of responses with ≥1-year duration were similar across evaluable subgroups, including tumor MCPyV status (Fig. 4).
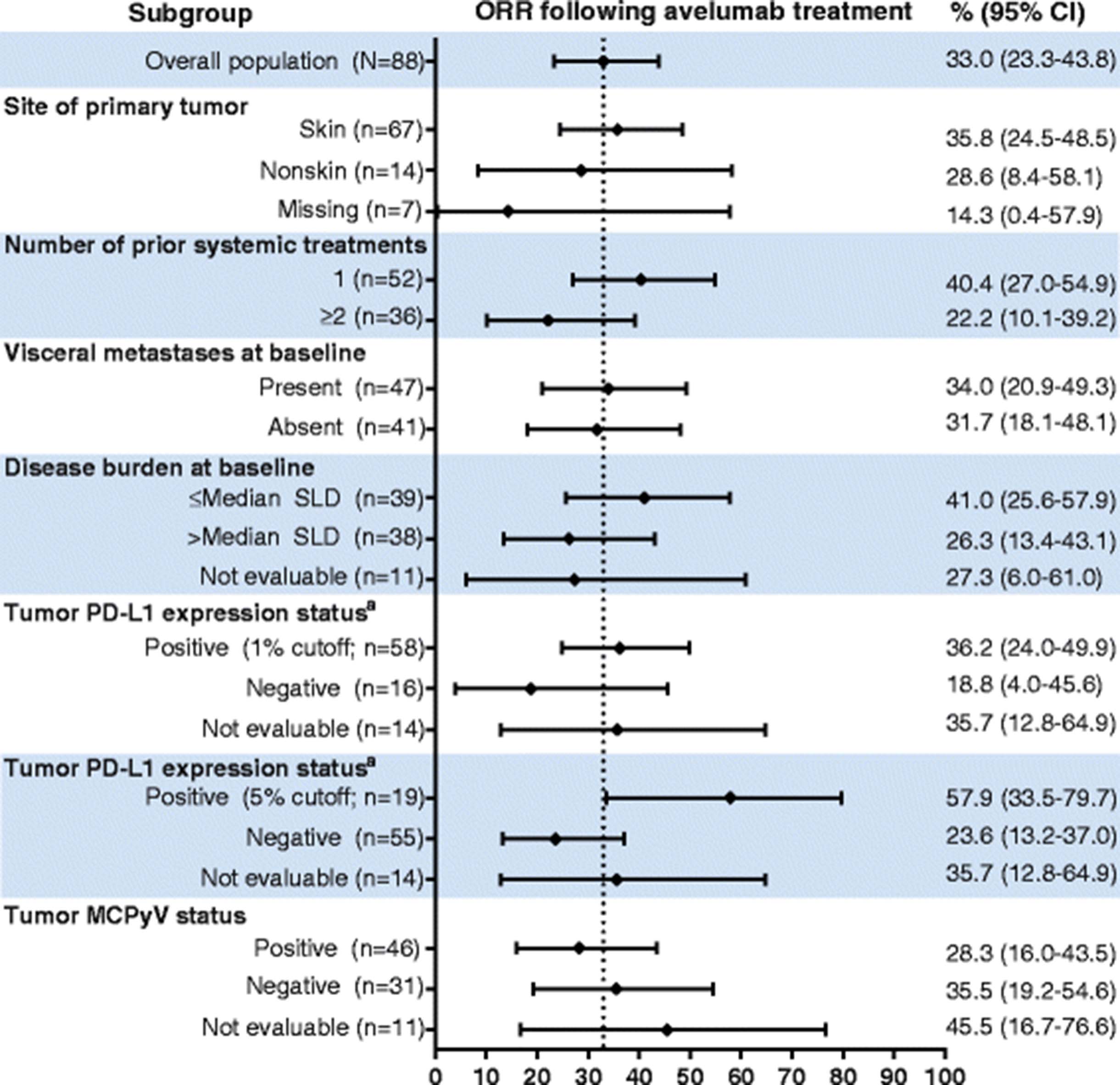
Objective response rates in patient subgroups. The ORR and associated 95% CI values are graphed and shown for the indicated subgroups. MCPyV, Merkel cell polyomavirus; ORR, objective response rate; PD-L1, programmed death-ligand 1; SLD, sum of target lesion diameters. a PD-L1 expression in tumor samples was assessed using a proprietary immunohistochemistry assay (Dako PD-L1 IHC 73-10 pharmDx). Determination of PD-L1–positive status at different PD-L1 cutoff levels was based on tumor cell staining of any intensity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Response durability in patient subgroups. The proportions of responding patients with response duration ≥1 year are depicted for the indicated patient subgroups. The associated median DOR and 95% CI for each subgroup is shown on the right. DOR, duration of response; MCPyV, Merkel cell polyomavirus; NE, not estimable; NR, not yet reached; PD-L1, programmed death-ligand 1; SLD, sum of target lesion diameters. a One patient missing information on site of the primary tumor had an ongoing response for <1 year (8.8+ months). b Of 3 patients with a response to avelumab and PD-L1–negative status (<1% tumor-cell staining cutoff), the response was ongoing in all 3 patients for <1 year (3.9+, 11.1+, and 11.1+ months)
Discussion
These updated data from 88 patients with distant mMCC that progressed following ≥1 line of prior chemotherapy show that avelumab treatment resulted in durable efficacy and prolonged PFS. The confirmed ORR was 33.0%, which is higher than ORRs reported in recent observational studies of second-line or later chemotherapy (9%-23%) [13–15]. Responses were durable, as evidenced by most (72.4%) ongoing at data cutoff and a median DOR not yet reached; the lower bound of the 95% CI (18.0 months) was considerably longer than the median DOR in retrospective studies of chemotherapy (1.7-3.3 months) [13–15]. Furthermore, the estimated proportion of responses lasting ≥1 year with avelumab was 74%, whereas few patients in the historical chemotherapy reference literature had a response lasting 6 months 13-15]. Kaplan-Meier plots of PFS showed that a notable proportion of avelumab-treated patients, primarily those with response, have ongoing clinical benefit. Although median PFS was similar to that with chemotherapy, the Kaplan-Meier–estimated PFS curve for avelumab reached a plateau, which is unprecedented with chemotherapy. Furthermore, the 1-year rate of PFS was 30% in avelumab-treated patients compared with 0% in chemotherapy-treated patients (Fig. 2a). Median OS was 12.9 months, compared with values of <6 months with second-line or later chemotherapy in patients with mMCC [13–15], and the lower bound of the 95% CI for median OS (7.5 months) was longer than that reported in these retrospective studies (Fig. 2b). As for PFS, the Kaplan-Meier estimated OS curve also reached a plateau; approximately 40% of patients exhibited long-term survival. These promising data underscore the challenges to conducting a randomized phase 3 study of immunotherapy compared with chemotherapy in this patient population, given the clear survival benefit of immunotherapy.
We observed objective responses across all subgroups and noted a trend for higher ORRs in patients who received fewer lines of prior therapy, who had lower disease burden, and whose tumors were PD-L1–positive (Fig. 3); these patients might be more likely to be immunocompetent and thus more responsive to immune checkpoint inhibitor treatment [16]. Durable responses were seen across all patient subgroups, irrespective of tumor PD-L1 and MCPyV status (Fig. 4). Taken together, these findings suggest that avelumab may be clinically active in patients with mMCC with different mechanisms of oncogenesis.
JAVELIN Merkel 200 is the largest prospective clinical trial performed in mMCC to date and is continuing enrollment of an additional cohort of patients with mMCC who will receive avelumab as first-line treatment. Findings from this study led to accelerated FDA approval of avelumab for the treatment of patients with mMCC [8, 10], and, for the first time, offer an alternative to chemotherapy.
Conclusions
Avelumab monotherapy has durable antitumor activity in patients with mMCC that progressed after chemotherapy. With a minimum of 1 year of follow-up, the observed prolonged PFS and maturing OS data suggest a potential long-term benefit not previously reported with chemotherapy.
Acknowledgments
The authors thank the patients and their families. The authors also thank the investigators, co-investigators, and study teams at each of the participating centers and at Merck KGaA, Darmstadt, Germany, and EMD Serono, Billerica, MA, USA (a business of Merck KGaA, Darmstadt, Germany).
Authors’ contributions
HLK, JHL, AvH, and PN conceived and designed the study. HLK, OH, SB, JHL, AvH, MH, and PN collected and reviewed the data. All authors analyzed and interpreted the data, participated in writing the manuscript, and approved the final version of the manuscript.
Notes
Ethics approval and consent to participate
All patients were enrolled in accordance with approved protocols, international standards of good clinical practice, institutional review board approvals, and institutional safety monitoring. Written informed consent was provided.
Consent for publication
Not applicable.
Competing interests
HLK reports consultancy for and honoraria from Amgen, Celldex, Compass Therapeutics, EMD Serono, Prometheus, Sanofi, Turnstone Biologics, and Merck KGaA, Darmstadt, Germany; reports research funding from Amgen, EMD Serono, Prometheus, Viralytics, and Merck KGaA, Darmstadt, Germany; and is a member of a speaker’s bureau for Merck KGaA, Darmstadt, Germany. JSR reports consultancy for EMD Serono. OH reports consultancy for Amgen, Novartis, Roche, Bristol-Myers Squibb, and Merck KGaA, Darmstadt, Germany; is a member of a speaker’s bureau for Bristol-Myers Squibb, Genentech, Novartis, and Amgen; and has received research funding from Astra Zeneca, Bristol-Myers Squibb, Celldex, Genentech, Immunocore, Incyte, Merck KGaA, Darmstadt, Germany, Merck Serano, MedImmune, Novartis, Pfizer, Rinat and Roche. SB received research support from EMD Serono. PT has received reimbursement and non-financial support from other commercial sponsors, outside the submitted work. SPD reports employment at Memorial Sloan Kettering Cancer Center and is a member of advisory boards for EMD Serrano, Nektar, and Amgen. CL reports advisory and consultancy for Roche, Bristol-Myers Squibb, Novartis, Amgen, GlaxoSmithKline, and Merck, Sharpe, and Dohme; has received research support from Roche and Bristol-Myers Squibb; is a member of a speaker’s bureau for Bristol-Myers Squibb, Amgen, Roche, and Novartis; has received honoraria from Roche, Bristol-Myers Squibb, Novartis, Amgen, and Merck, Sharpe, and Dohme; and has received travel accommodations from Roche, Bristol-Myers Squibb, and Novartis. KDL has received research support from EMD Serono. JHL has received research support from Novartis, Takeda-Millennium, and Bristol-Myers Squibb; and is a member of an advisory board for Bristol-Myers Squibb and Eisai. AvH reports employment at and is a stock shareholder of Merck KGaA, Darmstadt, Germany. MH reports employment at EMD Serono. PN has received research support from EMD Serono and Bristol-Myers Squibb; and has received personal fees from EMD Serono and Pfizer outside the submitted work. The remaining authors have no conflicts of interest to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
- 2 L
- Second-line
- 2 L +
- Second-line or later
- CI
- Confidence interval
- CR
- Complete response
- DOR
- Duration of response
- DRR
- Durable response rate
- ECOG
- Eastern Cooperative Oncology Group
- FDA
- Food and Drug Administration
- HIV
- Human immunodeficiency virus
- MCPyV
- Merkel cell polyomavirus
- MMCC
- Metastatic Merkel cell carcinoma
- NE
- Not estimable
- NR
- Not yet reached
- ORR
- Objective response rate
- OS
- Overall survival
- PD
- Progressive disease
- PD-1
- Programmed death-1
- PD-L1
- Programmed death-ligand 1
- PFS
- Progression-free survival
- PR
- Partial response
- RECIST
- Response Evaluation Criteria In Solid Tumors
- SLD
- Sum of target lesion diameters
- UV
- Ultraviolet
Footnotes
Funding This trial was sponsored by Merck KGaA, Darmstadt, Germany, and is part of an alliance between Merck KGaA, Darmstadt, Germany, and Pfizer, Inc., New York, NY, USA. Medical writing support was provided by ClinicalThinking, Inc., Hamilton, NJ, USA, and funded by Merck KGaA, Darmstadt, Germany, and Pfizer, Inc., New York, NY, USA.
Availability of data and materials The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request. More information can be found at https://www.merckgroup.com/en/research/our-approach-to-research-and-development/healthcare/clinical-trials/commitment-responsible-data-sharing.html.