Article Text

Abstract
Background The dynamic change in C-reactive protein (CRP) levels, CRP kinetics, is a prognostic factor for metastatic renal cell carcinoma (mRCC) in the tyrosine kinase inhibitor era. We investigated the impact of early CRP kinetics on the efficacy of nivolumab in patients with mRCC.
Methods We performed a retrospective analysis of 42 mRCC patients who were treated with nivolumab as a second-line or later therapy between 2016 and 2019. All patients had received previous TKI therapy. Patients were divided into three groups based on their early CRP kinetics: CRP levels increased to more than double compared with baseline within 1 month after initiation of nivolumab (flare) and then decreased to a lower value than baseline within 3 months (CRP flare-responders); CRP levels decreased by ≥30% within 3 months without “flare” (CRP responders); and the remaining patients (non-CRP responders). The maximum tumor shrinkage, objective response rate (ORR), progression-free survival (PFS), and overall survival (OS) were evaluated. The association of the early CRP kinetics and oncological outcomes was assessed.
Results The median follow-up period was 8 months. The median baseline CRP level was 23 mg/L. CRP flare-responders, CRP responders, and non-CRP responders included 11 (26%), 15 (36%), and 16 (38%) patients, respectively. Thirteen patients (31%) died of mRCC. The maximum changes in target lesions from baseline of CRP flare-responder, CRP-responder, and non-CRP responder groups were −38%, −13%, and 16%, on average, respectively (p<0.001). ORRs of these three groups were 73%, 27%, and 6%, respectively (p<0.001). The median PFS values of each group were not reached, 12 months, and 2.4 months (p=0.005), and the median OS values were not reached, not reached, and 12 months (p=0.048). In a multivariate analysis, early CRP kinetics was a significant independent factor for objective response, PFS, and OS (p<0.001, p=0.004, and p=0.006, respectively).
Conclusions CRP flare-response was associated with significant tumor shrinkage and improved survival outcomes in patients with mRCC who were treated with nivolumab. Early CRP kinetics could be useful for evaluating nivolumab treatment efficacy.
- kidney neoplasms
- immunotherapy
- biomarkers
- tumor
Data availability statement
Data are available upon reasonable request. The data sets used during the study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The management of advanced renal cell carcinoma (RCC) has dramatically changed in recent years with the introduction of immune checkpoint inhibitors (ICIs).1 ICIs are novel treatment options that improved clinical outcomes of patients with metastatic RCC (mRCC).2 3 Nivolumab, a programmed cell death protein-1 (PD-1) antibody, is the first approved ICI agent to treat mRCC, and it showed a survival benefit in the Checkmate 025 trial.2
Because only a subset of patients experience therapeutic benefits with nivolumab, identifying predictive biomarkers has been of great interest. The presence of a systemic inflammatory response has been shown to be associated with a poor prognosis in RCC patients.4 5 C-reactive protein (CRP), an acute-phase reactant, is a representative marker of systemic inflammatory response.5 6 We and other investigators reported that CRP is a potential biomarker for RCC patients treated with surgery, cytokine therapy, and tyrosine kinase inhibitors (TKIs).5 7–9
CRP kinetics, which is defined as the dynamic change in CRP levels, could be a prognostic marker for survival in mRCC patients under multimodal therapy including cytokine therapy.10 Moreover, the early decrease of CRP level after the initiation of TKI therapy was shown to be a predictive factor for tumor response and patient survival.11 However, the impact of CRP kinetics on nivolumab therapy in mRCC patients remains to be fully demonstrated.
In patients with non-small cell lung cancer who received ICIs, CRP was shown to increase at a very early phase after initiation of ICIs.12 Additionally, the early increase in inflammatory cytokines, such as CRP or interleukin (IL)-6, was demonstrated to be predictive for the efficacy of ICIs including nivolumab. There have been no studies assessing the impact of an early CRP increase after initiation of nivolumab therapy in patients with mRCC. This study aimed to explore whether the early CRP kinetics including the presence of early CRP increase after the treatment initiation could predict the efficacy of nivolumab in patients with mRCC.
Methods
We performed a retrospective analysis of 42 mRCC patients who were treated with nivolumab as a second-line or later therapy at our institutions between 2016 and 2019. The requirement for written informed consent was waived because of the retrospective design, and the study protocol was approved by the Ethics Committees at the Tokyo Medical and Dental University (Tokyo, Japan) and the Saitama Cancer Center (Saitama, Japan). Patients were diagnosed and assessed for the extent of the disease based on clinical findings, CT scan, MRI, and/or bone scan. All patients had received previous TKI therapy, and 37 patients (88%) had undergone nephrectomy. Nivolumab (240 mg/body or 3 mg/kg) was administered every 2 weeks until radiographic or clinical disease progression, death, or the occurrence of intolerable adverse events. The intervals of administration could be changed based on the patients’ condition.
The serum CRP level was measured at baseline before initiation of nivolumab, and thereafter at least every 2 weeks when nivolumab was administered as an institutional protocol. Patients were divided into three groups based on their early CRP kinetics, as follows (figure 1): CRP levels had increased to more than double from baseline within 1 month after initiation of nivolumab (flare) and then decreased to a lower value than baseline within 3 months (CRP flare-responders); CRP levels decreased by ≥30% from baseline within 3 months without “flare” (CRP responders), and the remaining patients (non-CRP responders).
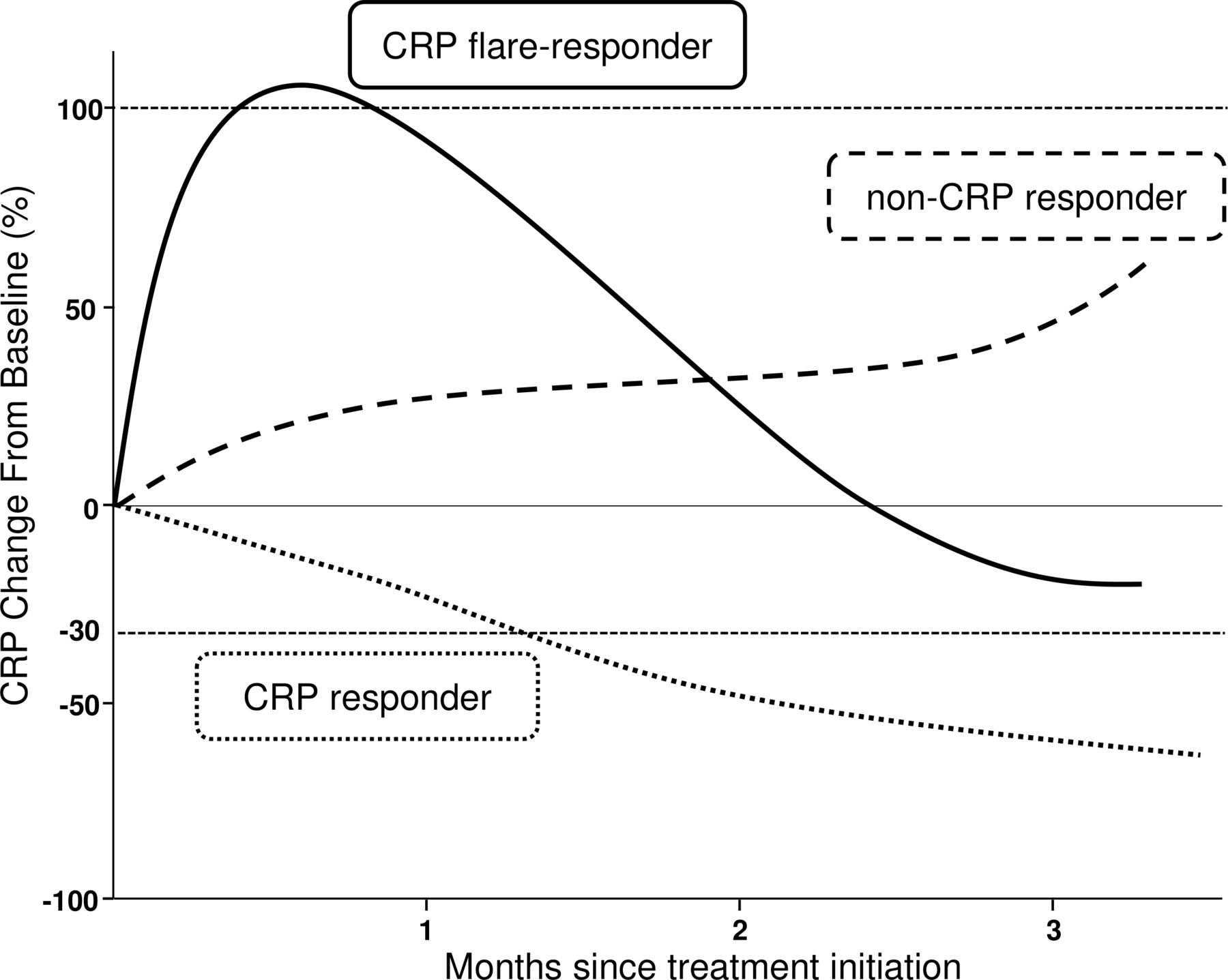
Model of early CRP kinetics showing the three defined groups (CRP flare-responders, CRP responders, and non-CRP responders). CRP, C-reactive protein
Analyzed factors included age, gender, Eastern Cooperative Oncology Group performance status (ECOG PS), and International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) risk13 at the initiation of nivolumab, histology, previous nephrectomy, previous systemic therapies, sites of metastases, baseline lactate dehydrogenase (LDH), baseline neutrophil-to-lymphocyte ratio (NLR), baseline CRP level, and early CRP kinetics status. For statistical analyses, baseline LDH, NLR, and CRP levels were categorized into two groups (elevated vs non-elevated). The increase in baseline LDH was defined as a value of ≥333 IU/L (1.5×upper normal limit at our institutions).14 The threshold value of baseline NLR was set at 3.0 because a previous review in renal oncology demonstrated its predictive ability for survival in mRCC patients.4 As in our previous study, the baseline CRP level was categorized using the threshold value of 10 mg/L.11
CT or MRI was performed before initiation of nivolumab and then repeated approximately every 8–12 weeks at the physician’s discretion. Maximum tumor shrinkage, objective response rate (ORR), and progression-free survival (PFS) were evaluated based on the Response Evaluation Criteria in Solid Tumors (RECIST) V.1.1.15 Overall survival (OS) was also evaluated.
Patient characteristics and oncological outcomes were compared among the three groups using the χ2 test for categorical variables and analysis of variance for numerical variables. Logistic regression analysis was used to identify predictive factors for an objective response. In each group, PFS and OS were estimated using the Kaplan–Meier method and differences between the groups were assessed using the log-rank test. In multivariate analyses for PFS and OS, the Cox proportional hazards regression model was used. PFS was defined as the time from nivolumab initiation to date of progression (radiological or clinical) or death, whichever came first. OS was evaluated as the time from nivolumab initiation to date of death or last follow-up. For all analyses, differences were considered to be significant at p<0.05. All statistical analyses were performed using JMP software V.10 (SAS Institute, Cary, NC, USA).
Results
Patient characteristics
The median follow-up period and number of administration cycles were 8 months (IQR, 3–16 months) and eight cycles (IQR, 4–18), respectively. The baseline characteristics of 42 patients with mRCC are shown in table 1. Patients had a median age of 67 years. Thirty-four patients (81%) were men and eight (19%) were women. Most patients (74%) had ECOG PS scores of 1 or less. IMDC risk criteria showed nine patients (21%) with a favorable risk, 23 patients (55%) with an intermediate risk, and 10 patients (24%) with a poor risk. Most patients (90%) had been diagnosed with clear cell RCC. The remaining four patients (10%) with non-clear cell RCC included chromophobe, type-2 papillary, Xp11.2 translocation, and tubulocystic RCC. While lung metastases were common (79%), seven patients (17%) had liver metastases and four patients (10%) had brain metastases. The median baseline CRP level was 23 (IQR, 2.0–64) mg/L.
Patient characteristics
Early CRP kinetics
The trends of CRP after nivolumab initiation in all patients are shown in figure 2. Overall, CRP flare-responders, CRP responders, and non-CRP responders included 11 (26%), 15 (36%), and 16 (38%) patients, respectively. The patient characteristics of these three groups are summarized in table 1. No significant difference was found among the groups for any variable including IMDC risk, histology, baseline CRP level, and baseline NLR.

The trends of CRP after nivolumab initiation in all patients. Patients were divided into three groups based on their early CRP kinetics (CRP flare-responders (n=11), CRP responders (n=15), and non-CRP responders (n=16)).
Oncological outcomes and early CRP kinetics
During the follow-up period, 13 patients (31%) experienced partial response, 20 patients (48%) had stable disease, and nine patients (21%) had progressive disease. The median PFS for the entire cohort was 8.7 months (95% CI, 3.0–12 months). Thirteen patients (31%) died of mRCC. The median OS for the entire cohort was 25.4 months (95% CI, 12.0 months to not reached).
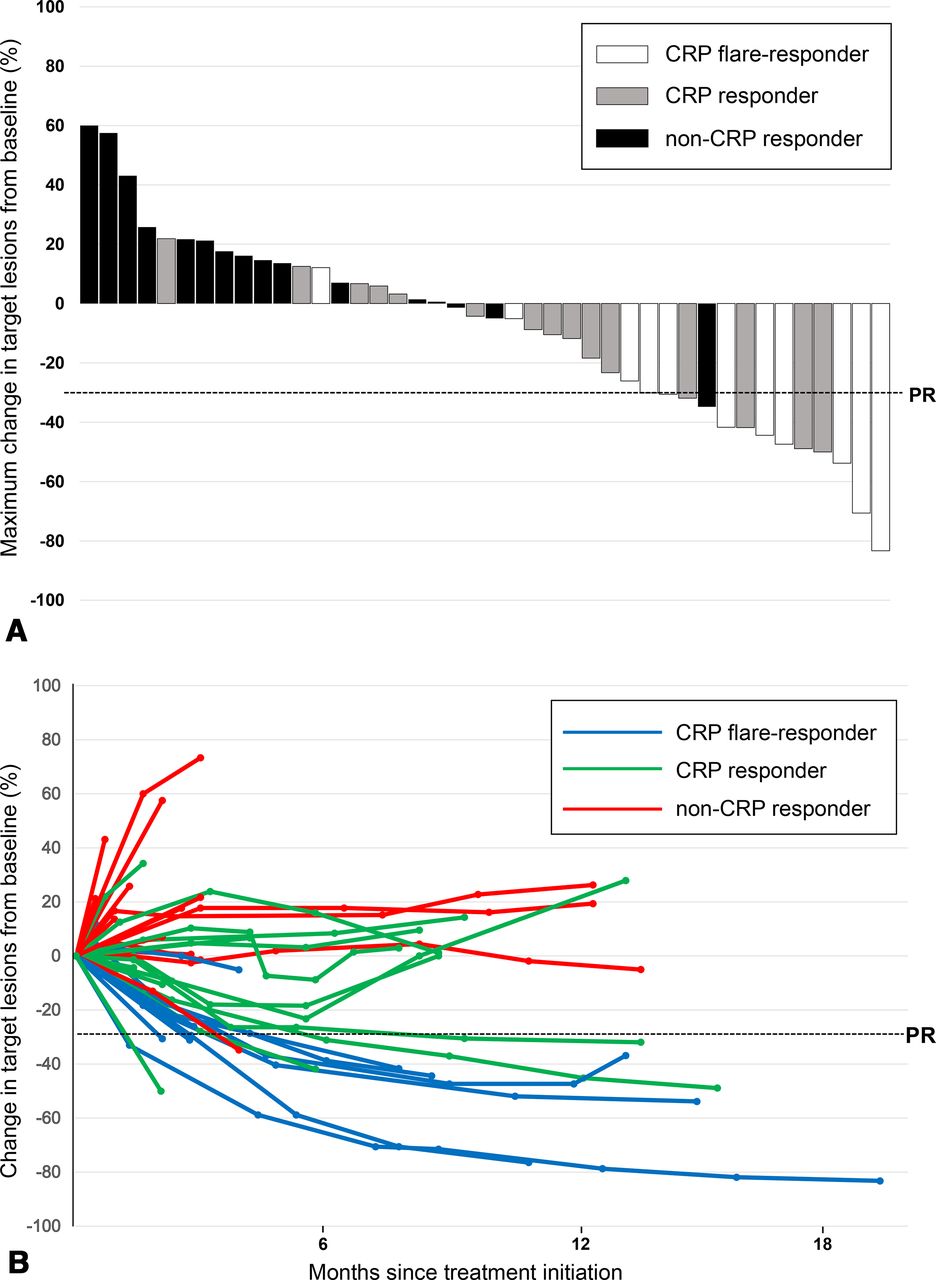
The maximum change in target lesions from baseline of all patients is shown in figure 3A. Those of the CRP flare-responder, CRP-responder, and non-CRP responder groups were −38% (95% CI, −53% to −24%), −13% (95% CI, −26% to −0.7%), and 16% (95% CI, 4.0% to 28%) on average, respectively (p<0.001). The change in target lesions from baseline is shown in figure 3B. In the CRP flare-responder group, six patients experienced significant and sustained tumor shrinkage. CRP flare-response was observed before radiological response in seven out of eight patients who achieved objective response. ORRs of the CRP flare-responder, CRP-responder, and non-CRP responder groups were 73% (95% CI, 43% to 90%), 27% (95% CI, 11% to 52%), and 6.3% (95% CI, 1.1% to 28%), respectively (p<0.001). Logistic regression analysis showed that early CRP kinetics was the only predictive factor for an objective response (p<0.001; table 2).

(A) Maximum change in target lesions from baseline and (B) change in target lesions from baseline based on early CRP kinetics. The dashed line indicates the threshold for a partial response based on the Response Evaluation Criteria in Solid Tumors V.1.1.
Univariate and multivariate analysis for objective response
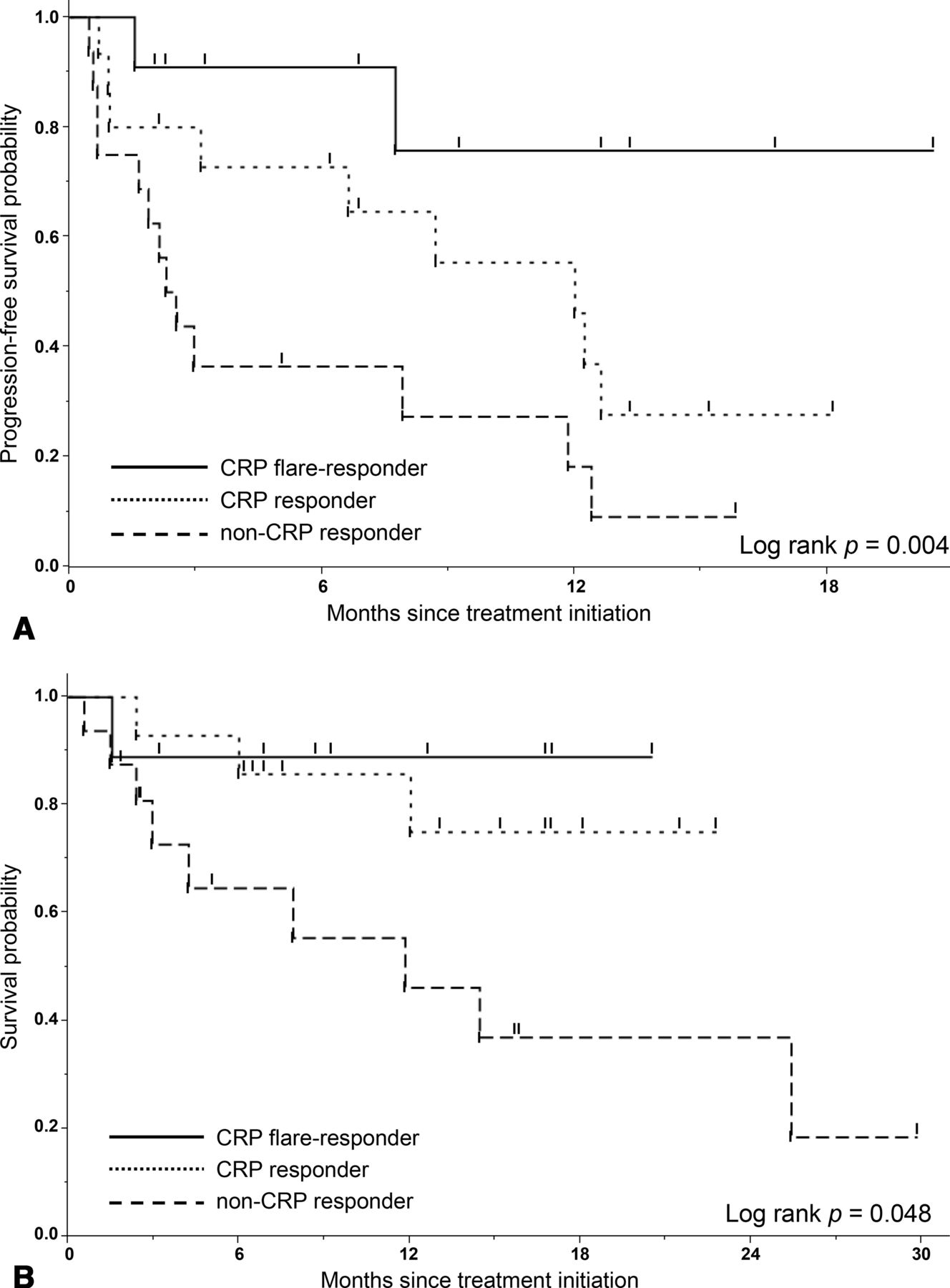
The PFS curves, according to early CRP kinetics, are shown in figure 4A. The median PFSs of the CRP flare-responder, CRP-responder, and non-CRP responder groups were not reached, 12, and 2.4 months, respectively, which showed a significant difference among the three groups (p=0.005). In multivariate analysis using the Cox proportional hazards regression model, early CRP kinetics was the only independent prognostic factor for PFS (p=0.004; table 3). IMDC risk and baseline CRP level were not associated with PFS in our cohort. Furthermore, the OS curves, according to early CRP kinetics, are shown in figure 4B. The median OS values of the CRP flare-responder, CRP-responder, and non-CRP responder groups were not reached, not reached, and 12 months, respectively. They also demonstrated a significant difference among the three groups (p=0.048). In multivariate analysis, early CRP kinetics was shown to be an independent prognostic factor along with baseline LDH for OS (p=0.006).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Progression-free survival curves and (B) overall survival curves based on early CRP kinetics.
Univariate and multivariate analysis for progression-free survival
Subgroup analysis in patients with clear cell RCC
Additionally, we performed a subgroup analysis of 38 patients with clear cell RCC. According to early CRP kinetics, CRP flare-responders, CRP responders, and non-CRP responders included 10 (26%), 14 (37%), and 14 (37%) patients, respectively. No significant differences were observed among the three groups for any baseline characteristics, including IMDC risk and baseline CRP level. During the follow-up period, 13 patients (34%) achieved objective responses. The median PFS and OS for this subgroup was 11.8 months (95% CI, 3.1–12.6 months) and 25.4 months (95% CI, 12.0 months to not reached), respectively. Multivariate analyses demonstrated that early CRP kinetics had a significant prognostic impact on objective response, PFS, and OS (p=0.001, p=0.005, and p=0.007, respectively).
Discussion
In the present study, we showed that early CRP kinetics have a significant impact on the response to nivolumab in mRCC patients. Flare-response of CRP was significantly associated with better tumor response and improved PFS. Most CRP flare-responders (73%) experienced an objective response during the follow-up period.
Research to identify prognostic biomarkers for mRCC patients treated with nivolumab is ongoing, and the predictive role of PD-L1 expression in mRCC patients remains controversial.16 Recently, Pignon et al demonstrated an improved association of tumor cell PD-L1 expression and nivolumab response evaluated with immune-related RECIST (irRECIST) compared with RECIST V.1.1.17 They also showed that a high percentage of CD8 expression in tumor-infiltrating cells was correlated with high levels of T-cell activation and associated with improved oncological outcomes. In addition, serum biomarkers could be useful in the management of ICI treatment.
The presence of a systemic inflammatory response is an indicator of poor outcome in various malignancies including RCC. CRP, a representative systemic inflammatory response, has been shown to be a biomarker for mRCC patients who are treated with systemic therapies including cytokine therapy and TKIs.8 9 18 Recently, elevation of the baseline CRP level was demonstrated to be prognostic for poor OS in mRCC patients treated with nivolumab.19 20 In these studies, the baseline CRP level was not associated with PFS. These findings are consistent with our study, demonstrating that the baseline CRP level was not associated with ORR or PFS although the baseline CRP level could still be a prognostic factor for OS, as shown in previous studies.9 10
Several studies evaluated the prognostic value of other serum biomarkers for the clinical outcomes in mRCC patients treated with ICIs. Zahoor et al demonstrated that the risk of progressive disease was increased with a higher baseline NLR and was reduced with a higher baseline eosinophil count in mRCC patients who received nivolumab.21 Bilen et al reported that pretreatment NLR could be a prognostic biomarker for mRCC patients receiving nivolumab.22 Furthermore, Lalani et al showed that the early decline of NLR and NLR at 6 weeks after the initiation of ICIs was associated with significantly improved outcomes.23 Our findings are consistent with these results regarding the significance of serum biomarkers including systemic inflammatory response in patients treated with ICIs.
Evaluation of early kinetics could add further predictive value of CRP for mRCC patients in the current ICI era. Our previous studies demonstrated that a decrease in CRP levels was an indicator of better survival in the cytokine and TKI era.10 11 While a decrease in CRP levels was also shown to be significantly associated with better ORR in patients with mRCC who were treated with nivolumab,20 the current study further demonstrated that the CRP flare-response had a significant impact on prediction of tumor response and PFS.
The CRP flare could also be significant in other solid tumors that are treated with ICI. Ozawa et al reported that a significant increase in CRP levels within 1 week after starting PD-1/PD-L1 inhibitors was predictive for the therapeutic efficacy in patients with non-small cell lung cancer.12 The authors also demonstrated that none of the patients without either early elevation of CRP or IL-6 showed a response to PD-1/PD-L1 inhibitors. They suggested that the elevation of inflammatory cytokines in the very early phase indicated early immune-system activation.
Clarifying the underlying mechanisms of the association between the systematic inflammatory response and the tumor response to ICIs could lead to an improvement of the treatment outcome. It has been shown that chronic inflammation can generate an immunosuppressive microenvironment.24 We demonstrated that higher CRP levels were associated with an immunosuppressive microenvironment infiltrated with M2 macrophages and regulatory T cells.25 CRP flare-response in nivolumab treatment would be associated with the dynamic change of the cancer-immune system in a tumor microenvironment. In the cancer immunogram that was developed by Blank et al, CRP is one of the clinical markers for tumor-associated inflammation that can promote tumor progression.26 CRP would reflect the cancer-immune status and have a significant role as a cancer-immune marker.
This study had several limitations. First, it had a retrospective design in a small cohort with a limited follow-up duration. The small cohort size could lead to a higher ORR (31%) compared with that of the Checkmate 025 trial.2 Second, this study included patients with clear cell RCC and those with non-clear RCC. Although we confirmed the significance of the CRP flare-response in the clear cell RCC subgroup, the mixture of clear cell and non-clear RCC patients may have affected the clinical outcomes in this study. Third, we categorized mRCC patients into three groups based on their early CRP kinetics. Further analyses are warranted to achieve the optimal definition of the CRP flare-response. To validate our results, additional larger confirmatory studies are needed. Despite these concerns, CRP could be useful to monitor the cancer-immune status so as to improve the treatment efficacy in mRCC patients treated with nivolumab.
Conclusions
This study demonstrated that the CRP flare-response was significantly correlated with better tumor response and improved survival outcomes in patients with mRCC treated with nivolumab. Early CRP kinetics are useful in evaluating the therapeutic effect of nivolumab for mRCC patients and needs prospective, larger validation.
Data availability statement
Data are available upon reasonable request. The data sets used during the study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the institutional review board (M2019-172). The requirement for written informed consent was waived because of the retrospective design.
References
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors SF and KS contributed to the acquisition, analysis, and interpretation of the data and made contributions to the drafting and revising of the manuscript. YY, TK, SY, MY, JI, YM, YK and YF participated in the data acquisition and final revision of the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by JSPS KAKENHI Grant Number 19K09726.
Competing interests YF received research grant from Ono Pharma (Osaka, Japan).
Provenance and peer review Not commissioned; externally peer reviewed.