Article Text

Abstract
Immune checkpoint inhibitors targeting cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) and programmed death-1 (PD-1)/ligand are increasingly used to treat several types of cancer. These drugs enhance antitumour T-cell activity and therefore induce immune-related adverse effects (irAE), of which gastrointestinal (GI) irAE are among the most frequent and severe. This systematic literature review summarises the clinical manifestations, management and pathophysiology of GI irAE due to immune checkpoint inhibitors. GI irAE induced by anti-CTLA-4 are frequent, potentially severe and resemble IBD, whereas those induced by PD-1 blockade seem to be less frequent and clinically more diverse. Baseline symbiotic gut microbiota is associated with an enhanced antitumour response to immune checkpoint inhibitors and an increased susceptibility to developing enterocolitis, in patients treated with anti-CTLA-4. These findings open new perspectives for possible manipulation of the gut microbiota in order to better identify responders to immune checkpoint inhibitors and to increase their efficacy and safety.
- inflammatory bowel disease
- immunotherapy
- colonic microflora
Statistics from Altmetric.com
Introduction
Immune checkpoint inhibitors (ICI) targeting cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) and programmed death-1/ligand (PD-1/PD-L1) have become a new standard of care in several cancers. Ipilimumab, an anti-CTLA-4 antibody, has been approved in melanoma by European Medicines Agency as well as Food and Drug Administration. Anti-PD-1 (nivolumab, pembrolizumab) and anti-PD-L1 (atezolizumab, avelumab and durvalumab) antibodies have been approved by European Medicines Agency and/or Food and Drug Administration in melanoma, non-small cell lung carcinoma (NSCLC), hepatocellular carcinoma, gastric or gastro-oesophageal junction PD-L1+ adenocarcinoma, classic Hodgkin’s disease, squamous cell carcinoma of the head and neck, urothelial carcinoma, Merkel cell carcinoma and solid tumours with high microsatellite instability.1–6 In contrast to the direct cytotoxic action of traditional antineoplastic agents, ICI enhance antitumour T-cell activity. This leads to a systemic loss of tolerance, with resulting immune-related adverse effects (irAE), of which gastrointestinal (GI) irAE are among the most frequent and severe.7
We performed a systematic literature review to summarise the clinical manifestations, management and pathophysiology of GI irAE due to ICI. We specifically focus on the role of microbiota in ipilimumab-induced enterocolitis and antitumour response to ICI, and outline the similarities and differences with IBD.
Methods
Eligibility criteria and literature search
A systematic literature search of PubMed was performed using a predetermined protocol in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis checklist. The medical subject heading (MeSH) terms ‘colitis’, ‘inflammatory bowel disease’ and ‘gastrointestinal toxicity’ with the subheading terms ‘ipilimumab’, ‘tremelimumab’, ‘anti-CTLA-4’, ‘immune checkpoint inhibitors’ ‘nivolumab’, ‘anti-PD-1’, ‘pembrolizumab’, ‘atezolizumab’, ‘avelumab’ and ‘durvalumab’ were used for the search in the PubMed/Medline from their inception to March 2018. Furthermore, references of relevant articles were checked. Searches were limited to articles in English.
Selection criteria
Studies reporting the prevalence, manifestations, management and pathophysiology of GI irAE due to ICI were included. Two study authors (ES and FC) independently conducted an initial screen of abstracts for eligibility and evaluated the full-text articles of identified abstracts for final eligibility. Disagreements in full-text eligibility were resolved by consensus.
Data extraction
The two reviewers independently extracted data from all selected studies. Data extracted included: author, journal, year of publication, title, data source, country, number of patients with GI irAE, manifestations, diagnosis, management and pathophysiology.
Results
A total of 912 citations were identified through PubMed, of which 611 citations were excluded on title or abstract because they were irrelevant, duplicates or non-English. Therefore, 301 citations were assessed for full-text eligibility (see online supplementary file 1 material). Among these, 96 papers were included in the systematic literature review. Thirty-nine additional papers were included in this review, mostly in the section dedicated to the role of gut microbiota.
Supplementary file 1
Incidence and risk factors for enterocolitis due to ICI
Three recent systematic literature reviews and meta-analyses of published studies (including controlled trials) have assessed the risks of diarrhoea and colitis in patients treated with anti-PD-1 and/or anti-CTLA-4.7–9 The incidence of diarrhoea was 12.1%–13.7% for anti-PD-1 and 30.2%–35.4% for anti-CTLA-4. The incidence of colitis was 0.7%–1.6% for anti-PD-1, 5.7%–9.1% for anti-CTLA-4% and 13.6% for the combination of both therapies. Risk factors of enterocolitis due to immune checkpoint inhibitors are shown in table 1.
Risk factors of enterocolitis due to immune checkpoint inhibitors
Age is not a predictor of ICI, as demonstrated in a recent study of 254 patients treated with anti-PD-1 for metastatic melanoma in which incidence of immune-related enterocolitis did not differ across age groups.10
The incidence of diarrhoea and colitis due to ipilimumab increases with the dose administered. In a recent randomised trial, the incidences of grade 3–4 diarrhoea and colitis were 10% and 5%, respectively, among those treated with 10 mg/kg of ipilimumab as compared with 6% and 2%, respectively, among those treated with 3 mg/kg.11
Pre-existing autoimmune or inflammatory disorders are frequent exclusion criteria in trials evaluating ICI. Thus, few data are available on the risk of immune-related colitis in patients with pre-existing Crohn’s disease (CD) and UC.12–15 Two retrospective studies have reported a total of nine patients with CD or UC who received ipilimumab.12 13 These patients with IBD were asymptomatic or minimally symptomatic at the time of ipilimumab initiation, yet three out of nine patients had an exacerbation of their IBD after initiating ipilimumab. One was a patient with CD who developed worsening colitis that resolved with methylprednisolone. A second was a patient with UC and prior colectomy who developed diarrhoea and responded to treatment with infliximab.12 A third was a patient with UC who developed grade 3 colitis after two doses of ipilimumab and required treatment cessation and systemic steroids.13 An additional case report described a patient with UC and metastatic melanoma treated with ipilimumab who had a severe exacerbation of his colitis with perforation requiring total colectomy, but subsequently had complete response of his melanoma to ipilimumab.16 Taken together, these data suggest that the risk of flare is approximately 30% in patients with IBD treated with anti-CTLA-4 therapy and that these flares may be severe. In contrast to treatment with anti-CTLA-4, in a series of five patients with quiescent IBD (three CD and two UC with prior colectomy) treated with anti-PD-1 therapy, no flares of their underlying IBD were seen.15 Among patients with non-IBD autoimmune or inflammatory disorders who were treated with anti-PD-1 therapy, flares of autoimmune or inflammatory disorders occurred more often in patients with baseline active inflammatory disease (9/15, 60%) than in those with clinically inactive disease (11/37; 30%; p=0.039).15 Patients with pre-existing autoimmune or inflammatory disorders had the same response rate to immunotherapy as patients without these conditions. However, patients on treatment with immunosuppressives at the time of treatment initiation had a lower response rate to anti-PD-1 antibodies.
Cancer type appears to be a risk factor for some irAE. GI irAE seem to be more frequent in patients treated with anti-PD-1 antibodies for melanoma as compared with those treated for NSCLC and renal cell cancer.7 8 This link between cancer types and selected irAE has already been reported for vitiligo, which is commonly observed in patients treated with ICI for advanced melanoma but is not common among patients treated for other cancers. In this particular case, the association suggests that vitiligo is due to an immune reaction towards antigens that are shared between melanoma cells and normal melanocytes. The pathophysiology underlying why GI irAE differ by specific cancer types is unclear.
Various biomarkers have been studied to assess their predictive value for the development of anti-CTLA-4-induced enterocolitis. Baseline levels of microbial antibodies were variably elevated in patients who later developed GI irAE, with 21.4% of patients with perinuclear anti-neutrophil cytoplasmis antibodies (p-ANCA) and 40.5% of patients with anti-OmpC antibodies later developing grade 2 or higher GI irAE. In contrast, there was little association with Anti-Saccharomyces Cerevisiae Antibody, anti-CBir1 or anti-I2 antibodies.17 Higher baseline serum interleukin (IL)-17 levels have also been shown to correlate significantly with the incidence of grade 3 diarrhoea and colitis (p=0.02).18 In addition, increasing eosinophil blood count during treatment with ipilimumab was associated with increasing rate of irAE.19 In contrast, faecal calprotectin, a biomarker of bowel inflammation frequently used in monitoring for the development of active inflammation in IBD,20 was not predictive of GI irAE after ipilimumab treatment.17 21
Anti-CTLA-4-induced enterocolitis
Numerous case reports22 23 and case series24–29 have described enterocolitis due to anti-CTLA-4. Enterocolitis may develop after 1 to 10 doses of ipilimumab, with a median onset time of approximately 1 month after the first infusion.24 25 29–31 The median time between the last ipilimumab infusion and diarrhoea onset is 11–14 days (range 0–59 days).29 30 Unlike other irAE which have been described with a delay of up to 2 years after the discontinuation of ipilimumab, a gap of 2 months seems the maximal delay observed between treatment discontinuation and onset of enterocolitis.32
Clinical presentation
The hallmark symptom of ICI enterocolitis is diarrhoea. Many patients also experience abdominal pain, nausea and vomiting, while haematochezia and fever are less frequent.23 25 The grading of severity of GI events is reported in table 2. Patients with colitis due to anti-CTLA-4 may also have other irAE such as hypophysitis, hepatitis, nephritis, pericarditis, uveitis or aseptic meningitis. However, the frequency of non-GI irAE is not different in patients with and without enterocolitis.29 In a series of 39 patients with anti-CTLA-4 enterocolitis, 4 patients had symptoms reminiscent of CD: 1 patient had aphthous mouth ulcers and 3 patients had anal lesions (2 fistulas and abscesses, 2 fissures).25
Grades of GI adverse effect according to National Common Terminology Criteria for Adverse Events V.4.0
Severe acute colitis can lead to colonic perforation and death, especially in cases of diagnostic delay. In prior reports, colon perforation occurred in 0.7%–1.5% of patients with melanoma29 33 and 6.6% of patients with renal cell carcinoma.29 In melanoma phase III trials, 0.6%–1% patients died of complications related to ipilimumab-induced enterocolitis.34 35 Diarrhoea and colitis are among the most frequent causes of treatment-related deaths in patients with cancer treated with immune checkpoint inhibitors36 and 31% of toxic deaths are due to GI events.7
Enterocolitis is the most frequent but not the only GI irAE induced by anti-CTLA-4. Indeed, two case reports have described enteric neuropathy induced by ipilimumab and revealed by severe constipation.37 38
Imaging findings
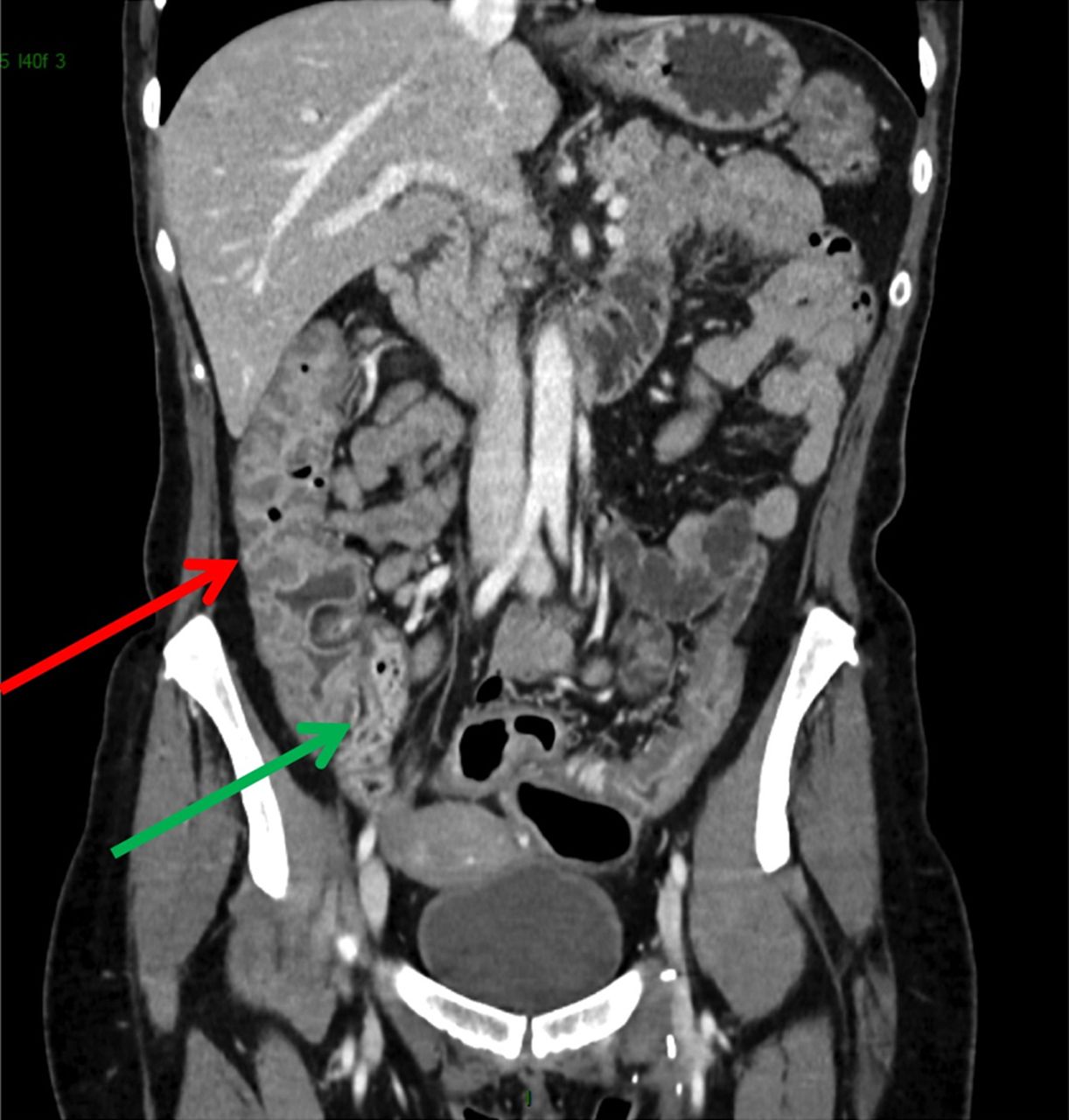
The common CT findings of colitis due to ipilimumab are mesenteric vessel engorgement, bowel wall thickening and colonic distension (figure 1).39 These findings may either be extensive or segmental, leading to a differential diagnosis that includes diverticular sigmoiditis.39 40 Thickening of the terminal ileum has also been reported.39 The positive predictive value of CT scan for enterocolitis is excellent (about 90%), but its negative predictive value is only moderate (40%–60%).40

Abdominal CT of a patient who received a combination of nivolumab and ipilimumab for melanoma. She had a severe diarrhoea and colitis. CT scan showed thickening of the colonic (red arrows) and ileal (green arrow) walls.
Endoscopic findings
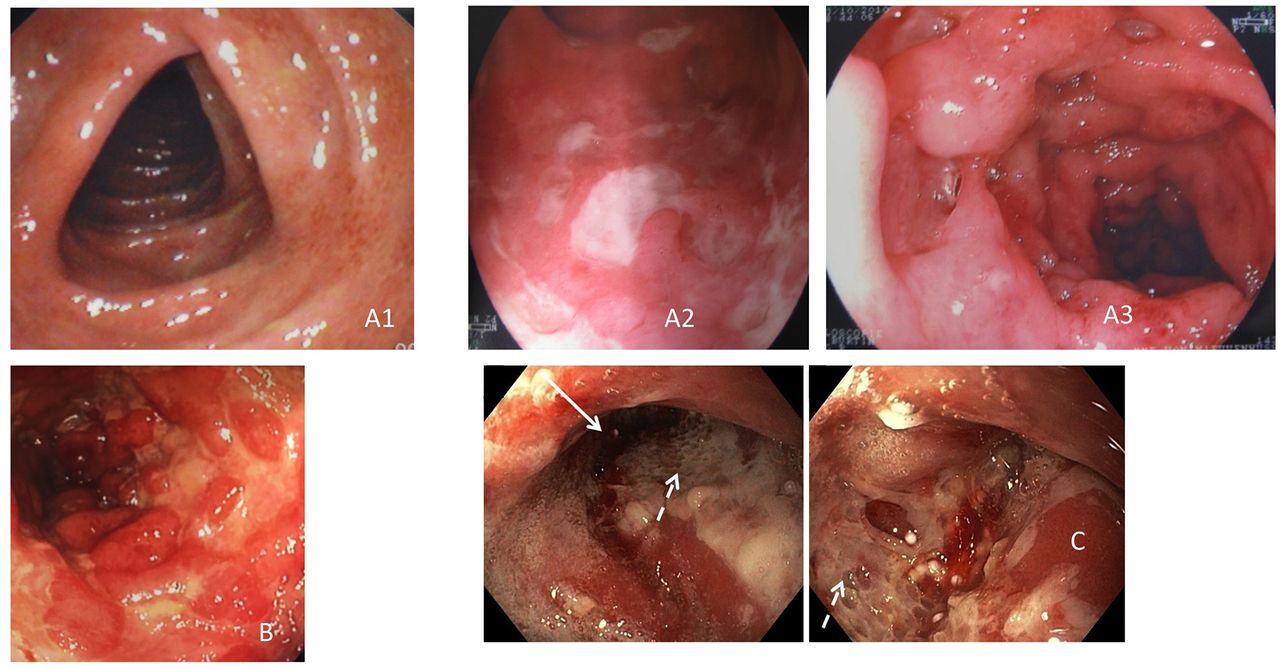
Early endoscopy findings (within 1–2 weeks of ipilimumab administration) before symptom onset do not appear to predict the occurrence of enterocolitis.17 In patients with established enterocolitis, lower GI endoscopy (flexible sigmoidoscopy or colonoscopy) shows erythema, erosion, ulceration and luminal bleeding (figure 2A).23 25 Ulcerations have been reported in 57%–79% of patients.25 26 41 At least two-thirds of patients have an extensive colitis, defined as endoscopic lesions proximal to the splenic flexure.24–26 Continuous pattern of inflammation has been reported in 45%–79% of patients.24 25 Most cases of enterocolitis involve the distal colon, which can be reached with a flexible sigmoidoscopy. Additionally, there appears to be a correlation between endoscopic severity and the need for infliximab treatment.24 41 Ileitis has been reported in 12% of patients and ipilimumab-induced enteritis without colitis has been reported as well.42 43

Colonoscopic findings observed in (A) anti-cytotoxic T-lymphocyte-associated protein-4 colitis. Disappearance of vascular pattern (A1), superficial ulcerations (A2), deep ulcerations (A3). (B) Anti-programmed death-1 (PD-1) enterocolitis. Deep ulcerations within the left colon. (C) Anti-PD-1 severe gastritis. Arrows indicate deep ulcerations.
Histological and immunopathological features
Histological features are generally those of acute colitis, including lamina propria expansion and acute inflammation characterised by infiltration of the lamina propria with neutrophils, and the presence of crypt abscesses.17 24 25 44 These inflammatory changes are diffuse rather than patchy in 75% of patients.17 Two studies have reported features of chronic IBD such as mononuclear cell infiltration, granulomas, basal plasmacytosis and crypt abnormalities (atrophy, distortion, branching, budding) in 40% of the patients.24 26 This chronic inflammatory process was found to infiltrate the submucosa in 47% of the patients.24 Another study, however, did not find histological signs of chronic colitis.25 Apoptotic cells in crypt epithelium have been reported in 42% of patients.24 Microscopic colitis has also been diagnosed in patients treated with anti-CTLA-4 antibodies.25 44 45 Interestingly, predominance of mucosal CD4+ lymphocytes in anti-CTLA-4-induced colitis was observed, with significantly higher tumour necrosis factor (TNF)-α secretion in anti-CTLA-4-induced colitis than in anti-PD-1-induced colitis.45 Histological inflammation of the stomach and the duodenum have been reported in 55% of patients treated with ipilimumab.25 In patients with ipilimumab-induced duodenitis, features of chronic duodenitis were observed (crypt distortion, focal and heterogeneous villus shortening, increased eosinophils and mononuclear inflammatory cells in the lamina propria as well as hyperplasia of Brunner’s glands), often with a patchy distribution and mild activity.25
Diagnosis and treatment management
Prophylactic budesonide (9 mg orally per day) was studied in a randomised, controlled trial and was found not to prevent ipilimumab-induced diarrhoea or colitis (figure 3).17 46

Management of diarrhoea/colitis due to Immune checkpoint inhibitors, based on ESMO guidelines.47 CMV, cytomegalovirus; CRP, C reactive protein; European Society for Medical Oncology.
Patients on ICI who develop diarrhoea should undergo a workup including complete blood count, serum electrolyte profile, search for stool enteropathogens and Clostridium difficile toxin.47
Grade 1 or 2 diarrhoea can be treated supportively with antidiarrhoeal drugs such as loperamide, oral fluid and a low-fibre diet. Oral corticosteroids (prednisolone 0.5–1 mg/kg/day or budesonide 9 mg/day in microscopic colitis) should be added in case of inadequate response, prolonged course or haematochezia.47
Patients with grade 3/4 diarrhoea or grade 1/2 and systemic symptoms (dehydration, fever, tachycardia) should discontinue ICI and receive intravenous corticosteroids (methylprednisolone 1 mg/kg/day).48 Flexible rectosigmoidoscopy or ileocolonoscopy and biopsies should be performed to confirm the diagnosis and assess severity. Abdominal CT is indicated in patients with severe acute colitis to diagnose perforation, colectasia and abscesses. Patients who respond to intravenous corticosteroids within 3–5 days should be switched to the oral form and tapered over 8–12 weeks. Infliximab (5 mg/kg), a TNF-α antagonist, is indicated in patients who fail to respond to intravenous corticosteroids. A single dose of infliximab is often sufficient to improve symptoms, although a second infusion 2 weeks later may be needed in some cases.23 25 29 33 49 50 Vedolizumab, a monoclonal antibody blocking α₄β₇ integrin, was administered to six patients with steroid-dependent or steroid-refractory enterocolitis due to ipilimumab.51 Time to steroid-free remission was 56 days, which is comparable to the time to spontaneous remission. Due to its delayed efficacy, vedolizumab is not a good option in patients with severe colitis due to anti-CTLA-4. Additionally, in refractory anti-CTLA-4 enterocolitis, CMV reactivation should be excluded by histology and immunohistochemistry of colonic biopsies as well as CMV PCR in the serum or whole blood.52 53
In rare cases, patients treated with anti-CTLA-4 may develop a toxic megacolon, intra-abdominal abscesses or a colonic perforation.25 54 These patients should undergo emergency subtotal colectomy with ileostomy.25 54 A management algorithm of diarrhoea and colitis in patients undergoing ICI therapy is proposed in figure 3.
Time to resolution of GI irAE related to anti-CTLA-4 ranges from 0.5 to 1.6 months,23 55 although chronic colonic inflammation has been found several months after the onset of enterocolitis in asymptomatic patients.25 55 In fact, a recent report describes a patient who developed IBD 2 years after grade 3 ipilimumab-induced enteritis and ipilimumab discontinuation.56
Anti-PD-1-induced GI irAE
The relative risk of colitis of any grade for patients treated with anti-PD-1 monotherapy is 0.20 (95% CI 0.07 to 0.62; p=0.005) as compared with patients treated with anti-CTLA-4 monotherapy.57
The median time to onset of GI irAE associated with anti-PD-1 therapy is later than with anti-CTLA-4 treatment, and generally occurs 2–4 months after treatment initiation.58–60 Delayed occurrence of GI irAE, up to 1 year after initiation of anti-PD-1 therapy has also been reported.61 In addition, recurrent colitis has been observed in patients who had been off anti-PD-1 therapy up to 11 months.62
Clinical presentation
The most common symptoms described are abdominal pain, diarrhoea and nausea.59 60 63 Four categories of anti-PD-1 GI irAE have been described: acute colitis (40%), microscopic colitis (35%), upper GI tract inflammation including necrotising gastritis (20%) and pseudo-obstruction (5%).59
Mouth ulcers or anal lesions have not been observed in patients with GI irAE related to anti-PD-1, in contrast to anti-CTLA-4.59 60
Endoscopic findings
The endoscopic lesions found in lower GI endoscopies are erythema, luminal bleeding, erosions and ulcerations59 64 (figure 2B), with a patchy distribution reported in 75% of cases. Two-thirds of patients investigated for GI irAE related to anti-PD-1 had an abnormal upper GI endoscopy, 10.5% (n=2) of them with necrotising gastritis59 (figure 2C).
Histological and immunopathological features
Acute colitis and microscopic colitis including lymphocytic colitis and the less common collagenous colitis have been reported.45 59 60 62 65–67 Active colitis is the most common pattern of injury observed, with neutrophilic crypt microabscesses and with prominent crypt epithelial cell apoptosis and crypt atrophy/dropout. Granulomas may be observed in association with ruptured crypts.60 In patients who experienced recurrent anti-PD-1 colitis, features of chronicity such as basal lymphoplasmacytosis and crypt architectural irregularity are reported many months after cessation of anti-PD-1 therapy.62 Colonic mucosal lymphocytes are predominantly CD8+ T cells in anti-PD-1-induced colitis,45 which differs from the predominance of CD4+ T cells observed in anti-CTLA-4-induced colitis.68 69
Inflammation of the upper GI tract, that is, oesophagitis and gastritis, can be induced by anti-PD-1. Histological features observed in gastric biopsies are intraepithelial lymphocytosis, inflammatory infiltrate with neutrophils and in rare cases, necrosis of the epithelium.59 67 70 Duodenal biopsies showed partial villous blunting, intraepithelial lymphocytosis and lymphocytic and plasma-cell infiltration of the lamina propria.59
Diagnosis and treatment management
Diagnosis and management of GI irAE due to anti-PD-1 parallel the approach described above for anti-CTLA-4.47 71 A similar workup to rule out enteric pathogens and alternate aetiologies is appropriate. It is noteworthy, however, that, in a study of 44 patients referred to a digestive care unit for suspected anti-PD-1-induced GI irAE, half had alternative aetiologies identified, including intestinal metastases of non-small cell lung cancer.59
As in anti-CTLA-4-induced colitis, most patients respond to corticosteroids, including up to 87.5% of patients with acute colitis and 57% of patients with microscopic colitis.59 Most patients (75% in our experience) with upper GI inflammation respond to corticosteroids. They may need parenteral nutrition or postpyloric enteral nutrition, because of vomiting and anorexia. Some patients with steroid-refractory colitis improved with infliximab, but data are scarce.59 63 72 Patients with anti-PD-1-induced GI IrAE have received mesalazine, vedolizumab,51 tocilizumab and adalimumab-methotrexate combination with reported improvement.73–75 One patient who had skin and GI irAE induced by pembrolizumab improved with secukinumab but subsequently lost antitumour efficacy.76
Time to resolution of GI irAE related to anti-PD-1 ranges from 1.1 to 4.2 months,58 59 with an often protracted course in microscopic colitis.
Table 3 highlights the differences between anti-PD-1 and anti-CTLA-4-induced GI irAE.
Differences in anti-PD-1 and anti-CTLA-4 GI immune adverse events
Enterocolitis associated with combination of anti-CTLA-4 and anti-PD-1
Anti-CTLA-4 (ipilimumab) and anti-PD-1 (nivolumab) antibodies used in combination results in objective responses in >50% of the patients with metastatic melanoma.77–79 The safety profile is related to the dose of ipilimumab.32 At the standard dose of 3 mg/kg of ipilimumab every 3 weeks in combination with nivolumab 1 mg/kg every 3 weeks, grade 3–4 diarrhoea and colitis occurred in 9%–10.7% and in 8%–17%, respectively.77 79–81 In contrast, grade 3–4 GI irAE were observed in <5% of patients treated with a combination of nivolumab and ipilimumab at a reduced dose of 1 mg/kg every 3, 6 or 12 weeks.6 82 Clinical presentation, endoscopic findings and management recommendations of enterocolitis induced by combination therapy parallel those described above for anti-CTLA-4 and anti-PD-1-induced colitis.32 Median time to symptom onset and time to resolution were approximately 5 and 3 weeks, respectively, in a pooled safety data analysis of 407 patients with advanced melanoma treated with ipilimumab plus nivolumab.83
Immune-related enterocolitis, antitumour response to ICI and immunosuppressive agents
Some, but not all,33 studies have suggested that antitumour response is higher in patients with irAE.46 84 In a series of 576 patients treated with nivolumab for advanced melanoma, objective response rate was significantly higher in patients who experienced irAE of any grade, compared with those who did not.58 Furthermore, an overall survival advantage was noted among patients with any grade of irAE versus those without (p≤0.001), and in those who reported three or more irAE events (p≤0.001).85 In addition, several studies have found associations between ipilimumab-induced enterocolitis and objective response rate or overall survival.29 84 The use of immunosuppressive agents for irAE (corticosteroids, infliximab or mycophenolic acid) does not seem to be associated with a diminished efficacy of ICI.24 33 58 86 87
Risk of recurrent GI irAE after reintroduction of immune checkpoint inhibitors
Discontinuation rates of ICI range between 3% and 12% in anti-PD-1 trials and between 3% and 25% in anti-CTLA-4 trials. The most common irAE leading to discontinuation are diarrhoea and colitis7; therefore, the question of reintroducing ICI after GI irAE is an important one.
In patients who previously experienced an enterocolitis due to ipilimumab, subsequent treatment with anti-PD-1 antibodies only rarely (1/47; 2%) resulted in recurrent enterocolitis.15 88 However, new grade 3/4 irAE occurred more frequently (21%)15 in patients who previously experienced a major irAE with ipilimumab, as compared with the whole population of patients treated with anti-PD-1 after having received ipilimumab (8%).58
Most patients with enterocolitis associated with anti-PD-1/anti-CTLA-4 combination therapy, tolerated subsequent anti-PD-1 monotherapy well. Enterocolitis was less likely than other irAE to recur on anti-PD-1 rechallenge after combotherapy discontinuation (6% vs 28%, respectively, p=0.01).89
In a series of 26 patients who experienced a GI irAE during a first line of ICI and received a second course of ICI, we have observed a recurrence of GI irAE in six patients (23%), including 2/26 (7.7%) patients with grade 4 GI irAE. There was a trend towards a higher recurrence rate when the second line was an anti-CTLA-4, rather than an anti-PD-1 (logrank test: 0.11).55
The decision to reintroduce ICI should be made on a case-by-case basis, and discussed within a multidisciplinary team.
The role of gut microbiota in intestinal inflammation and antitumour response induced by immune checkpoint inhibitors
The impact of anti-CTLA-4 and anti-PD-1 antibodies on the immune system is described in figure 4.

Role of cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) (panel A) and programmed death-1 (PD-1) (panel B) in immunoregulation. (A) T-cell activation requires binding of the T-cell receptor to the antigen in association with major histocompatibility complex (MHC). It also needs binding of CD80 and CD86 ligand on the antigen-presenting cells (APC) with CD28 costimulatory receptor on the T cells.111 112 CTLA-4 is a homologue of CD28, which binds CD80 and CD86 with higher affinity, and thereby downregulates T-cell activation. CTLA-4 also inhibits T-cell activation by other mechanisms such as inhibition of CD28 costimulation by cell-extrinsic depletion of ligands, a mechanism referred to as transendocytosis.113 CTLA-4 exerts its immunoregulatory effect on T cells that are primed in lymphoid organs such as the T-cell zone of draining lymph nodes. Anti-CTLA-4 monoclonal antibodies block CTLA-4’s interaction with CD80 and CD86 favouring CD28 engagement, and consequently, T-cell activation and proliferation.114–116 Anti-CTLA-4 monoclonal antibodies abolish the inhibitory mechanism only on T cells that were previously challenged by an antigen, and not all T cells. This effect is seen irrespective of the antigen specificity, and therefore affects a much wider repertoire of T cells than those involved in the antitumour response. This broad effect on T cells, explains why CTLA-4 blockade is associated with numerous and varied irAE. (B) In contrast with CTLA-4, which downregulates the early phase of T-cell activation within lymph nodes, PD-1 regulates T-cell activation at a later stage within chronically inflamed, peripheral tissues, particularly in the cancer microenvironment.117 PD-1 is expressed on exhausted T cells such as tumour-infiltrating lymphocytes, and among B lymphocytes, natural killer cells, monocytes and dendritic cells.118–120 PD-1 is also highly expressed on intratumoural Treg cells and may enhance their immunosuppressive activity.121–124 PD-1 pathway does not inhibit costimulation but inhibits signalling downstream of the T-cell receptor (TCR). PD-1 ligation reduces the expression and production of cytokines and transcription factors, such as GATA3 and TBET, which are associated with effector T-cell function.125–128 PD-1 has two ligands: PD-L1 and PD-L2. PD-L1 is expressed by cancer cells and tumour-infiltrating macrophages, while PD-L2 is expressed by APCs.121 129 PD-1 blockade by monoclonal antibodies (nivolumab and pembrolizumab) can provoke a peripheral, antitumour immune reaction.
A variety of tumour and host factors can affect the efficacy of antitumour immunity and cancer immunotherapy. Activation of the Wnt/β-catenin pathway, deletion or mutation of phosphatase and tensin homologue (PTEN) germline, polymorphisms in immune regulatory genes (CCR5, CTLA-4, PD-L1), microsatellite instability and mutational load may influence the efficacy of ICI.79 90–94 A recent study failed to demonstrate a significant association between irAE and seven single nucleotide polymorphisms (SNPs) in four genes, which are considered contributors to PD-1-directed T-cell responses, that is, PDCD1, PTPN11, ZAP70 and IFNG.95
There is accumulating experimental and clinical evidence (table 4) that the gut microbiome is involved in antitumour response and the development of enterocolitis induced by ICI. Tumours in antibiotic-treated or germ-free mice do not respond to CTLA-4 blockade, and antitumour effect is restored with faecal microbial transplantation. Studies of faecal transplantation from patients with melanoma to recipient mice have shown that bacteria from the Bacteroides genus (Bacteroides fragilis and Bacteroides thetaiotaomicron) enhance the antitumour effect of CTLA-4 blockade.96 Similar experiments have been performed with anti-PD-L1 and have shown that antitumour efficacy was mediated by Bifidobacterium species.97
Associations between baseline gut microbiota and GI immune-related adverse events, as well as antitumour response in human patients
The first study in humans to assess the link between gut microbiota and antitumour response as well as enterocolitis due to anti-CTLA-4 antibodies was performed in patients with melanoma.84 Colonisation by Firmicutes, such as Faecalibacterium prausnitzii L2-6, butyrate-producing bacterium L2-21, Gemmiger formicilis ATCC 27749, was associated with antitumour response and subsequent immune-related colitis (table 4). In contrast, Bacteroidetes (mostly Bacteroides genus) were more highly represented in patients who had a poor antitumour response and in those who remained colitis-free. While in mice anti-CTLA-4 treatment induced a microbial dysbiosis,96 in patients with melanoma, the gut microbiota was not significantly modified over the course of the ipilimumab treatment. However, development of immune-related enterocolitis was associated with a shift in the gut microbial composition and decreased bacterial diversity. The proportions of seven genera were significantly reduced; they all belonged to the Firmicutes phylum and were dominant members of the microbiota. The study by Dubin et al also found an increased representation of Bacteroidetes phylum among patients who remain free of ipilimumab-induced colitis.98 Another group found that the gut microbiome was enriched for F. prausnitzii, Bacteroides thetaiotaomicron and Holdemania filiformis in patients who responded to ipilimumab/nivolumab combination therapy.99
Three recent studies have reported a link between intestinal microbiota composition and response to anti-PD-1 (table 4). The first study showed that patients who had received antibiotics responded less well to anti-PD-1.100 There was a higher representation of Firmicutes as well as genera such as Akkermansia and Alistipes, in responders as compared with non-responders. There was a correlation between TH1 activity towards Akkermansia muciniphila and progression-free survival (PFS). Faecal transplantation from anti-PD-1 treatment responders and non-responders to mice has shown that A. muciniphila and Enterococcus hirae enhanced anti-PD-1 efficacy. This was correlated with increased CD4/FOXP3 expression within the tumour and increased IL-12 secretion by dendritic cells. The second study showed a correlation between response to anti-PD-1 and composition of intestinal microbiota, while there was no association with oral microbiota.101 Gut microbiota diversity was higher in responders. Furthermore, intestinal microbiota was enriched in the families Clostridiales in responders and in Bacteroidales in non-responders. Faecalibacterium genus was enriched in responders, whereas B. thetaiotaomicron, Escherichia coli and Anaerotruncus colihominis were over-represented in non-responders. In univariate study, the best predictors of response were gut microbiota diversity, and Faecalibacterium as well as Bacteroidales abundance. Faecal transplantations from responders and non-responders to anti-PD-1 to mice have confirmed the importance of Faecalibacterium in influencing response. The third study also found that the ratio of beneficial to non-beneficial operational taxonomic units (OTUs) was the strongest predictor of response to anti-PD-1.102
In the study by Chaput et al, patients who belonged to Faecalibacterium-driven cluster had a higher increase in ICOS+ CD4 T cells (in proportion and absolute number) under ipilimumab.84 A recent study based on T-cell mass cytometry has shown that anti-CTLA-4, but not anti-PD-1, modulates the CD4 effector compartment, specifically inducing the expansion of an ICOS+ Th1-like CD4 effector subset.103 In addition, expansion of ICOS+ CD4 T cells is correlated with overall survival following ipilimumab therapy.104 Patients with melanoma treated with anti-PD-1 whose intestinal microbiota were enriched in Faecalibacterium, Ruminococcaceae and Clostridiales, had a higher number of baseline intratumoural CD8+ T cells.101 In the study by Routy et al, the only immune responses that correlated with the clinical outcome during anti-PD-1 therapy were Th1 and Tc1 cell reactivity against A. muciniphila.100 Interferon-γ release above the median was associated with prolonged PFS. Mice fed with A. muciniphila had increased intratumoural CD4/Foxp3 ratios and increased secretion of IL-12 by dendritic cells.
Taken together, these data suggest that patients whose gut microbiota contains high amounts of symbionts such as F. prausnitzii and A. muciniphila have more potent T-cell activation systemically and within the tumour. Therefore, they have a stronger antitumour response to both anti-CLTA-484 and anti-PD-1100 101 and a higher risk of developing anti-CTLA-4-induced enterocolitis.84 A unifying hypothesis, displayed in figure 5, may be proposed to explain the links between microbiota, and antitumour response to CLTA-4 and PD-1 blockade as well as enterocolitis due to anti-CTLA-4. The mechanisms by which symbionts enhance T-cell activation provoked by immune checkpoint inhibitors remain to be elucidated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A hypothesis linking microbiota to T-cell response, intestinal inflammation and antitumour response. One can hypothesise that the antitumour effect of anti-cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) is mediated by gut microbiota via intestinal inflammation and translocation of selected bacteria, as has been shown with cyclophosphamide.132 However, symbionts such as Faecalibacterium prausnitzii are associated with antitumour response to both anti-CTLA-4 and anti-programmed death-1 (PD-1). Anti-CTLA-4 is frequently associated with intestinal inflammation, whereas this is rarely the case for anti-PD-1. In addition, gut microbiota is not significantly modified over the course of the ipilimumab treatment. Taken together, these data suggest that intestinal inflammation is not necessary for the antitumour effect of symbionts. We postulate that eubiotic microbiota is associated with a marked and non-selective T-cell activation in response to anti-CTLA-4 (panel A) and anti-PD-1 (panel B). This leads to an antitumour response with both classes of drugs, and to intestinal inflammation in patients treated with anti-CTLA-4. Indeed, CTLA-4 plays a pivotal role in the maintenance of intestinal immune homeostasis.133–135
Although our study of 16S rRNA-based sequencing found that the same group of symbionts were associated with both antitumour response and enterocolitis,84 metagenomics may help distinguish the bacterial strains responsible for these two distinct effects. A recent study showed that while anti-CTLA-4 aggravated dextran sulfate sodium (DSS)-induced colitis in mice, pretreatment with Bifidobacterium largely attenuated intestinal inflammation without any detriment to the antitumour effect of anti-CTLA-4. The protective effect of Bifidobacterium appeared to be mediated by Treg cells.105 Yet, in mice, anti-CTLA-4 alone does not induce colitis. Moreover, another group has found that anti-CTLA-4 attenuated rather than aggravated DSS-induced colitis in mice.106
Enterocolitis associated with immune checkpoint inhibitors and naturally occurring IBD
IBD is associated with gut microbial dysbiosis. Microbial features that have been reproducibly found in adult IBD are a decreased number of non-redundant bacterial genes and reduced overall diversity of the microbiota, increased percentage of Actinobacteria and Enterobacteriaceae including Escherichia coli and decreased representation of putative anti-inflammatory bacteria from the Firmicutes phylum, more specifically F. prausnitzii, and several butyrate-producing species.107 108 It is not clear as to whether dysbiosis precedes or follows intestinal inflammation. However, the current theory of IBD hypothesises that dysbiosis, induced by genetic and environmental factors such as Western diet and repeated antibiotic treatments, precedes intestinal inflammation.109 Anti-CTLA-4-induced enterocolitis is associated with a dysbiosis that does not precede intestinal inflammation, and rather appears concomitantly with it. Indeed, the reverse was observed; patients whose gut microbiota was enriched in symbionts such as F. prausnitzii or A. muciniphila were at the highest risk for developing enterocolitis.
Abatacept, a fusion CTLA-4-Ig protein that blocks T-cell activation, has proven ineffective in CD and UC.110 However, IBD is clinically and genetically heterogeneous. It is possible that the pathophysiogical scheme of ipilimumab-induced colitis may apply to a subgroup of IBD. To this regard, the clinical and endoscopic picture of colitis induced by anti-CTLA-4, either alone or combined with anti-PD-1, is closer to UC than CD.
Conclusion
Enterocolitis due to anti-CTLA-4 therapy is frequent, potentially severe and shares some similarities with naturally occurring IBD. GI irAE associated with PD-1 blockade appears to be less frequent and clinically more diverse. In enterocolitis induced by anti-CTLA-4, dysbiosis is the consequence, not a predisposing factor of intestinal inflammation. Symbiotic gut microbiota with high proportions of F. prausnitzii or A. muciniphila is associated with an enhanced antitumour response to ICI and to increased susceptibility to developing enterocolitis in patients treated with anti-CTLA-4. These findings open new perspectives for possible manipulation of the gut microbiota (ie, faecal transplantation or microbial complementation), with a view to better identify responders to ICI and to increase their efficacy and safety.
Acknowledgments
The authors would like to thank Jill Gregory, graphic illustrator at Icahn School of Medicine at Mount Sinai, New York City, NY, USA.
References
Footnotes
ES, PL, CR and FC contributed equally.
Contributors ES and FC performed the systematic literature review and wrote the first draft of manuscript; JFC and DF contributed to the writing of the manuscript. PL contributed of the acquisition of data and writing of microbiota section. Others contributed to the acquisition of data and critical appraisal of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Franck Carbonnel received boards or lecture fees from enterome, MSD, BMS, Janssen, Pfizer, AbbVie, Mayoly Spindler, Takeda, Pileje Jean Frédéric Colombel: Consultant or advisory board member for AbbVie, Amgen, Boehringer-Ingelheim, Arena Pharmaceuticals, Celgene, Celltrion, Enterome, Eli Lilly, Ferring Pharmaceuticals, Genentech, Janssen and Janssen, Medimmune, Merck & Co, Nextbiotix, Novartis Pharmaceuticals, Otsuka Pharmaceutical Development & Commercialization, Pfizer, Protagonist, Second Genome, Gilead, Seres Therapeutics, Shire, Takeda, Theradiag. Speaker for AbbVie, Ferring, Takeda, Celgene. Stock options: Intestinal Biotech Development, Genfit Research grants: AbbVie, Takeda, Janssen and Janssen.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.