Article Text

Abstract
Background The predictive power of novel biological markers for treatment response to immune checkpoint inhibitors (ICI) is still not satisfactory for the majority of patients with cancer. One should identify valid predictive markers in the peripheral blood, as this is easily available before and during treatment. The current interim analysis of patients of the ST-ICI cohort therefore focuses on the development and validation of a liquid immune profile-based signature (LIPS) to predict response of patients with metastatic cancer to ICI targeting the programmed cell death protein 1 (PD-1)/programmed cell death-ligand 1 (PD-L1) axis.
Methods A total of 104 patients were prospectively enrolled. 54 immune cell subsets were prospectively analyzed in patients’ peripheral blood by multicolor flow cytometry before treatment with ICI (pre-ICI; n=89), and after the first application of ICI (n=65). Pre-ICI, patients were randomly allocated to a training (n=56) and a validation cohort (n=33). Univariate Cox proportional hazards regression analysis and least absolute shrinkage and selection operator Cox model were used to create a predictive immune signature, which was also checked after the first ICI, to consider the dynamics of changes in the immune status.
Results Whole blood samples were provided by 89 patients pre-ICI and by 65 patients after the first ICI. We identified a LIPS which is based on five immune cell subtypes: CD14high monocytes, CD8+/PD-1+ T cells, plasmacytoid dendritic cells, neutrophils, and CD3+/CD56+/CD16+ natural killer (NK)T cells. The signature achieved a high accuracy (C-index 0.74 vs 0.71) for predicting overall survival (OS) benefit in both the training and the validation cohort. In both cohorts, the low-risk group had significantly longer OS than the high-risk group (HR 0.26, 95% CI 0.12 to 0.56, p=0.00025; HR 0.30, 95% CI 0.10 to 0.91, p=0.024, respectively). Regarding the whole cohort, LIPS also predicted progression-free survival (PFS). The identified LIPS was not affected by clinicopathological features with the exception of brain metastases. NKT cells and neutrophils of the LIPS can be used as dynamic predictive biomarkers for OS and PFS after first administration of the ICI.
Conclusion Our study identified a predictive LIPS for survival of patients with cancer treated with PD-1/PD-L1 ICI, which is based on immune cell subsets in the peripheral whole blood.
Trial registration number NCT03453892.
- biomarkers
- tumor
- immunotherapy
- programmed cell death 1 receptor
- tumor microenvironment
- tumor biomarkers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Immune checkpoint inhibitors (ICI) can effectively restore the activity of exhausted CD8+ cytotoxic T cells and thereby trigger antitumor immune responses. During the last years, several ICI were approved for more than ten different tumor entities. However, still only the minority of patients shows durable responses.1 In clinical trials, the expression of programmed cell death-ligand 1 (PD-L1) on tumor and/or immune cells has been frequently used to select patient subgroups with higher chances of treatment response. However, the predictive power of PD-L1 expression is restricted and its expression varies, as its expression is for example increased after radiotherapy.2–5 Consequently, large effort has been made to identify routinely available blood and clinical markers that may predict the response to ICI therapies,6 besides and complementary to the analyzes of genomic instability.7 The latter has been assessed via tumor mutational burden (TMB)8 or mismatch repair deficiency.9 All of these methods have the potential to predict treatment responses to a certain extent, but are still too complex to be used in the clinical routine. A further challenge is imaging of the cancer treatment response to ICI. Tumor lesions can initially increase in size due to inflammatory events.10 This pseudoprogression cannot be distinguished easily from an increase in size due to tumor growth. Consequently, the classical RECIST V.1.1 criterial were modified to the iRECIST criteria, which recommend treatment beyond the first progression.11 The main problem of this procedure is that patients with real tumor progression loose time for a probably more efficient radiotherapy and/or chemotherapy.
A recent strategy to complement these approaches is to analyze changes of peripheral blood immune cells at early time points during treatment.12 The peripheral blood immune status may have a high predictive power for the treatment response of solid tumors to ICI, as several immune cells that were already proven to predict treatment responses when being present in the tumor tissue also circulate through the peripheral blood.13 Furthermore, peripheral blood can be drawn easily and be repeated without an additional risk for the patients compared with repeated biopsies of the tumor tissue. Immunophenotyping (IPT) of peripheral blood from patients with stage IV melanoma before and after treatment with ICI already identified pharmacodynamic changes in circulating CD8+ T cells with an exhausted-phenotype. Clinical failure of the patients was identified to be associated with an imbalance between T-cell reinvigoration and tumor burden.14 Another study identified a predictive character of proliferating (Ki-67+) PD1+CD8+ T cells for the response to anti-PD-1 immunotherapy in solid tumors.15 Using high-dimensional single-cell mass cytometry, Krieg and colleagues identified monocytes, expressing high levels of HLA-DR to be predictive for the treatment response to anti-PD-1 therapy.16
In the introduced preplanned biomarker analysis of the prospective ST-ICI cohort, the peripheral blood immune phenotype of patients with recurrent and/or metastatic cancer treated with ICI was prospectively monitored by multicolor flow cytometry. Our aim was to construct a predictive immune signature, based on the peripheral blood immunophenotype that identifies patients who benefit from ICI.
Materials and methods
Patients
Patients with recurrent and/or metastatic cancer with clinically indicated treatment with ICI were eligible for this prospective non-interventional study. Patients could be included independent from cancer entity and concomitant radiotherapy. Criteria for eligibility were adult age of at least 18 years and the willingness of the patients to allow regular blood draws for immune phenotyping of peripheral blood. As the trial should represent the predominant clinical situation, there were no limitations regarding baseline Eastern Cooperative Oncology Group performance status or baseline routine blood parameters. Exclusion criteria were fertile patients who refused effective contraception during study treatment, persistent drug and/or alcohol abuse, patients not speaking German, patients in legal care and imprisoned patients.
Study design and treatments
Patients that were treated with ICI directed against programmed cell death protein 1 (PD-1) or PD-L1 were selected from the ST-ICI cohort. All ICI were indicated by the treating physician according to current guidelines and clinical standards. The following ICI were used: Nivolumab (Opdivo, Bristol-Myers Squibb, New York City, NY, USA), Pembrolizumab (Keytruda, Merck Sharp & Dohme, Kenilworth, New Jersey, USA), Atezolizumab (Tecentriq, Roche, Basel, Switzerland), Durvalumab (Imfinzi, AstraZeneca Group, Cambridge, England, UK) or Avelumab (Bavencio, Pfizer and Merck KGaA, Darmstadt, Germany). Dosing of the ICI was according to the European Medicines Agency marketing authorizations.
The research design for the identification of a predictive signature for patients with cancer treated with ICI is displayed in figure 1A. The redaction of the manuscript followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies.

Research design (A) and flowchart (B) for the identification of a predictive signature by immunophenotyping (IPT) for patients with metastatic cancer treated with immune checkpoint inhibitors (ICI). ROC, receiver operating characteristic.
Endpoints and assessments
The primary endpoint of the here presented prospective interim analyzes was the association between changes of the patients’ peripheral blood immunophenotypes and the clinical outcomes. Main clinical outcome parameters were overall survival (OS), and progression-free survival (PFS). OS and PFS were calculated starting with the first administration of the ICI. Peripheral whole blood immune phenotyping was performed before each administration of the ICI. The current analysis focused on the early immune phenotypes, namely before the first administration of the ICI (pre-ICI), and additionally to validate their potential as dynamic biomarker during treatment before the second administration of the ICI.
Multicolor flow cytometry
Whole blood samples of the patients were collected and the fresh whole blood was analyzed by multicolor flow cytometry according to our previously published and optimized IPT protocols.17 18 IPT was performed within 3 hours after the collection of whole blood. Data acquisition was performed on a Gallios Flow Cytometer (Beckman Coulter) in the standard filter configuration. The Kaluza Flow Analysis Software (Beckman Coulter) was used for data analysis. The immune cell subpopulations analyzed are visualized and specified in online supplemental sFigure 1.
Supplemental material
Data collection
Differences in OS and PFS were analyzed in dependence of the absolute immune cell counts of each immune cell subset and in dependence of the clinical factors age, gender, tumor entity, PD-L1 expression (assessed by the tumor proportion score (TPS)), the number of previous treatments and the presence of brain metastases.
Development and validation of liquid immune profile-based signature
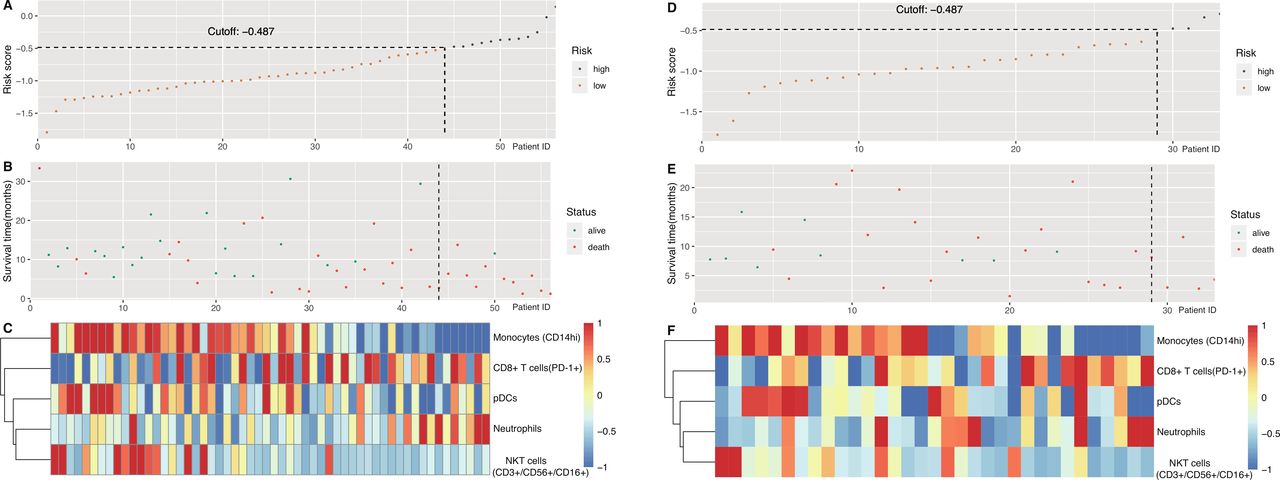
The overall workflow for the development of the liquid immune profile-based signature (LIPS) is shown in figure 1B. Univariate Cox proportional hazard regression was applied to examine the association between peripheral blood immunophenotypes and patients’ OS.19 Peripheral blood immune cells statistically significant associated (p<0.2) with the OS of the patients served as candidates for further analyzes. To uncover the practicability and accuracy of LIPS for patients with metastasized cancer treated with ICI, all patients were divided randomly into the training (n=56) and validation (n=33) cohorts. Least absolute shrinkage and selection operator (LASSO) could reduce the complexity of the model and can be used well with the Cox proportional hazard regression model for survival analysis with high dimensional data.20 21 The Cox-LASSO regression model was applied to develop a multi-immunophenotype-based predictive signature for OS in the training cohort. After 200,000-time steps for LASSO, the best C-index related model was selected as LIPS. Subsequently, we analyzed the data in a validation cohort for this model, to assess its feasibility and reliability in patients treated with ICI. The optimal cut-off value for the risk score (figure 2A,D) was determined by surv_cutpoint function in survminer package. All patients were divided into different groups (high-risk or low-risk) based on the cut-off of the risk score, which was calculated by considering the expression of immunophenotypes and the correlation coefficient. In order to validate the predictive ability of LIPS for PFS, these same coefficients of LIPS were calculated as risk score for survival analysis.
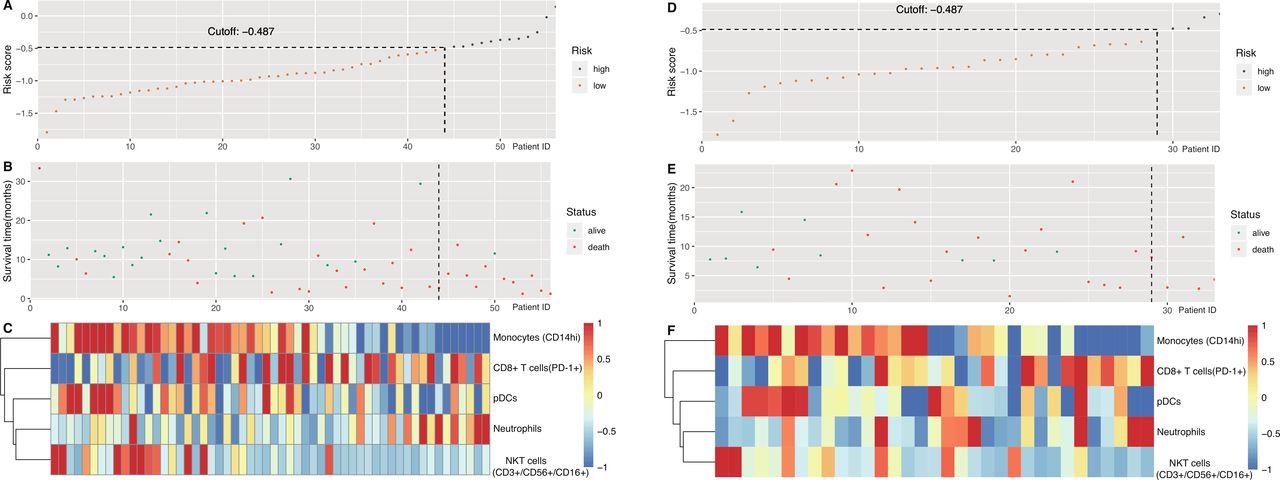
Characteristics of the liquid immune profile-based signature (LIPS) in the training and validation cohorts. (A) The risk score of each patient with metastatic cancer (patient ID) treated with immune checkpoint inhibitors (ICI) in the training cohort. (B) Overall survival and survival status of patients with metastatic cancer in the training cohort. (C) Heat map of immune cell counts of patients with metastatic cancer in the training cohort. (D) The risk score of each patient with metastatic cancer treated with ICI in the validation cohort. (E) Overall survival and survival status of patients with metastatic cancer in the validation cohort. (F) Heat map of immune cell counts of patients with metastatic cancer in the validation cohort. NKT cells, natural killer T cells; pDCs, plasmacytoid dendritic cells; PD-1, programmed cell death protein 1.
Statistical analysis
Associations between clinical characteristics in the training and the validation cohorts, or pre-ICI and after first ICI were evaluated using the χ2 test. OS time was defined from the date of the first administration of the ICI to the date of the last follow-up or death of the patient. PFS time was defined from the date of the first administration of the ICI to the date of the last follow-up or first radiological confirmed progression (eg, imaging date) or date of death (whichever occurs first). The Kaplan-Meier method and Cox proportional hazard regression models were applied to compare survival of the different groups with the immunophenotypes, LIPS and related clinical factors. Univariate, multivariate and subgroup analyzes were used to evaluate the impact of other confounding factors. Results of Cox regression analysis are described by means of HRs, 95% CI of HR and p values (Wald test). The concordance index (C-index) and the time-dependent receiver operating characteristic (ROC) curve, and the area under the ROC curve (AUC) values were calculated for different models as a measure of the discriminatory ability that allows comparison of signatures. A signature with a C-index of 0.5 has no predictive value, but the signature with a C-index of 1 would allow a perfect prediction of the patient’s outcome.22 The C-index was analyzed using the survcomp (V.1.22.0).23 The ROC curve and AUC values were calculated with the timeROC package (V.0.3); for survival analyzes the survival package was used. All of the analyzes were carried out using R V.3.6.1 (R Foundation for Statistical Computing) and related packages. P≤0.05 was considered to be statistically significant.
Results
Patient characteristics
A total of 104 patients were prospectively enrolled in the ST-ICI cohort between April 2017 and August 2019 (figure 1B). Whole blood samples for IPT pre-ICI were available of 89 patients, and for 65 of these 89 patients also after first ICI. The patient characteristics are presented in table 1 and online supplemental sTable 1. The median age was 65.8 years; 73% were men. Most frequent tumor entities were head and neck squamous cell carcinoma (HNSCC) in 40 patients (45%) and non-small cell lung cancer (NSCLC) in 39 patients (44%). The drugs used were Nivolumab in 58 patients (65%), Pembrolizumab in 20 patients (23%), Durvalumab in 8 patients (9%), Avelumab in 2 patients (2%), Atezolizumab in 1 patient (1%).
Supplemental material
Baseline characteristics of patients with metastatic cancer treated with immune checkpoint inhibitors (ICI) and for which immunophenotyping was performed pre-ICI
The ICI was first line treatment in 19 patients (21%). In the recurrent and/or metastatic setting, 13 patients (15%) had received one prior systemic treatment and 57 patients (64%) two or more prior systemic treatments. The median follow-up was 8.3 months. A total of 57 OS-events and 72 PFS-events occurred during the follow-up period. Median OS was 8.7 months, median PFS was 4.2 months.
Development and definition of the LIPS
After the data cleaning steps, 54 peripheral blood immune markers were included into a univariate cox survival analysis. The following 14 of them were associated with OS (p<0.2): monocytes (CD14high), monocytes (CD14low), neutrophils, dendritic cells (DCs), myeloid (m)DCs-1, mDCs-2, plasmacytoid DCs (pDCs), natural killer (NK) cells (CD56high/CD16+), NKT cells (CD3+/CD56+/CD16+), NKT cells (CD3+/CD16+), CD8+ T cells (PD-1+), CD8+ T cells (CD25+), CD8+ T cells (CD69+), and regulatory T cells (Tregs) (table 2).
Univariate Cox regression pre-ICI (p<0.2)
The ST-ICI cohort was then randomly assigned to a training cohort (n=56) and a validation cohort (n=33) for further LASSO proportional hazards Cox regression analysis. After 200,000 times repeat LASSO regression, the highest C-index’s model was chosen as the LIPS. This predictive signature model obtained from the training cohort showed the following risk score=(0.00001219963×the absolute immune cell counts of neutrophils)+(−0.0335468×the absolute immune cell counts of pDCs)+(−0.08766993×the absolute immune cell counts of NKT cells (CD3+/CD56+/CD16+))+(−0.01120408×the absolute immune cell counts of monocytes (CD14high))+(0.004149556×the absolute immune cell counts of CD8+ T cells (PD-1+)). In this signature, neutrophils and CD8+ T cells being positive for PD-1 surface expression were positive coefficients, which means that patients with increasing absolute counts had a shorter OS. However, pDCs, NKT cells (CD3+/CD56+/CD16+) and monocytes (CD14high) were negative coefficients, which means that patients with increasing absolute cell counts had a longer OS.
According to best C-index (0.74, 96% CI 0.67 to 0.82), the optimal cut-off is −0.487, which classified the training cohort into a low-risk group (n=44) and a high-risk group (n=12) (figure 2A–C).
In the training cohort, each unit increase in LIPS was associated with a 0.26-fold increase in OS rates (95% CI 0.12 to 0.56, p=0.00025). The median OS in the LIPS low-risk and high-risk groups was 14.5 (95% CI 10.1-NE (not estimable)) vs 5.4 (95% CI 3.0-NE) months, respectively (figure 3A).
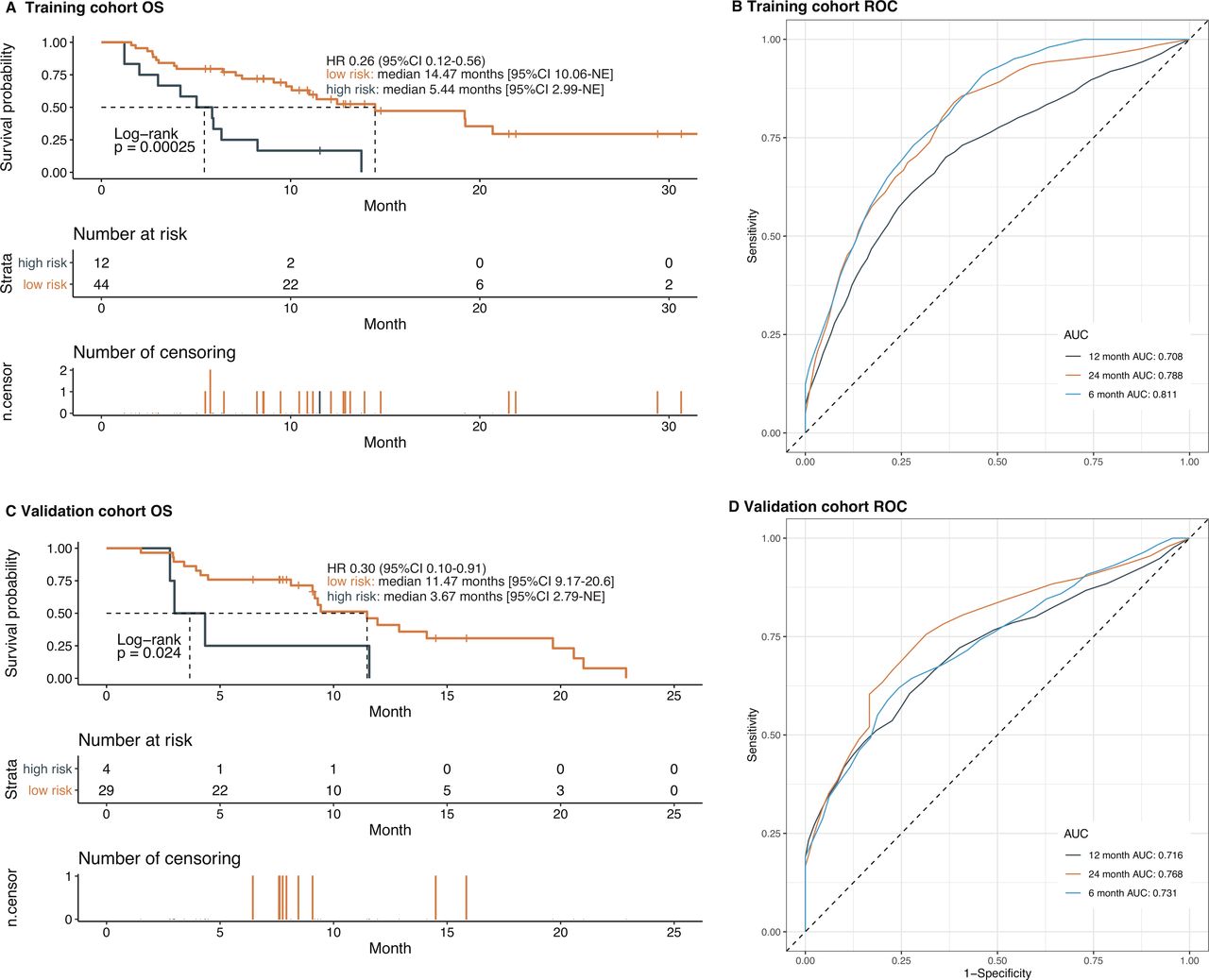
The ability of the liquid immune profile-based signature (LIPS) to predict the overall survival (OS) in the training and validation cohorts. (A) The OS in training cohort stratified by the LIPS into high-risk and low-risk with the p value. (B) Time-dependent receiver operating characteristic (ROC) curves of LIPS in the training cohort. (C) The OS in validation cohort stratified by the LIPS into high-risk and low-risk with the p value. (D) Time-dependent ROC curves of LIPS in the validation cohort. AUC, area under the ROC curve.
The validation cohort was classified using the same cut-off of LIPS into a low-risk group (n=29) and a high-risk group (n=4) (figure 2D–F). The validation cohort confirmed the proposed risk model (C-index=0.71, 95% CI 0.62 to 0.81). The median OS in the low-risk and high-risk groups was 11.5 (95% CI 9.2 to 20.6) versus 3.7 (95% CI 2.8- NE) months (HR=0.30, 95% CI 0.10 to 0.91, p=0.024), respectively (figure 3C).
The sensitivity and specificity of LIPS for predicting the OS were plotted in a time-dependent ROC. In the training cohort, the AUC values for 6-month, 12-month, and 24-month OS prediction were 0.811, 0.708, and 0.788, respectively (figure 3B). In the validation cohort, the AUC values for 6-month, 12-month, and 24-month OS prediction were 0.731, 0.716, and 0.768, respectively (figure 3D).
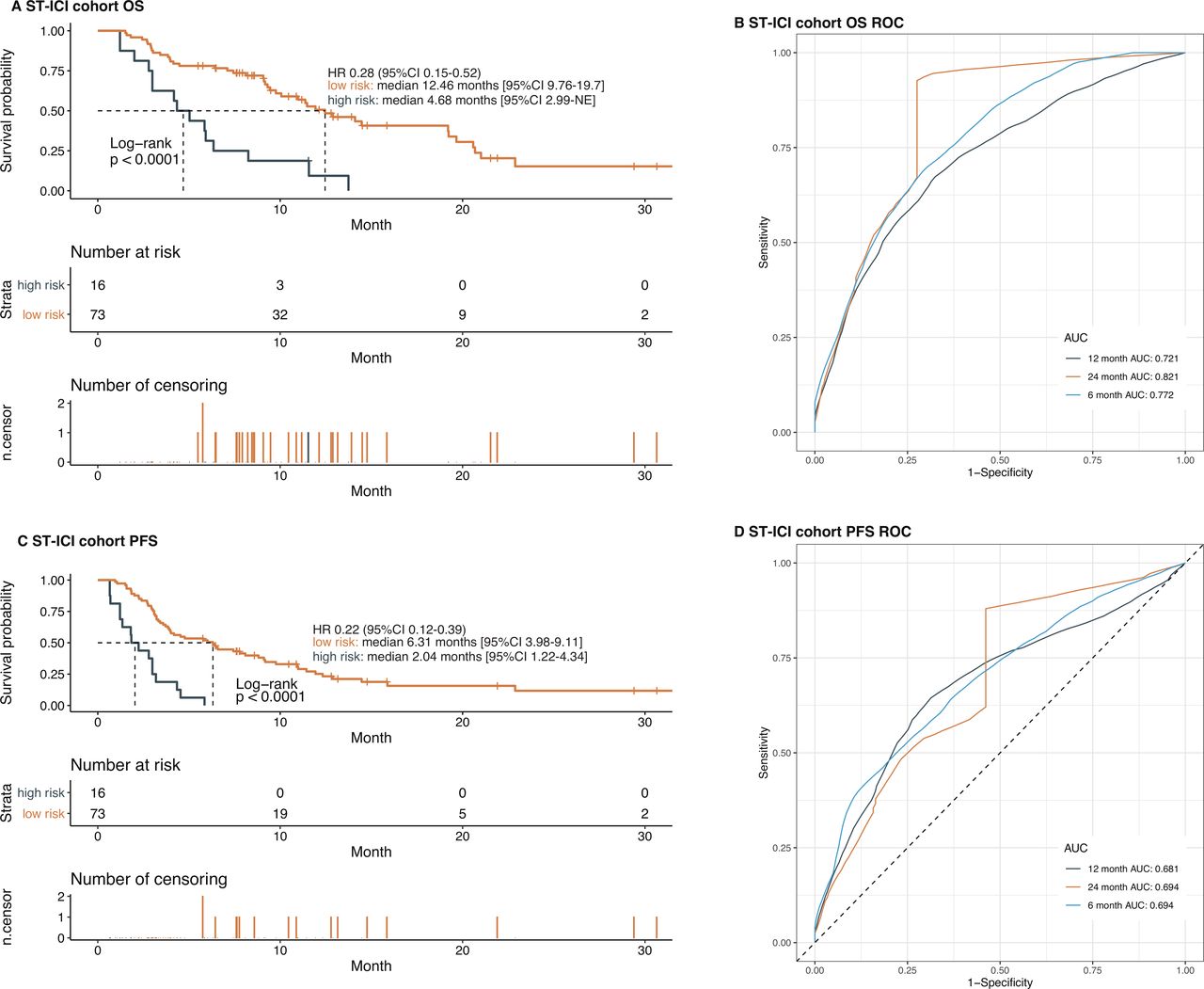
In the total ST-ICI cohort, the median OS in the low-risk and high-risk groups was 12.5 (95% CI 9.8 to 19.7) versus 4.7 (95% CI 3.0-NE) months (HR=0.28, 95% CI 0.15 to 0.52, p<0.001), respectively (figure 4A). The time-ROC results indicate that this signature is still a powerful predictor for OS in the whole cohort (AUC6m=0.77, AUC12m=0.72, AUC24m=0.82) (figure 4B).

Liquid immune profile-based signature (LIPS) predicts survival benefit from immune checkpoint inhibitors (ICI) treatment in all patients with metastatic cancer of the ST-ICI cohort. (A) The overall survival (OS) in all patients stratified by the LIPS into high-risk and low-risk with the p value. (B) Time-dependent receiver operating characteristic (ROC) curves of LIPS for OS in all patients. (C) The progression-free survival (PFS) in all patients stratified by the LIPS into high-risk and low-risk with the p value. (D) Time-dependent ROC curves of LIPS for PFS in all patients. AUC, area under the ROC curve.
Additionally, LIPS also can predict the PFS benefit for patients treated with ICI (low-risk vs high-risk: HR=0.22 (95% CI 0.12 to 0.39); the median PFS of low-risk and high-risk are 6.3 and 2.0 months, respectively (figure 4C); AUC6m=0.69, AUC12m=0.68, AUC24m=0.69 (figure 4D). These results indicate that the developed LIPS can predict which patients with cancer have a prolonged OS and PFS after treatment with anti-PD-1 or anti-PD-L1 in the early phase.
Predictive role of LIPS in patients with metastatic cancer treated with ICI
To determine whether the LIPS could serve as an independent predictive factor, Cox proportional hazard regression model was used for the detection of the relationships between OS and the clinical factors (table 3). In the ST-ICI cohort, univariate analysis showed that LIPS and brain metastases were significantly associated with OS, while multivariate analysis showed that age, PD-L1 TPS >50% and LIPS were significantly associated with OS (p<0.05).
Univariate and multivariate Cox regression analysis for overall survival and progression-free survival
Furthermore, LIPS, number of previous treatments and brain metastases were significantly associated with PFS in the univariate analysis; however, only LIPS was significantly associated with PFS in the multivariate analysis. These results indicate that LIPS remained an independent survival benefit predictor for patients with metastatic cancer treated with ICI.
Applicability of LIPS in patients with cancer with different clinical characteristics
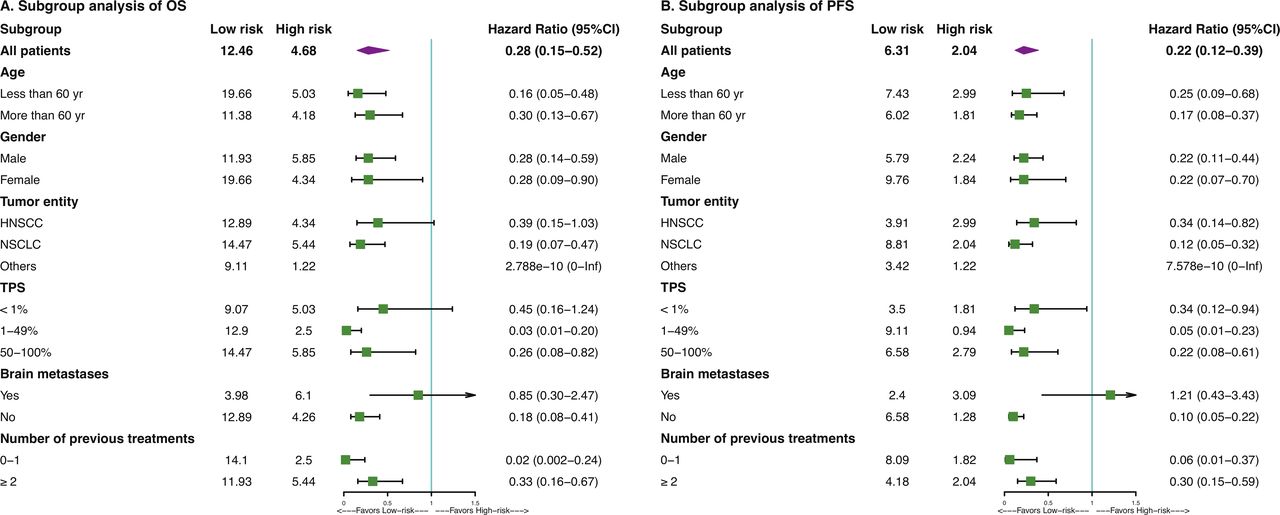
Post-hoc subgroup analyzes based on patient characteristics suggested that OS and PFS HRs favored the LIPS low-risk group in most subgroups (figure 5, online supplemental sFigures 2–7). The LIPS had a predictive value both in PD-L1 TPS low and high cohorts (figure 5A, online supplemental sFigure 3). However, no differences of OS and PFS were found between low-risk and high-risk groups in patients with brain metastases (online supplemental sFigure 4). Median OS and PFS of patients stratified by tumor entity, age, gender, and number of previous treatments are shown in online supplemental sFigures 2, 5–7, respectively.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analysis of the liquid immune profile-based signature (LIPS) predict survival benefit of patients treated with ICI by baseline characteristics. Subgroup analysis of the LIPS predict overall survival (OS) benefit (A) and progression-free survival (PFS) benefit (B) of patients treated with ICI. HR and 95% CIs. HNSCC, head and neck squamous cell carcinoma; ICI, immune checkpoint inhibitors; NSCLC, non-small cell lung cancer; TPS, tumor proportion score.
NKT cells and neutrophils still predict OS and PFS when being analyzed after the first administration of the ICI
The 14 OS-related immune cell subtypes from the pre-ICI time point, based on a Cox regression (p<0.2) (table 2), were also studied in the time point after the first administration of ICI. This analysis revealed that five of them were still significantly (p<0.05) associated with OS (online supplemental sTable 2). The high relevance of considering the dynamics of immune cells in defining predictive signatures is highlighted in online supplemental sFigure 8. While for example, monocytes and PD-1 expressing CD8+ T cells showed a strong decrease in the peripheral blood, NKT cells were relatively stable (mean of the differences for log2(count)=0.21). These NKT cells (CD3+/CD56+/CD16+) (online supplemental sFigure 9) and neutrophils (online supplemental sFigure 10) can still be used as dynamic predictive biomarkers for OS and PFS after first administration of the ICI.
Supplemental material
Supplemental material
Discussion
In recent years, ICI with or without chemotherapy were approved for multiple recurrent or metastatic cancer types. However, only approximately 20% of non-selected patients experience long-term benefit.2 24 Numerous studies suggest that TMB may predict the clinical response to ICI across multiple cancer types.25–27 However, different studies used different cut-off values based on independently companies’ database or cancer types to define low and high TMB.
The detection of PD-L1 by different methods or cut-off values could also guide anti-PD-1/PD-L1 therapy, but still harbors the risk of a false-negative patient stratification.28–30 The gene methylation status may also serve to select patients who will experience a clinical benefit from the PD-1 blockade.31 Nevertheless, there is still particular need of additional or complementary time saving, cost-effective, safe, and easy applicable tools to identify patients with cancer who could benefit from ICI.
In this context, a detailed knowledge about the immune status, both in the tumor and in the periphery, is needed to judge about the potential of cancer immunotherapy and the efficacies of immunotherapies.32 Tumor immunogenicity scores are under evaluation as predictors for responses to ICI.33 Previous studies already indicated peripheral blood immune cell subsets like PD-1+CD56+ T cells34 or CD4+ and CD8+ cells35 to be associated with favorable outcome for advanced melanoma patients treated with ipilimumab directed against cytotoxic T lymphocyte antigen-4 (CTLA-4). Now we identified a liquid immune profile-based signature to predict response of patients with metastatic cancer to anti-PD-1/PD-L1 treatment at an early time point.
To our best knowledge, the prospective ST-ICI cohort is the first one, which prospectively included a whole-blood multicolor flow cytometry-based approach for the identification of a detailed peripheral immune status in a clinical relevant multitype advanced cancer patient cohort treated with anti-PD-1/PD-L1 ICI. For these patients the treatment response according to RECIST V.1.1 is less appropriate for defining a prognostic signature. The main cohorts in ST-ICI are NSCLC and HNSCC. Pseudo-progression is a rare, but a frequently appearing phenomenon in PD-1 inhibitor therapy. These patients are rated as “progressive disease” according to RECIST V.1.1, even though they are probably the best responders later on. In NSCLC patients continuing immunotherapy beyond progression had significantly prolonged OS.36 The newly developed iRECIST criteria might be a method to cope with this problem, but have not been established in prospective clinical trials so far. Also, in HNSCC a secondary analysis of the CheckMate-141 trial identified responses after initial progression.37 A total of 24% of patients developed a reduction of the RECIST sum of diameters after initial progression. This highlights also in HNSCC that patients benefit from ICI even if tumor progression is identified in the first imaging assessment. Growing evidence indicates that there is a large number of patients that benefit from ICI also without developing an objective response according to RECIST V.1.1. Consequently, we decided to use the more valid endpoint OS for the development of our prognostic signature.
To avoid large volume blood sampling for preparation of peripheral blood mononuclear cells and to include granulocytes in the analyzes, the IPT was performed in fresh whole blood without preceding isolation of specific cells. Thus, whole blood assays gain importance as they are an easy approach to screen a large number of blood parameters. Within the ST-ICI cohort, 54 immune cell subsets were monitored in the patients with the need of less than 1 mL of peripheral whole blood. Our identified LIPS has the advantage of being easily integrated into clinical use for nominal expense. In a first step, 14 immune cell subsets were identified to be associated with OS. Furthermore, LASSO regression constructed the LIPS signature including neutrophils, pDCs, NKT cells (CD3+/CD56+/CD16+), monocytes (CD14high), and CD8+ T cells (PD-1+). This signature includes innate and adaptive immune cells and serves as an effective tool for the identification of patients with metastatic cancer who benefit from ICI treatment. It is becoming more and more evident that multiple immune cell subsets in a concerted action may help for selecting patients that are likely to respond to ICI.38
We identified that increasing amounts of neutrophils in the peripheral blood of patients with cancer were associated with less benefit from ICI treatment. Neutrophils have been reported to support for example the development of metastasis through multiple mechanisms, such as the release of proteases that degrade antitumor factors, and leukotrienes that propagate metastasis-initiating cells. In addition, pro-tumorigenic neutrophils suppress antitumor T cell responses.39 Decreased migration of neutrophils to tumor areas or the inhibition of granulocyte colony stimulating factor to decrease the amount of neutrophils has already shown efficacy in preclinical models.40 Recent findings suggest that neutrophil antagonism will improve the efficacy of ICI therapy in the future.12
Regarding innate immune cells not of the granulocytic, but of the monocytic compartment, increased amounts of CD14 high expressing monocytes in the peripheral blood are associated with improved prognosis. This is in accordance with the findings of Krieg et al who identified CD14+/HLA-DR+ monocytes as a strong predictor of PFS and OS in response to anti-PD-1 immunotherapy in melanoma patients16. We here show the importance of CD14 high expressing monocytes in the peripheral blood for non-melanoma solid tumor patients.
Further, we found that increased amounts of plasmacytoid dendritic cells (pDCs) are beneficial for the PFS and OS. pDCs have a central role in activating host innate and adaptive immune responses and they are known as the major interferon type I-producing cells. Thereby, pDCs activate many other cell types, such as monocytes, NK cells, and T cells which are known to be also crucial for antitumor immune responses.41 High levels of circulating pDCs were already found to be predict a favorable outcome in patients with breast cancer42 and for patients with pancreatic adenocarcinoma.43
NKT cells are suggested to induce a cross talk of pDCs with conventional DCs that result in induction of memory CD8+ T cells.44 We identified increased numbers of NKT cells in patients of the ST-ICI cohort to be favorable for PFS and OS. Just recently, it was shown for patients with NSCLC that increased amounts of peripheral NK cells correlate with responses to anti-PD-1 treatment.45 The role for NKT cells in this scenario has not been investigated before, but it is becoming more and more evident that NKT cells are important in antitumor immunity as they, for example, reinvigorate exhausted immune cells in the tumor microenvironment.46
Exhausted immune cells fail to contribute to antitumor immunity. Increased numbers of PD-L1+ NK cells in the peripheral blood, for example, are associated with poor response to anti-PD-1 treatment of patients with NSCLC.47 However, intratumoral CD8+ T cells which are positive for PD-1+ were shown to be predictive for response and survival on anti-PD-1 antibody therapy, as shown in a small cohort of patients with NSCLC.48 Studies in chronic myeloid leukemia patients just recently revealed that differences in PD-1. Expression on CD8+ T-cells might predict the disease course.49 Our immune monitoring suggests that increased amounts of circulating PD-1+ CD8+ T cells at early time points of ICI therapy predict a poorer OS and PFS in patients with metastatic solid tumors treated with ICI. This might indicate that in these cases the activated CD8+ T cells cannot enter properly into the tumor and exert their antitumor activity.
The ST-ICI cohort composes a clinically highly relevant group of advanced stage patients with solid tumors, that includes some confounding factors such as the treatment with different ICI, different tumor types, brain metastases, the number of previous treatments and PD-L1 expression. La and colleagues identified a median OS of NSCLC patients of 9.9 months in the second line ICI treatment, and a median OS of HNSCC patients of 7.4 months in real-world cohorts.50 This is in line with our findings with a median OS of 8.7 months in a cohort consisting mainly of NSCLC and HNSCC. In the ST-ICI cohort, 32 patients had 0–1 previous treatments, while 57 patients had ≥2 of previous treatments. Patients with less (0–1) of previous treatments did not show significantly prolonged OS (HR=0.60 (0.34–1.08), median OS(0–1)=12.46 (9.76-NE) months, median OS(≥2)=9.44 (7.43–14.5) months), but a prolonged PFS (HR=0.49 (0.30–0.82), median PFS(0–1)=7.79 (4.01–15.88) months, median PFS(≥2)=3.22 (2.93–5.79) months). Furthermore, number of previous treatments (0–1 vs ≥2) was significantly associated with PFS in the univariate analysis, however, it was not significantly associated with PFS in the multivariate analysis. The number of previous treatments was also not significantly associated with OS in the univariate and multivariate analysis. Taken together, this factor did not impact our LIPS signature as predictor for ICI. The multivariable Cox regression and subgroup analyzes suggest that LIPS is an independent predictive factor for patients with advanced cancer treated with ICI targeting the PD-1/PD-L1 axis. The subgroup analyzes suggest that this immune signature can reliably predict OS and PFS benefit for patients with cancer treated with ICI in any subgroups, except for brain metastases. This may be a consequence of a continuous administration of glucocorticoids in these patients. Although patients with brain metastases can benefit from ICI treatment,51 the knowledge about the immune microenvironment at this tumor location side is scarce,52 53 and future trials will have to particularly focus on this subgroup of the ST-ICI study population. In present clinical practices, PD-L1 expression is an essential biomarker as drug approvals mostly depend on its expression. However, our subgroup analyzes revealed that the LIPS predicts survival benefits independent from PD-L1 expression. Notably, LIPS identified more than 82% of all patients with advanced cancer, who benefit from anti-PD-1/PD-L1 antibodies.
It has been recognized that a non-invasive and early detection of multiple parameters including peripheral immune features are promising to predict the clinical response of patients with cancer to ICI. At the same time, the dynamics of the responses should be considered.54 As the NKT cells and neutrophils as central part of our identified LIPS can still predict OS and PFS even after the first administration of the ICI (online supplemental sFigures 9–10), our analyzes and results demonstrate that easy applicable immune phenotyping of peripheral blood of patients with metastasized cancer allows an accurate and early forecasting of OS and PFS in patients with metastatic cancer.
Supplemental material
Supplemental material
Conclusion
Our prospective analyzes of the immune status of patients of the ST-ICI cohort demonstrated that LIPS can predict which patients with cancer with advanced disease will benefit from ICI treatment and therefore could guide clinical decisions in the future. This newly identified LIPS is a low-cost, safe, easy and broadly applicable and effective early predictor for OS and PFS in patients with recurrent and/or metastatic cancer treated with ICI.
Acknowledgments
The authors thank the patients who participated in the study, their supporters, the investigators, and clinical research staff from the Department of Radiation Oncology. The present work was performed by J-GZ in (partial) fulfillment of the requirements for containing the degree “Dr. rer. biol. hum.”. We further acknowledge the support by the German Research Foundation and the Friedrich-Alexander-Universität Erlangen-Nürnberg within the funding program Open Access Publishing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JianGuoZhou3, @BetterCallBenni, @Markuseckstein3, @rgrsun, @GaiplS
J-GZ and A-JD contributed equally.
UG and MH contributed equally.
Contributors Conception and design: MH, UG, BF, RF, HM, J-GZ, ME, A-JD. Development of methodology: J-GZ, A-JD. Acquisition of data: A-JD, SR, IB, BF, ME, MH, UG. Analysis and interpretation of data: J-GZ, AD, ED, RS, PS, UG, MH. Writing, review, and/or revision of the manuscript: J-GZ, A-JD, RF, MH, UG, ED, RS, CS, PS. Administrative, technical, or material support: SR, CS, HM. Study supervision: UG, MH, RF, BF.
Funding The study was supported by the Department of Radiation Oncology, Universitätsklinikum Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen, Germany and it was partly supported by the BMBF (GREWIS-alpha, 02NUK050E), and the NSFC (Grant No. 82060475).
Competing interests MH reports conflict of interest with Merck Serono (advisory boards, honoraria for lectures, travel grants, research funding); MSD (advisory boards, travel grants, research funding); AstraZeneca (research funding); Novartis (research funding); BMS (advisory boards, honoraria for lectures); Teva (travel grants). USG received support for presentation activities for Dr Sennewald Medizintechnik GmbH, has received support for investigator initiated clinical studies (IITs) from MSD and AstraZeneca and contributed at Advisory Boards Meetings of AstraZeneca and Bristol-Myers Squibb. JGZ received support from AstraZeneca (travel grants). HM reports conflict of interest with Merck Serono (advisory boards, honoraria for lectures, travel grants); MSD (advisory boards, honoraria for lectures, travel grants); AstraZeneca (advisory boards, honoraria for lectures, travel grants); BMS (advisory boards, honoraria for lectures, travel grants). RS received travel and accommodation expenses from AstraZeneca. ED reports grants and honoraria from ROCHE GENENTECH, grants from SERVIER, grants and honoraria from ASTRAZENECA, MERCK SERONO, BMS and MSD, outside the submitted work. SR conflict of interest with AstraZeneca (research funding); MSD (research funding). ME conflict of interest with Diaceutics (employment, honoraria, advisory role, speakers’ bureau, travel expenses); AstraZeneca (honoraria, advisory role, speakers’ bureau, travel expenses); Roche (honoraria, travel expenses); MSD (honoraria, speakers’ bureau); GenomicHealth (honoraria, advisory role, speakers bureau, travel expenses); Astellas (honoraria, speakers’ bureau); Janssen-Cilag (honoraria, advisory role, research funding, travel expenses); Stratifyer (research funding, patents). RF conflict of interest with MSD (honoraria, advisory role, research funding, travel expenses); Fresenius (honoraria); BrainLab (honoraria); AstraZeneca (honoraria, advisory role, research funding, travel expenses); Merck Serono (advisory role, research funding, travel expenses); Novocure (advisory role, speakers’ bureau, research funding); Sennewald (speakers’ bureau, travel expenses).
Patient consent for publication Not required.
Ethics approval The institutional review board at the Friedrich-Alexander-Universität Erlangen-Nürnberg approved the study (number: 2_17 B). The study was performed in accordance with the Declaration of Helsinki. All patients gave written informed consent before enrollment that comprised a data privacy clause for data collection and analysis for research purpose.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.