Article Text

Abstract
Aim: Recent studies had suggested substantial molecular differences between tumours from different ethnic groups. In this study, the molecular differences between the incidences of colorectal carcinoma in Saudi and Swiss populations are investigated.
Method: 518 cases of colon cancer tumours (114 from Saudi Arabia and 404 from Switzerland) were analysed in a tissue microarray format. Fluorescence in situ hybridisation (FISH) was used to estimate frequencies of copy number changes of known oncogenes, including HER2, TOPO2A, CCND1, EGFR and C-MYC.
Results: Using FISH, amplifications were mostly low level (gene-to-centromere ratio 2 to 4), which is in contrast with other tumour types with more frequent gene amplifications. The amplifications were particularly frequent for MYC (Saudi 9% and Swiss 14.2%) but unrelated to clinical outcome and pathological information. Remarkably, there were four tumours exhibiting classic high-level gene amplification for HER2 (Swiss 1.3%), a pattern often accompanied by response to trastuzumab (Herceptin) in breast cancer. Occasional high-level amplifications were also observed for CCND1 (Saudi 1/106, 0.9%; Swiss 2/373, 0.5%) and EGFR (Swiss 2/355; 0.6%).
Conclusions: Rare high-level amplifications of therapeutic target genes were found in patients with colon cancer. Although no molecular differences were found between incidences of colon cancer cases in Swiss and Saudi populations, these observations emphasise the urgent need for clinical studies investigating the effect of targeted therapies.
- CH, Switzerland
- FISH, Fluorescence in situ hybridisation
- KSA, Kingdom of Saudi Arabia
- TMA, tissue microarray
Statistics from Altmetric.com
- CH, Switzerland
- FISH, Fluorescence in situ hybridisation
- KSA, Kingdom of Saudi Arabia
- TMA, tissue microarray
Almost all information on the molecular features of human malignancies has been derived from patients from Europe and the US. There is, however, growing evidence that these findings may not be applicable to all ethnic groups.1 For example, genetic differences in the pattern of p53 mutations have been reported among Midwest US Caucasian, African-American, Austrian and Japanese patients with breast cancer.2,3
In a recent study, we found notable differences in histological features and gene amplification frequencies of HER2 and C-MYC between Saudi and Swiss patients with breast cancer.4 Notable differences in the lifestyle or variable genetics causing cancer susceptibility were considered as possible explanations. These findings prompted us to expand our project to other major cancer types including colon cancer, for which a considerable geographical variability has mainly been attributed to dietary factors.5–7 For example, the deaths due to colon cancer is ten times lower in Mexico, South America and Africa compared with the US and Europe.8 In the KSA, the incidence of colon cancer is about half as high as in the US, and the peak incidence in Saudi Arabia is at a lower age group (40–60 years in the KSA vs 60–80 years in the US).8
Our study focuses on known oncogenes that can serve as target genes for current or future gene-specific therapies rather than significant genetic hallmarks of colorectal cancers like deleted in colon cancer or microsatellite instability. Knowledge of differences in the prevalence of alterations of such genes is of particular interest because it gives insight into treatment options in different ethnic groups, and might also help to prioritise development of new drugs. Since oncogene amplification is infrequent at least in colon cancer cases in Western countries, high throughput technologies, like the tissue microarray (TMA), are a prerequisite for such analyses.
The aim of this study was to identify potential genetic differences in patients with colon cancer from Western countries and the Middle East, which may accompany or even contribute to the epidemiological differences. For best possible standardisation of the analyses, all samples were included into TMAs. The analyses were limited to amplification detection of five genes (HER2, TOP2A, CCND1, EGFR and C-MYC) by fluorescence in situ hybridisation (FISH).
PATIENTS AND METHODS
Colon cancer TMAs
Two sets of TMAs were made from formalin-fixed (buffered neutral aqueous 4% solution) paraffin-embedded colon cancer tissue were used. Both sets were from consecutive series of colon cancers. The first set consisted of 404 Swiss (CH) tumours from patients with colon cancer collected at the Institute of Clinical Pathology, Basel, Switzerland. The median age of these patients was 69 years. The second TMA consisted of samples from 114 patients with colon cancer from the KSA, collected at the Pathology Department, King Faisal Specialist Hospital & Research Centre, Riyadh, Saudi Arabia. The median age of these patients was 62 years. Table 1 summarises the histopathological data of the TMAs. The ethical committees of the Cantonal Hospital, Basel, Switzerland and the King Faisal Cancer Center, Riyadh, Saudi Arabia, had permitted to use the tissue and the data for this project. Two pathologists (LT, LT) reviewed all Swiss cases of colon cancer, one pathologist (PB) reviewed all Saudi cases of colon cancer to confirm histological diagnosis. Raw survival information was available for 310 Swiss cases with a median follow-up time of 4.2 years. TMA was constructed as described previously.9 Briefly, tissue cylinders with a diameter of 0.6 mm were punched from morphologically representative tumour areas of each “donor” tissue block and brought into one recipient paraffin block using a home-made semi-automated tissue arrayer.
Histopathological data of samples from Saudi and Swiss patients with colon cancer
Fluorescence in situ hybridisation
TMA sections were used for dual labelling fluorescence in situ hybridisation (FISH). A commercial kit was used for proteolytic slide pretreatment (paraffin pretreatment reagent kit, Vysis, Downers Grove, IL, USA). Spectrum-Orange-labelled gene-specific probes were used together with Spectrum-Green-labelled probes for the respective centromere as a reference. The probe combinations were: HER2/centromere 17 (Path Vysion; Vysis), EGFR/centromere 7 (Vysis), CCND1/centromere 11 (Vysis), MYC/centromere 8 (Vysis) and a TOP2A probes/ centromere (Vysis). Before hybridisation, TMA sections were deparaffinised, air dried and dehydrated in 70%, 85% and 100% ethanol followed by denaturation for 5 min at 74°C in 70% formamide-2×standard saline citrate solution. After overnight hybridisation at 37°C in a humidified chamber, slides were washed and counterstained with 0.2 μM DAPI in an antifade solution. Data from our laboratory have previously shown that diagnosis of amplification based on signal number estimation is highly reliable.10 A tumour was considered amplified if the ratio was >2.0. All other tumours were considered non-amplified. Figure 1 gives examples of amplified and non-amplified tumours.

Examples for oncogene amplification in colon cancer cases from Saudi. (A) CCND1, (B) CMYC, (C) TOP2A, (D) EGFR, (E) HER2 and (F) HER2 (normal copy number).
Statistics
Contingency table analysis and χ2 tests were used to study the relationship between FISH results and morphological parameters. A p value of <0.05 was regarded as significant. SAS software (SAS Institute Inc, JMP 5.1 software (Cary, North Carolina, USA)) was used for data analysis.
RESULTS
Histology
Table 1 summarises the histopathological features of Saudi and Swiss cases with colon cancer. Except for a significant difference observed in pN1 patients, a remarkable similarity was reported between both consecutive tumour sets in the pT and histological grade distribution.
FISH, amplification analysis
There were no differences between the tumours of patients from Swiss and Saudi populations in the amplification pattern of all five genes (fig 2). MYC showed by far the highest amplification frequency among the analysed genes. Amplification was reported in 9% Saudi and in 14.2% Swiss patients with colon cancer. Most of these were low-level amplifications with 2–3 centromeres and 5–8 MYC signals per nucleus. Only four tumours had classic high-level amplifications with a MYC/centromere 8 ratio ⩾5. The centromere 8/MYC FISH findings were 1/20, 2/10, 2/20 and 4/40 in these cases.

Amplification frequency of CCND1, CMYC, TOP2A, EGFR and HER2 in colon cancer cases from Saudi Arabia (KSA) and Switzerland (CH).
All other genes showed gene amplification only occasionally (range 1.9–3.9%; fig 2). There were, however, some high-level amplifications seen for each gene in colon carcinomas. For example, among the nine HER2-amplified cases, there were four cases with a HER2/centromere 17 ratio >5.0. The centromere 17/HER2 findings were 2/10, 2/12.5, 2/20 and 2/20 in these cases. Two of these highly HER2-amplified cases had a TOP2A co-amplification, while the two others had a normal TOP2A gene status. Among the 14 EGFR-amplified cases, there was one case with 4 centromere 7 and 100 EGFR signals and another case with 2 centromere 7 and 20 EGFR signals. For CCND1, a ratio of ⩾5.0 was seen in 1 of 11 amplified cases (2 centromere 11, 10 CCND1 signals).
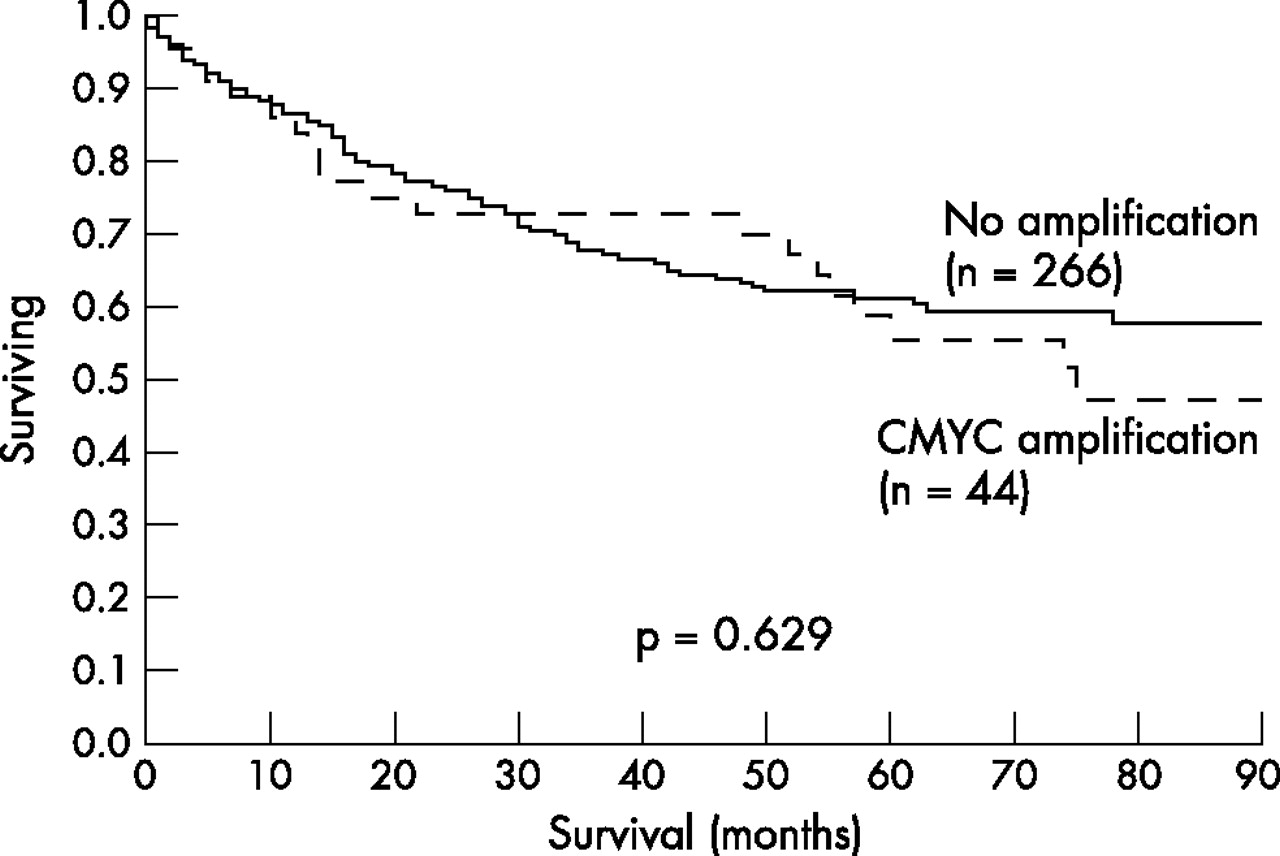
There were no associations between gene amplifications and histological tumour grade or the pT/pN categories (table 1). MYC amplification was unrelated to overall patient survival (fig 3). The impact of the other amplifications on raw survival could not be analysed because of their low amplification frequency.

{kind=link}
{kind=link}
{kind=link}
Lack of prognostic impact of CMYC amplifications in patients with colon cancer (Swiss tumour set).
FISH, technical aspects
The number of interpretable cases only varied slightly between the different FISH probes and between the two colon cancer sets. In the Swiss set, the fractions of non-informative cases were 22% for HER2, 8% for CCND1, 23% for MYC, 12% for EGFR and 19 % for TOP2A. In the Saudi set, the non-informative fractions were 14% for HER2, 7% for CCND1, 22% for MYC, 17% for EGFR and 19.8 % for TOP2A. Reasons for non-informative results were lack of tissue on the TMA, absence of unequivocal tumour cells in the arrayed tissue or insufficient hybridisation. All TMA sections were hybridised only once. The amplification results of interpretable cases already made it very unlikely that the (small) amplification frequency could vary significantly between the two cancer sets. Hence, no attempts were made to increase the number of interpretable cases by additional experiments.
DISCUSSION
Most of the genetic information on colon cancer and other tumours are derived from studying European and US patients. However, increasing evidence suggests that patients with cancer from different ethnic groups exhibit significant molecular differences between them. Differences in the length of EGFR intron 1 account for varying EGFR expression levels between Asian, Caucasian and African-American patients with breast cancer.11 More recently, remarkable differences in the frequency of EGFR exon 18–21 mutations, predictive for response to gefitinib (Iressa; AstraZeneca Pharmaceuticals LP, Wilmington, Delaware, USA), were found between Japanese and US patients with lung cancer.12,13
In the context with other studies comparing colon cancers in patients of Western and Eastern countries, our data also do not provide evidence for major molecular differences. However, differences might be seen with respect to other genetic factors. Obviously, these results do not exclude major genetic ethnic differences for this tumour type, especially since four of five investigated genes showed only rare amplifications.
Only FISH was used in this project in an effort to avoid methodological bias due to differences in tissue handling. Insufficient hybridisation is always recognised in FISH due to the absence of signals, if suboptimal tissue processing interferes with the hybridisation. Regarding immunohistochemical analysis, false negative results cannot occur in FISH analysis, because lack of any signals renders a FISH analysis non-interpretable but not (false) negative. In contrast, by immunohistochemical analysis it is not possible to distinguish a true negative result (absence of the antigen) from a false negative result (loss of immunoreactivity due to suboptimal tissue fixation). However, section thickness, incubation time, data evaluation can all influence FISH results. The definition used for amplification (ratio of gene copy number-to-centromere copy number ⩾2.0) reflects the currently used standard. However, this value was established in breast cancer HER2/neu studies where the majority of amplified cases had ratios >5.0 and where the few cases with a borderline ratio (2 to 4) were too rare to have a major impact on statistical analyses. It is noteworthy that the general amplification pattern in cases with colon cancer is not comparable to HER2 findings in patients with breast cancer. Here, for all genes, most “amplified” cases had ratios ranging between 2.0 and 4.0. This may indicate a much lower genomic instability of colon cancer as compared with breast cancer, and may also suggest a different biological significance of “amplifications” according to the definitions used in this study in colon cancer than in breast cancer.
Using these established criteria, a relevant fraction of MYC amplifications was observed in colon cancer. This is consistent with previous studies describing 48–60% 8q over-representations in studies performing comparative genomic hybridisation,14–16 Southern blot17 and FISH analysis.18 An additional study using the Southern blot method detected low-level amplification in approximately one-third of cases with colon carcinoma.19 Furthermore, these authors reported that amplification of c-myc identified patients with stage II and stage III colon cancer with increased disease-free and overall survival after 5 FU-based therapy. In contrast with previous studies (maximum of 149 patients included),20 our patient set was large enough to investigate the potential clinical significance of MYC amplifications. The absence of associations between MYC amplification and unfavourable pathological or clinical features was disappointing. Previous large-scale amplification analyses had almost always found gene amplification—a hallmark of genomic instability—to be related to unfavourable tumour features—for example, in cases with breast and bladder cancers.21 We hypothesise that the borderline nature of most MYC amplifications may be at least a part of the cause for the absence of associations with tumour phenotype and prognosis.
Other amplifications known to occur frequently in other tumour types were occasionally observed in our population with colon cancer. This, for example, applies to HER2 amplification, a molecular hallmark and therapeutic target in breast cancer.22 Although most HER2 amplifications were of borderline nature, a few cases (4 of 404, CH dataset) were with classic high-level amplifications exactly as seen in HER2-responsive breast cancers. Similar to breast cancer, TOP2A co-amplifications were observed in a fraction of HER2-amplified colon cancers. In the case of breast cancer, it was suggested that HER2/TOP2A co-amplified cancers would be particularly sensitive to anthracyclins directly targeting the TOP2A protein. It would be interesting to see whether such a treatment response could also be predicted in TOP2A-amplified colon cancers.
Other than HER2, EGFR is an established therapeutic target in colon cancer. Cetuximab, a human/murine chimeric monoclonal antibody against EGFR, has shown partial response in 9% and minor response in 36% of patients with advanced colorectal cancer.23 Although overexpression of EGFR is requested for Cetuximab indication, no association has so far been observed between the EGFR expression level and response to Cetuximab therapy. Our results do not suggest a role of amplification analysis for Cetuximab response prediction, as the number of amplified cases was much lower than the potentially responding population. However, the finding of two cases with a very high level EGFR amplification—one with 100 EGFR gene copies per cell—is intriguing. It could be speculated that these two tumours could have reacted exceedingly well to Cetuximab or potentially also to other anti-EGFR therapies.
In summary, the large number of tumours included in this study highlights the presence of rare events with molecular features of potential therapeutic relevance. However, our data does not suggest major molecular differences between the incidences of colorectal cancer in Saudi and Swiss populations. In the era of targeted tumour therapies, these observations emphasise the urgent need for clinical studies to investigate the effect of targeted therapies with an established patient benefit in one tumour type and also in other tumours with similar molecular features.
Take-home messages
-
Using the tissue microarray technique, we investigated molecular differences between the incidences of colorectal carcinoma in Saudi and Swiss populations by fluorescence in situ hybridisation analysis to estimate frequencies of copy number changes of known oncogenes like HER2, TOPO2A, CCND1, EGFR and C-MYC.
-
Amplifications were mostly low level (gene-to-centromere ratio 2 to 4) and were particularly frequent for MYC but unrelated to clinical outcome and pathological information.
-
Rare high-level amplifications of HER2 were found in cases with colon cancer in a pattern similar to patients with breast cancer, which is often accompanied by response to trastuzumab (Herceptin).
-
Although no molecular differences were found between the incidences of colorectal cancers in Swiss and Saudi populations, these observations emphasise the urgent need for clinical studies investigating the effect of targeted therapies.
Acknowledgments
We thank Valerie Atizado for her assistance in tissue micro array construction of colorectal carcinomas in Saudi population.
REFERENCES
Footnotes
-
Published Online First 2 August 2006
-
Funding: This research was funded by the Schweizerischen Arbeitsgemeinschaft für klinische Krebsforschung (SAKK; to CT).
-
Competing interests: None declared.