Article Text

Abstract
Objective Immune checkpoint inhibitors like anti-programmed cell death protein 1 (PD-1) drugs Nivolumab and Pembrolizumab and anti-cytotoxic T-lymphocyte associated (CTLA-4) drug Ipilimumab have become standard of care in many metastatic cancers. Immunotherapy-related hepatitis and cholangitis present a diagnostic and management challenge, being rare and incompletely characterised. We aim to report the incidence, features and treatments used for this in a real-world setting and to identify useful biomarkers, which can be used to predict effective use of steroids.
Design Retrospective review of 453 patients started on immunotherapy over 7 years.
Setting Tertiary hepatology and oncology centre.
Patients 21 patients identified with immunotherapy-related hepatotoxicity.
Results Hepatitis was most common in those receiving dual therapy (incidence 20%), with 75% of Grade 4 hepatitis cases occurring with ipilimumab-containing regimens. Corticosteroid monotherapy is first line treatment, but doses above 60 mg OD prednisolone do not demonstrate any additional benefit in time to hepatitis resolution. The alanine transaminase (ALT) reduction in steroid-responsive hepatitis is typically rapid (with a halving of ALT within 11 days). The commencement of additional immunosuppression (typically mycophenolate) appears safe and prompts a more rapid fall in ALT than corticosteroid use alone. Infliximab was safely used twice as hepatitis treatment. We also describe one patient with rare immunotherapy-induced biliary disease.
Conclusions Vigilance is required for detection of immunotherapy-associated liver disease as, other than dual immunotherapy, we can identify no predictive factors for its development. Our data suggest that corticosteroid response is not dependent on the higher dosing regimens. Early escalation of immunosuppression may be of benefit in the absence of a rapid response to corticosteroids.
- checkpoint inhibitor
- hepatitis
- immunotherapy
- drug-induced liver injury
Statistics from Altmetric.com
Significance of this study
What is already known on this topic
Immune checkpoint inhibitor (ICPI) therapy results in a variety of autoimmune reactions affecting different organs including the liver.
There is no significant difference in survival between those patients who developed ICPI hepatitis and those who did not.
Corticosteroids are the first-line treatment for immunotherapy-related hepatitis.
What this study adds
Treatment escalation should be to an additional steroid sparing agent (SSA) rather than an increased dose of steroid if the ALT does not respond rapidly as higher doses are not more effective.
There are no clear clinical biomarkers predicting who will require SSAs in addition to steroid therapy for hepatitis.
There are two potential groups of non-responders—those who develop a clear failure of therapy with a ‘rapid ALT rise’ hepatitis and those where the ALT shows a more delayed rise, with no immediate response to starting therapy.
Although liver immune-related adverse event usually manifests as a hepatitis, it can also manifest in a predominant biliary pattern.
How might it impact on clinical practice in the foreseeable future
Consider escalation of treatment early in cases where the ALT does not recover within a few days though this strategy needs to be validated in larger numbers of patients.
Patients can be rechallenged with another type of immunotherapy without getting further hepatotoxicity.
Background
Immune checkpoint inhibitors (ICPIs) represent a novel class of oncological therapy that increase survival in patients with various tumours. These revive exhausted immune populations that then react against cancer cells through blocking physiological anergic pathways involving the programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte associated (CTLA) proteins. While ICPIs are known to deliver durable responses and are being trialled in an expanding number of cancer types,1–10 there is caution in their use because of immune-related adverse events (irAEs) that can affect multiple different organ systems.11
Liver irAEs are uncommon and vary in severity from mild to life-threatening. Reports suggest the predominant histological pattern of liver injury is a pan-lobular hepatitis resembling autoimmune hepatitis12–14 and more rarely, fibrin ring granulomas.15 The factors predisposing to liver irAEs and whether pre-existing liver conditions confer an increased risk for irAEs are unknown. Furthermore, many clinical trials excluded patients with such conditions and/or organ dysfunction.16 There are reports of immunotherapy use in patients with viral hepatitis17 and recent evidence suggests that both anti-CTLA-418 and anti-PD-119 monotherapy, respectively, can be safely administered to patients with pre-existing autoimmune disease without increased severe toxicities.20 The Food and Drug Administration (FDA) and American Society of Clinical Oncology (ASCO) have championed the expansion of clinical trial eligibility criteria, which may aid in the characterisation of the safety of immunotherapies in these patients with pre-existing liver disease.21 22
We present a cohort of patients identified to have liver irAEs.
Methods
A total of 453 patients started checkpoint inhibitor therapy at a single tertiary centre between December 2011 and June 2018. Electronic patient records and oncology databases were retrospectively analysed for clinical data on two occasions by separate teams. Analysis was conducted using GraphPad PRISM and IBM SPSS software. Type and number of cycles of immunotherapy, cancer type, survival, biochemistries and treatment received were recorded for all patients with liver irAEs. Checkpoint-inhibitor-associated liver disease was graded according to the Common Terminology Criteria for Adverse Events (CTCAE) V.5.23 The choice of therapy, threshold for starting and of escalation varied by clinical context but was in line with national and local guidelines (online supplementary file 1). Briefly, if hepatitis was more severe than Grade 1, intravenous methylprednisolone or oral prednisolone was started, followed by escalation to steroid sparing agents (SSAs) such as mycophenolate mofetil (MMF) (in 1 g two times a day or 500 mg two times a day doses), Tacrolimus or Infliximab (5 mg/kg) if necessary. Treatment failures represent disease courses where therapy for ALT control was unsuccessful as assessed at 7 days. Treatment failure ‘Rapid Risers’ were defined as those where the ALT rose within 7 days, and ‘Slow risers’ as those where the ALT remained stable despite initiating treatment.
Supplemental material
Results
In total, 21 patients with liver irAEs and their clinical features are shown in table 1. Twenty patients were categorised as having developed checkpoint inhibitor-associated hepatitis, an incidence of 4% which is comparable to published literature.24 25 One patient developed biliary pathology (Identifier, _272). Two further patients with abnormal LFTs were excluded from analysis—one had underlying Hepatitis C infection, and the other was a trial patient who remained blinded to checkpoint inhibitors versus placebo.
Clinical data for all patients who had abnormal liver function tests I
Patients received various regimens, including monotherapy and dual therapy with both CTLA-4 and PD-1 inhibitors. One patient developed hepatitis separately on both anti-CTLA-4 (Ipilimumab) and anti-PD-1(Pembrolizumab) therapy (Identifier: _07).
Seventeen patients had ICPI treatment for melanoma, two for Lung Cancer (Identifiers _272, _896) and one each for Renal cell cancer (Identifier: _42) and Epithelial Mesothelioma (Identifier: _92). In 12 patients, checkpoint inhibitors were given as first-line systemic therapy, and in 6 patients, it was second-line therapy (previous Pemetrexed, Dabrafenib, Carboplatin, Bevacizumab or PAN-RAF inhibitor) and in 2, it was third-line therapy (previous Dabrafenib-Trametinib or Sunitinib-Cabozantinib). The remaining patient had received hormone therapy for breast cancer (Letrozole). No patient had prior autoimmune disease.
Clinical outcomes
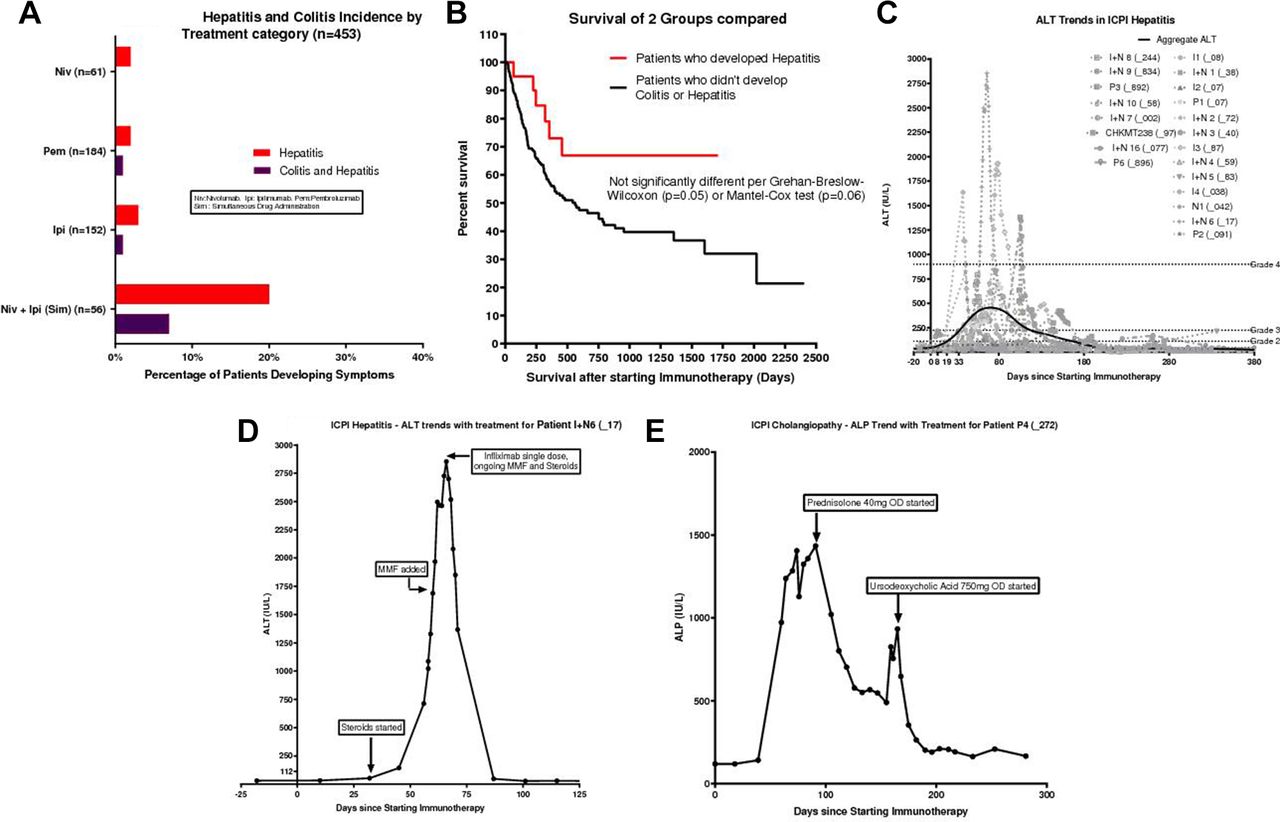
The median follow-up time for patients in the hepatitis cohort was 456 days (range 46–1710 and mean 524 days. Hepatitis was most common for patients who received simultaneous dual therapy (20%; figure 1A, table 2), mirroring trends in ICPI colitis.26

(A) Incidence of hepatitis and colitis in a 2011–2018 single tertiary centre cohort of patients receiving different treatment regimens. Combination therapy represented separately to single therapy. Demonstrates highest incidence in those receiving simultaneous PD-1 (Nivolumab) and CTLA-4 (Ipilimumab) therapy. (B) Survival after initiation of ICPI therapy in this cohort of patients compared to patients who did not develop ICPI hepatitis or colitis. Trends towards improved survival if develop hepatitis, but not significant. (C) Individual and aggregate (Lowess) trends in ALT (liver inflammation biomarker) after initiation of ICPI therapy for all patients with ICPI hepatitis. (D) ALT trends in a single patient after initiation of ICPI therapy. Distinct patterns of response to different drugs, with inflammation not responding to addition of steroids or MMF but responding to a single dose of Infliximab. (E) ALP (cholestasis biomarker) in a single patient with ICPI cholangiopathy as well as response to steroids and UDC. I=Ipilimumab, I+N=Ipi+Nivolumab, N=Nivolumab, P=Pembrolizumab. CHKMT238=Blinded to receive either Ipilimumab or Nivolumab. Suffixes (_08, _17 and so on) represent individual patient codes. CTLA, cytotoxic T-lymphocyte associated; ICPI, immune checkpoint inhibitor; MMF, mycophenolate mofetil; PD-1, programmed death 1; UDC, ursodeoxycholic acid.
Clinical features and management outcomes of ICPI hepatitis
In line with previous published series, there was a trend towards, but no significant difference in survival between those patients who developed ICPI hepatitis and those who did not (figure 1B).27 28
All hepatitis patients were diagnosed and managed empirically without liver biopsy. ALT was the most consistently measured and sensitive biomarker (figure 1C). Bilirubin, ALP and Albumin underwent smaller fluctuations (online supplementary file 2A-C), whereas the PT and INR did not change (not shown).
Supplemental material
Treatment response
ICPI hepatitis was treated with steroid induction (18/20 patients, the remaining patients had Grade 1 hepatitis). Immunotherapy was withheld until the ALT normalised.
Treatment successes
All patients were managed in line with national and local guidelines. We subdivided patients depending on whether the hepatitis responded to steroid monotherapy (typically intravenous methylprednisolone followed by PO prednisolone or PO prednisolone alone) or required the addition of SSAs if monotherapy failed by day 7. There was no link between clinical characteristics such as patient gender or immunotherapy regimen with the requirement for SSAs plus steroids versus steroids alone (online supplementary file 3).
Supplemental material
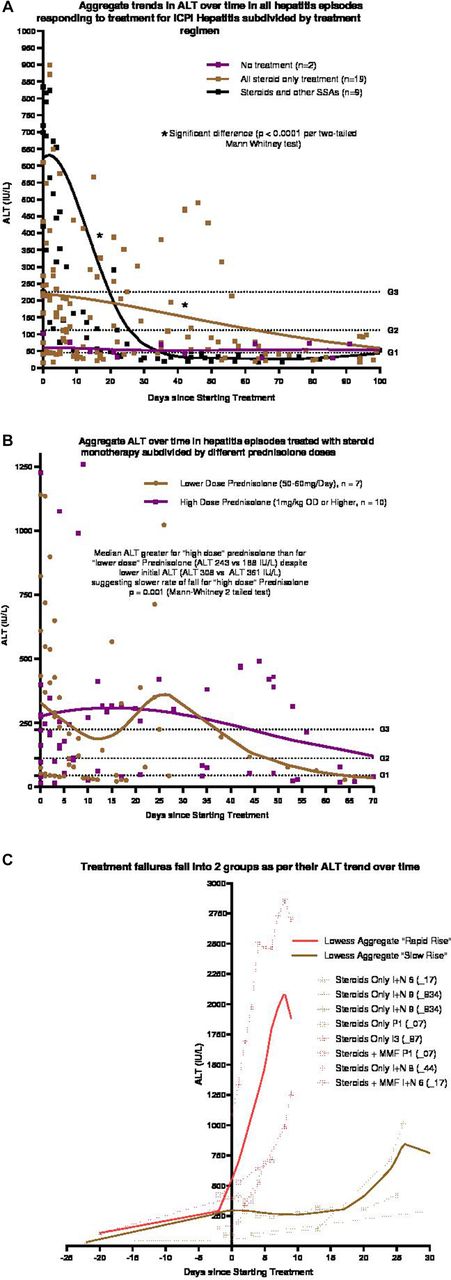
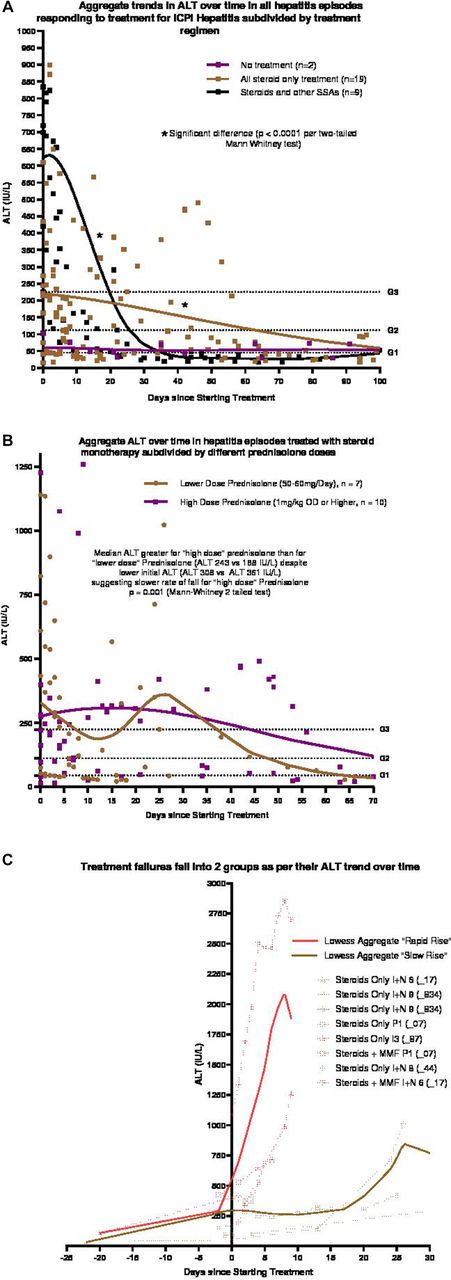
The aggregate trends for the fall in ALT (figure 2A, individual trends in online supplementary file 2) show a slower drop in ALT for those treated with steroid monotherapy as compared with those treated with a second immunosuppressive agent, despite a higher ALT at SSA initiation. This suggests that addition of a second immunosuppressive agent accelerates time to resolution, with no adverse effect on survival (online supplementary file 3).
{kind=link}
{kind=link}
(A) Lowess curves (aggregate ALT trends) comparing three ICPI hepatitis groups—episodes treated with steroids alone, those with steroids as well as SSA and those receiving no therapy. The rate of decrease of ALT with the addition of a SSA is significantly faster to steroid monotherapy. (B) ICPI hepatitis ALT trends in response to treatment with two different doses of steroids. Lowess curves (aggregate ALTs) represented for each cohort. Using a higher dose of prednisolone (1 mg/kg) does not accelerate the rate of fall of ALT and instead shows that response may be slower, despite a lower starting aggregate ALT. (C) Individual ALT trends (dotted lines) in all ICPI hepatitis episodes that failed initial immunosuppressive therapy. Supervised clustering of individual trends reveals two patterns of ALT rise, ‘Fast’ and ’Slow’, with the Lowess curves (aggregate ALT) for each represented. Individual ALT trends colour coded by whether they fell into the ‘Fast’ or ‘Slow’ category. I=Ipilimumab, N=Nivolumab, P=Pembrolizumab, I+N=Simultaneous Ipilimumab and Nivolumab therapy, CHKMT238=Blinded Ipi vs Niv. Suffix (_08,_07) and so on=individual patient codes. ICPI, immune checkpoint inhibitor; IFX, infliximab; MMF, mycophenolate mofetil; SSA, steroid sparing agents.
Notably, two patients in this cohort received Infliximab—one for treatment of ICPI hepatitis and one for ICPI colitis (while having no hepatitis at the time of the colitis). In one case, there was clear improvement (figure 1D). In the other, the ALT was measured for 112 days after the drug was administered and remained normal, that is, no medication-induced hepatotoxicity was seen.
Treatment failures
All ALT trends in individual hepatitis flares which initially failed control therapy, are shown in figure 2. Despite small numbers, a supervised clustering approach delineated two potential patterns. In the first week after escalating immunosuppression for hepatitis, the cohort of ‘rapid risers’ had an ALT rise of 100 IU/L per day, whereas the ‘slow risers’ showed either no response to treatment or an increase in ALT by an average of 5 IU/L per day. Although all ‘slow risers’ were initially on steroid monotherapy only, two of the three only responded after the addition of two SSAs, specifically MMF and either Tacrolimus or Infliximab.
Effect of steroid doses
The data were analysed for the effect of steroid doses within the successful steroid-only cohort. Two broad categories were identified—patients treated with a ‘lower dose’ regimen of 50–60 mg Prednisolone and those treated with a higher 1 mg/kg daily dose.
A higher prednisolone dose did not shorten the time to ALT normalisation, despite the aggregate ALT being higher at baseline in patients treated with a lower prednisolone dose. The data appear to show no clear benefit to using a higher steroid dose.
Rechallenge with immunotherapy
Four patients with ICPI hepatitis were given further immunotherapy after resolution of Liver function tests. Patients I+N5(_83) and I+N4(_59) who both developed combination immunotherapy associated hepatotoxicity were given maintenance nivolumab and they have had 8 and 19 cycles, respectively, without hepatotoxicity so far. Patients I+N2(_72) and I+N9(_834) were given second line Pembrolizumab after hepatotoxicity with combination immunotherapy and have tolerated 10 and 2 cycles, respectively, to date.
ICPI cholangiopathy
One patient developed a predominantly cholestatic pathology on ICPI (table 1, figure 1C). The elevation in ALP was markedly more than in ICPI hepatitis, whereas the rise in ALT was more modest. The trends for Bilirubin and Albumin were similar.
Late peaks of ALP in the time course of the treatment were due to reintroduction of ICPI drugs, with resolution occurring on administration of oral steroids. The patient underwent a magnetic resonance cholangiopancreaticogram as well as a liver biopsy. These demonstrated bilobar intrahepatic bile duct stricturing and ectasia, and portal based mixed inflammation with minimal lobulitis. The cholestasis was responsive both to steroids and ursodeoxycholic acid. Taken together, this indicated a pathology driven by immune checkpoint blockade.
Discussion
This series reports the incidence, clinical features and treatments used for liver irAEs, but also attempts to identify useful biomarkers and how they can be used to predict effective use of steroids.
ICPI therapy results in a variety of autoimmune reactions—ranging from encephalitis (B cell mediated) to colitis (T cell mediated). There is variation both in terms of organ systems affected over time, as well as the intensity of an inflammatory response with repeat dosing. In addition, the autoimmune reaction, once initiated, does not consistently resolve on withdrawal of the drug, so may require longer term immunosuppression.
ICPI hepatitis is an uncommon side-effect,29 which despite interindividual variability, displays distinct histological characteristics to autoimmune hepatitis or drug-induced liver injury.30 31 In this cohort of 21 patients, novel trends can be identified regarding the biochemical patterns of disease.
Although there are as yet no defined predictive factors for developing hepatitis, it appears to be the most common in the cohort receiving simultaneous PD-1 and CTLA-4 blockade. Seventy-five per cent (n=3) of instances of Grade 4 hepatitis were in Ipilimumab-containing regimens. Our data suggest that all patients develop hepatitis within 120 days of starting checkpoint therapy, which could be timed with immunotherapy cycles delivered every 2–3 weeks to check for hepatitis onset.
Within the steroid only treatment cohort, the ALT fell below the treatment threshold of Grade 2 hepatitis (ALT 112) within 20 days in all patient courses except for four—I3, I4, I+N7 and I+N9 (online supplementary file 2). Increased patient numbers are required to verify these trends, but this may represent a cohort of patients that would benefit from escalation of therapy earlier.
In the nine instances where SSAs were employed, the ALT trends over time clustered together irrespective of regimens used, with similar slopes of response times (values falling to half of baseline ALT by 11 days).
The relevance of two patterns of non-response is unclear but may reflect immunological differences as no clinical factors differed between the cohorts.
Although patient numbers are small, data from this cohort suggests that the smaller 50–60 mg OD Prednisolone dose is likely to be sufficient. Treatment escalation should be to an additional SSA rather than an increased dose of steroid if the ALT does not respond rapidly. This may reduce the incidence and/or severity of corticosteroid-related adverse effects in such patients.
Finally, no adverse events were noted with Infliximab use. Some guidelines advocate avoiding infliximab in immune-mediated hepatitis owing to the risk of liver failure (although they concede the evidence for this is lacking).32 Other therapies such as anti-thymocyte globulin, tacrolimus methotrexate, leflunomide and ciclosporin have also been reported to ameliorate immunotherapy-related hepatitis in cases that are steroid-refractory.33–36
We describe one case of a predominantly cholangiopathic pathology that was responsive to steroids and ursodeoxycholic acid.
Abnormal liver biochemistry also occurs in this group of patients due to other causes of liver disease, such as viral hepatitis or sepsis. Liver screens and if necessary, biopsies, should form a key step in the investigation of abnormal blood tests in this cohort of patients.37
Future work should seek to characterise this patient population in more detail. Early and routine liver biopsy, with flow-cytometry or single-cell RNA analysis, may be helpful so that this heterogeneous patient group may be better phenotyped. Clinical parameters are insufficient for predicting outcome (online supplementary file 3), and we require peripheral biomarkers that can predict treatment response more accurately.
Conclusion
Incidence of liver irAEs was 4% in this cohort with ICPI hepatitis occurring within 120 days of the first dose of checkpoint therapy. A subset of patients did not respond to initial therapy with corticosteroids, and additional immunosuppression appears safe and effective. Corticosteroid doses above prednisolone 60 mg daily were not associated with more rapid resolution of liver biochemistry.
References
Footnotes
VC and TG are joint first authors.
Correction notice This article has been corrected since it published Online First. The joint first author statement has been added.
Contributors VC, TG and JFC devised the article. VC, TG, JDC, MP and JFC collected the data. VC and TG analysed the data and drafted the original article. MRM, MP, AS, PK, JDC, OB, VC and JFC were involved in the management of the patients, edited the original article prior to submission and all reviewed and agreed the revised version. VC, TG and JFC wrote the responses to the Editor’s and reviewers’ comments and revised the manuscript. VC and JFC are responsible for the overall content as guarantors.
Funding The research was supported by funds from the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC) and NIHR Research Capability Funding.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests JFC and OB have received speaker fees from BMS. OB has received a research grant from Celgene. MRM has acted as a consultant for Amgen, AstraZeneca, Bristol-Myers Squibb, Eisai, GlaxoSmithKline, Immunocore, Lilly, Merck, Millennium, Novartis, Physiomics, Rigontec and Roche; his institution has received research grants from Abbvie, Amgen, AstraZeneca, Bristol-Myers Squibb, Clovis, Eisai, GlaxoSmithKline, Immunocore, Merck, Millennium, Novartis, Pfizer, Rigontec, Roche and Vertex.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.