Article Text

Abstract
Background Patients with rare cancers represent 55% of all gynecological malignancies and have poor survival outcomes due to limited treatment options. Combination immunotherapy with the anti-programmed cell death protein 1 (anti-PD-1) antibody nivolumab and the anti-cytotoxic T-lymphocyte-associated protein 4 (anti-CTLA-4) antibody ipilimumab has demonstrated significant clinical efficacy across a range of common malignancies, justifying evaluation of this combination in rare gynecological cancers.
Methods This multicenter phase II study enrolled 43 patients with advanced rare gynecological cancers. Patients received induction treatment with nivolumab and ipilimumab at a dose of 3 mg/kg and 1 mg/kg, respectively, every 3 weeks for four doses. Treatment was continued with nivolumab monotherapy at 3 mg/kg every 2 weeks until disease progression or a maximum of 2 years. The primary endpoint was the proportion of patients with disease control at week 12 (complete response, partial response or stable disease (SD) by Response Evaluation Criteria In Solid Tumor V.1.1). Exploratory evaluations correlated clinical outcomes with tumor programmed death-ligand 1 (PD-L1) expression and tumor mutational burden (TMB).
Results The objective response rate in the radiologically evaluable population was 36% (12/33 patients) and in the intention-to-treat population was 28% (12/43 patients), with additional 7 patients obtaining SD leading to a disease control rate of 58% and 44%, respectively. Durable responses were seen across a range of tumor histologies. Thirty-one (72%) patients experienced an immune-related adverse event (irAE) with a grade 3/4 irAE observed in seven (16%) patients. Response rate was higher among those patients with baseline PD-L1 expression (≥1% on tumor cells) but was independent of TMB.
Conclusions Ipilimumab and nivolumab combination treatment has significant clinical activity with a favorable safety profile across a range of advanced rare gynecological malignancies and warrants further investigation in these tumor types.
- CTLA-4 antigen
- programmed cell death 1 receptor
- immunotherapy
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified participant data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Up to 55% of gynecological cancers are considered rare and despite the high collective occurrence, the low incidence rate of individual rare cancer types makes research in these cancers challenging.1 Accordingly, patients have very limited treatment options as clinical guidance is frequently based on small institutional case series or anecdotal evidence and overall an inferior survival rate compared with patients with common malignancies.2
Immunotherapy using monoclonal antibodies that block negative regulators of T-cell activation such as programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) leads to stimulation and/or reinvigoration of tumor-specific T-cell responses.3 Immune-stimulatory antibodies have demonstrated significant clinical activity in a range of malignancies; however, single-agent anti-PD-1/programmed death-ligand 1 (PD-L1) treatment has shown only limited activity in patients with common gynecological malignancies, such as high-grade serous ovarian cancer or uterine endometrioid carcinoma4 5 with the exception of microsatellite unstable (MSI-H) endometrial cancer.6 Anti-PD-1/PD-L1 and anti-CTLA-4 blockade have distinct and complementary features and combined anti-PD-1/CTLA-4 blockade has demonstrated superiority compared with single-agent anti-PD-1 therapy across a range of malignancies.7–9
CA 209-538 was a multicenter multicohort phase II trial that investigated combination immunotherapy with the anti-PD-1 antibody nivolumab and the anti-CTLA-4 antibody ipilimumab in patients with rare cancers.10–12 The trial included a cohort of patients with advanced gynecological malignancies. Accompanying translational research aimed to identify tumor-agnostic biomarkers.
Methods: patients
Study design, patients and treatment
CA 209-538 was a multicenter open-label phase II study conducted at five Australia sites (Austin Health, Peter MacCallum Cancer Centre, Monash Health, Melbourne, Blacktown Hospital, Sydney, Border Medical Oncology, Albury). Eligible patients for the gynecological cohort were aged 18 years or older and had a histologically confirmed metastatic rare cancer of the female genital tract. Patients with high-grade serous ovarian carcinoma, uterine endometrioid adenocarcinoma and cervical cancer (adenocarcinoma and squamous cell carcinoma) were excluded. Patients had at least one measurable lesion according to Response Evaluation Criteria In Solid Tumor (RECIST) V.1.113 and an Eastern Cooperative Oncology Group performance status of 0 or 1. Other inclusion criteria were a life expectancy of 3 months or more and adequate organ function. Patients could either be treatment naive or had received prior systemic therapy with a minimum washout period of 28 days before initiation of study treatment. Disease progression under prior therapy was not an inclusion criterion. Key exclusion criteria were active brain metastases and a history of autoimmune conditions. Archival tumor tissue, or a fresh tumor biopsy during screening, was required for predictive biomarker analysis.
Nivolumab and ipilimumab were administered intravenously at a dose of 3 mg/kg over a period of 60 min and 1 mg/kg over a period of 90 min, respectively, every 3 weeks for four doses (induction phase), followed by nivolumab monotherapy at a dose of 3 mg/kg every 2 weeks (maintenance phase) until disease progression or a maximum of 2 years after enrolment. Dose reductions were not permitted; however, study treatment could be interrupted to enable recovery from adverse reactions for up to 6 weeks. If treatment was discontinued, patients were followed up until disease progression or initiation of a different treatment.
Tumor assessments were performed by radiological assessment (CT scan of the brain, chest, abdomen and pelvis) at baseline and then every 12 weeks during treatment or follow-up. A confirmatory scan was performed 6 weeks after the first restaging scan at week 18. Tumor response was assessed according to RECIST V.1.1.13
Patients with evidence of progressive disease at their first restaging scan at week 12 were permitted to continue on study treatment at the discretion of the investigator for another 6 weeks until radiological confirmation of progression at week 18.
Safety analyses were performed on all patients who received at least one dose of study treatment. Laboratory monitoring and safety assessments were performed at baseline and every two to 3 weeks prior to treatment according to the study protocol. Adverse events were graded in accordance with the NCI Common Terminology Criteria for Adverse Events V.4.0 and collected during treatment and for 100 days after the last dose received.
Study endpoints
The primary endpoint was the proportion of patients with disease control at week 12 (complete response, partial response or stable disease (SD)) according to RECIST criteria. The secondary objective was identification of a tumor-agonistic biomarker.
Biomarker analysis
Archival formalin-fixed paraffin-embedded tumor tissue was tested for PD-L1 expression by immunohistochemistry (IHC). The antibody used was Ventana PD-L1 (SP263) according to the ULTRA VENTANA PD-L1 (SP263) Assay (Roche diagnostics). A tumor was deemed PD-L1 positive if at least 1% of tumor cells expressed PD-L1. DNA was extracted from tumor tissue for gene sequencing and the tumor mutational burden (TMB) was determined by the Oncomine tumor mutation load assay (Thermo Fisher Scientific). Additional archival formalin-fixed paraffin-embedded tumor tissue from two patients with hypermutated tumors was tested for CD3 (SP7, ab16669, Abcam), CD4 (EPR6855, ab133616, Abcam), CD8 (C8/144B, MA5-13473, Invitrogen), CD19 (EPR5906, ab134114, Abcam), CD68 (PG-M1, MA5-12407, Invitrogen), granzyme B (D6E9W, 46890, Cell Signalling), FOXP3 (36A/E7, ab20034, Abcam), MHC class I (in-house), PD-L1 (E1L3N, 13684, Cell Signalling) and panCK (Akoya Biosciences) expression by multispectral IHC. Briefly, slides were baked at 65°C for 2 hours, dewaxed in xylene three times for 10 min, rehydrated in ethanol twice for 10 min and manually stained. The staining included initial blocking of endogenous peroxidases using 3% hydrogen peroxide for 30 min, followed by sequential 15 min rounds of heat-induced epitope retrieval (microwave at 20% power), 10 min blocking of non-specific binding sites, 30 min primary and 10 min secondary (anti-mouse and anti-rabbit horseradish peroxidase) antibody incubation and 10 min fluorophore-tyramide signal amplification using Opal 520, 540, 570, 620, 650 and 690 fluorophores (Akoya Biosciences) labeling target proteins, respectively. Slides were counterstained with spectral DAPI and scanned using the Vectra 3 Automated Quantitative Pathology Imaging System (Akoya Biosciences). Images were spectrally unmixed and analyzed using inForm Cell Analysis software (Akoya Biosciences). Tissue specimens were segmented into tissue and stroma areas and cell phenotyping was performed on at least 10 regions of interest per tissue specimen to quantify the number of total CD3+ T cells, CD4+FOXP3+ regulatory T cells and panCK+MHC class I+ cells, which are shown per 1000 cells.
Statistical analysis
Given the heterogeneous nature of the patient population, statistics were descriptive and no sample size calculation was undertaken. Descriptive statistics (median, CIs) were performed using GraphPad Prism V.8.3.0 software.
Fisher’s exact test was used to assess any association between response and PD-L1 expression and between response and TMB.
Results
Patient population and treatment
Forty-three patients were enrolled into the gynecological cohort and received at least one dose of ipilimumab and nivolumab. The disease characteristics of the study population are outlined in table 1. Apart from one patient, all had received prior systemic therapy with 51% of patients having received at least two lines of prior systemic treatment prior to enrolment into the trial. Ten tumor types were represented with the most common being uterine serous carcinoma, ovarian clear cell carcinoma, uterine leiomyosarcoma and ovarian carcinosarcoma (table 1). Only one patient (uterine carcinosarcoma) had a tumor with a MSI-H phenotype.
Patient demographics and tumor types
Overall, 20 of 43 (47 %) patients were alive at the time of data analysis (November 2020), with a median follow-up of 16.8 months.
Overall, 30 (70%) patients completed the induction treatment with four doses of nivolumab and ipilimumab, 10 (23%) patients progressed clinically during the induction phase with the majority receiving only one or two treatment doses respectively. Three (7%) patients discontinued treatment during the induction period due to high-grade immune-related adverse events (irAEs). One of the patients was subsequently switched to single-agent nivolumab therapy and two patients came off study after resolution of their irAE due to disease progression at their first restaging. Out of the 30 patients who completed induction treatment, 20 patients entered into the maintenance phase with fortnightly nivolumab infusions and 10 patients came off study for progressive disease at their first radiological assessment at week 12.
Efficacy
The objective response rate of the radiologically evaluable population was 36% (12 out of 33 patients) and 28% (12 out of 43 patients) in the intention-to-treat population (table 2, figure 1A).

(A) Waterfall plot of the best objective response measured as the maximum change from baseline in the sum of the longest diameter of each target lesion. Thirty-three patients with at least one radiological evaluation after treatment are shown. Bars marked (progressive disease (PD)) represents patients with new metastatic lesions at their first radiological evaluation. (B) Time to response and duration of study treatment. Thirty-three patients were undergoing at least one radiological assessment. Six patients had an ongoing response at the time of data analysis.
Response to study treatment
Additional seven patients had SD leading to a disease control rate of 58% and 44%, respectively. Ten patients (23%) progressed rapidly prior to the first restaging scan and were taken off study. Overall, 6 out of the 12 confirmed responses were ongoing at the time of data cutoff (range, 6–24+ months) (figure 1B). Fourteen (33%) patients had progressive disease at their first restaging scan at week 12 with four patients continuing treatment beyond initial progression. None of these patients subsequently achieved a treatment response. Durable responses were observed across a range of tumor types including uterine leiomyosarcoma, uterine and ovarian clear cell carcinoma, uterine and ovarian carcinosarcoma, vaginal carcinoma and low-grade serous ovarian carcinoma. The median progression-free and overall survival for the entire cohort were 2.8 months (95% CI: 2.6 to 6.7) and 15.8 months (95% CI: 5.8 to 19.1), respectively (figure 2).

Kaplan-Meier curve of overall survival (A) and progression-free survival (B) for the entire cohort.
Three of the five patients (60%) with uterine leiomyosarcoma had an objective response (two complete and one partial remissions) with the remaining two patients having SD as their best response to study treatment (figure 3). Three of the nine patients with uterine and ovarian carcinosarcoma demonstrated a partial response with an additional two patients having SD. Of the six patients with ovarian clear cell carcinoma, two patients had an objective response including one patient with a complete remission that is ongoing at nearly 2 years. In contrast, only one of the eight patients with uterine serous carcinoma obtained a response which was short lived (table 2).

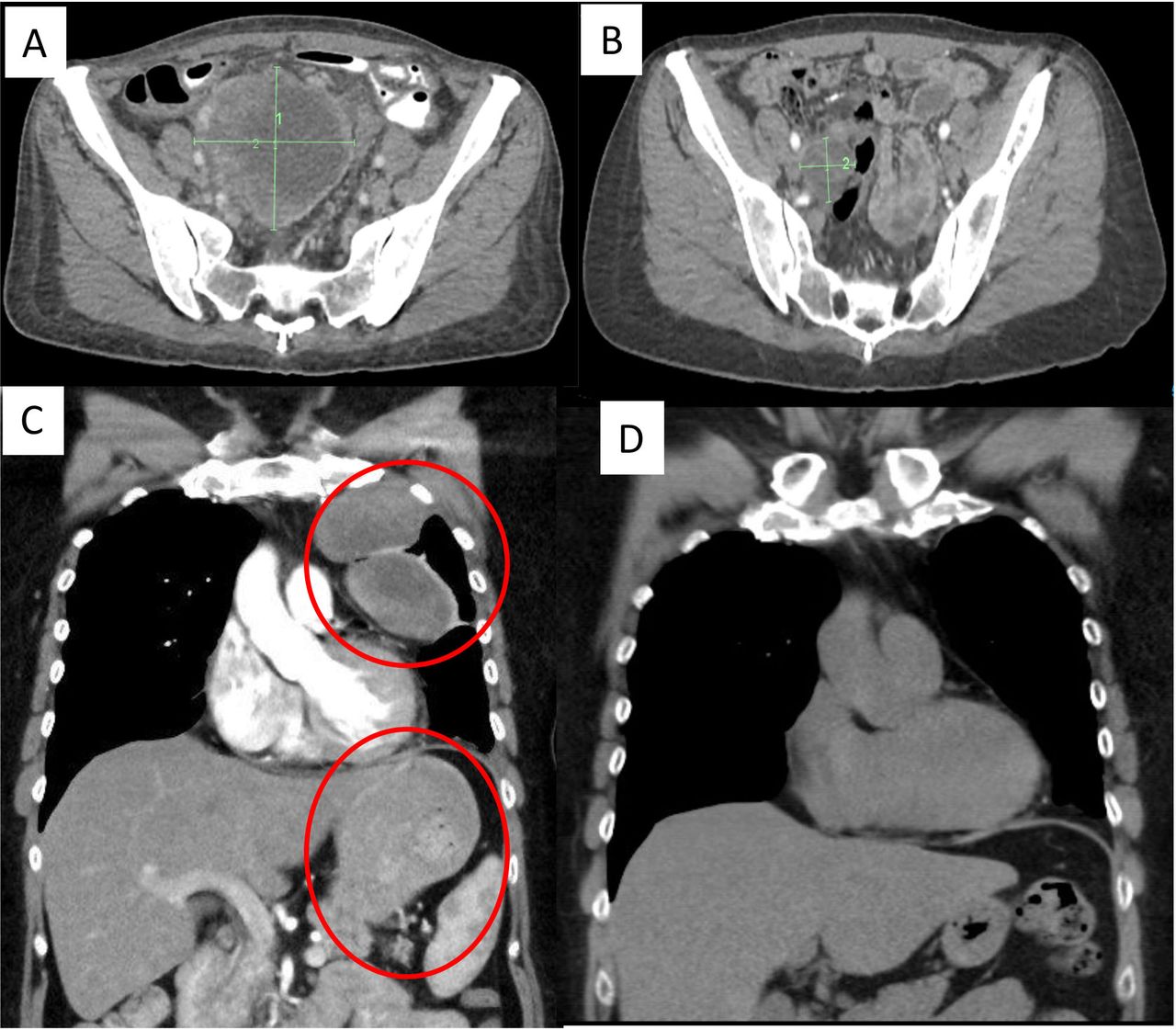
(A,B) Pretreatment and on-treatment CT scan of a patient with metastatic uterine leiomyosarcoma who progressed on first-line chemotherapy with docetaxel and gemcitabine and obtained a partial response at the first restaging CT scan at week 12. All metastases completely regressed under trial treatment with a residual subcentimeter pulmonary lesion being not fludeoxyglucose (FDG) avid. The response is ongoing close to 2 years after commencement of therapy. (C,D) Pretreatment and on-treatment CT scan of a patient with metastatic uterine leiomyosarcoma who progressed on first-line chemotherapy with doxorubicin and obtained a durable partial remission under trial treatment. The patient discontinued study treatment at the start of her maintenance phase due to recurrent pneumonitis. The patient’s partial remission lasted for a year with ongoing reduction of target lesions despite discontinuation of study treatment. (Circles mark the sites of pleural and peritoneal metastases.)
Safety
Overall, 31 (72%) of the 43 patients experienced immune-related adverse events of any grade (table 3) with grade 3 or higher immune-related toxicity occurring in 7 (16%) patients.
Frequency of Immune-related adverse events
Treatment-related adverse events led to treatment discontinuation in four (9%) patients. There were no treatment-related deaths.
Biomarker analysis
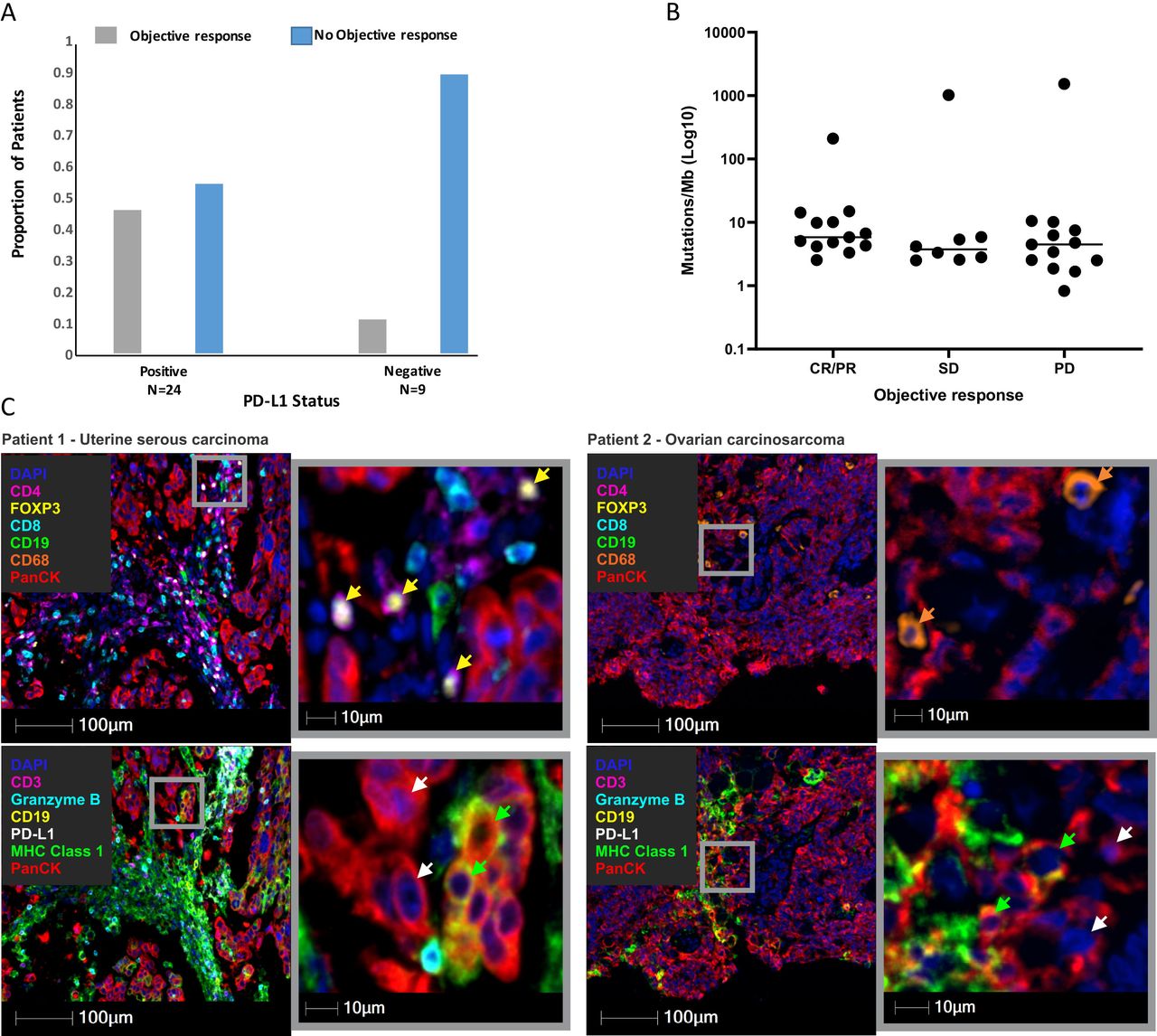
Thirty-three patients underwent at least one restaging scan and had tumor tissue available for PD-L1 IHC. Positive staining of at least 1% of PD-L1 expression on tumor cells was found in 24 (73%) patients, 11 (46%) of whom had an objective response. Of nine patients with PD-L1 negative tumors, only one (11%) obtained a treatment response (figure 4A). Tumor DNA sequencing to assess the TMB was also performed on tumors of all 33 patients. The vast majority of these tumors had a TMB of less than 10/megabase (MB) and the median TMB was not different between patients obtaining an objective response versus SD or disease progression (figure 4B). Three tumors had a very high TMB (range, 211–1535/MB) in keeping with a hypermutated tumor phenotype. Only one of these patients, who had an MSI-H uterine carcinosarcoma, obtained a durable response to study treatment. The underlying mechanism of hypermutation in the remaining two tumors (ovarian carcinosarcoma and uterine serous carcinoma) could not be determined; both demonstrated a mismatch repair proficient phenotype and genomic sequencing showed no mutations in DNA polymerase epsilon/delta genes. The tumor tissue of the hypermutated uterine serous carcinoma (TMB 1535/MB) was heavily infiltrated by CD3+ T cells which was accompanied by a loss MHC-I class expression on panCK+ tumor cells and infiltration of CD4+FOXP3 regulatory T cells (figure 4C on left). In contrast, the hypermutated ovarian carcinosarcoma (TMB 1022/MB) demonstrated only low-level T-cell infiltration (data not shown) along with an increased frequency of CD68+ macrophages (figure 4C on right).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Tumor cell-surface expression of PD-L1 was significantly correlated with an objective clinical response. (B) Tumor mutational burden in patients according to radiological response (complete response/partial response, stable disease versus those with progressive disease). (C) Immunofluorescence of two patients (patient with uterine serous carcinoma on left, patient with ovarian carcinosarcoma on right) with hypermutated tumors that lacked a treatment response. Representative regions of interest showing anti-CD4 (magenta), anti-FOXP3 (yellow), anti-CD8 (cyan), anti-CD19 (green), anti-CD68 (orange) and anti-panCK (red) antibodies with DAPI (blue) counterstain (upper panels), and anti-CD3 (magenta), anti-granzyme B (cyan), anti-CD19 (yellow), anti-PD-L1 (white), anti-MHC class I (green) and anti-panCK (red) antibodies with DAPI (blue) counterstain (lower panels). Arrows highlight CD4+FOXP3+ regulatory T cells (yellow arrows in upper left panel), panCK+MHC class I+ cancer cells (green arrows in lower panels), panCK+MHC class I negative cancer cells (white arrows in lower panels) and CD68+ macrophages (orange arrows in upper right panel). All images were taken at 20× magnification, and scale bars indicate 100 µm or 10 µm (magnified regions of interest). PD-L1, programmed death ligand 1; SD, stable disease; CR, complete response; PR, partial response.
Discussion
Patients with rare cancer represent a significant proportion of all gynecological cancer diagnoses yet have very limited treatment options. This results in inferior survival compared with patients with common malignancies.2 Therapeutic advances are therefore urgently needed in this patient population. We demonstrate here that combination immunotherapy with the anti-PD-1 antibody nivolumab and the anti-CTLA-4 antibody ipilimumab has significant clinical activity across a range of rare gynecological cancers.
Our trial cohort included five patients with metastatic uterine leiomyosarcoma in which chemotherapy has only modest activity and leads to short-lived responses.14 Remarkably, two of our patients with leiomyosarcoma obtained complete remissions which are ongoing and one patient achieved a major partial response that lasted for more than a year in the absence of ongoing treatment as the patient had to discontinue study treatment for recurrent pneumonitis. Our observations contrast with the lack of activity using anti-PD-1 monotherapy with nivolumab15 suggesting that the addition of anti-CTLA-4 blockade is required in advanced uterine leiomyosarcoma to generate an effective antitumor response.
Similarly, patients with advanced uterine and ovarian carcinosarcoma show low response rates to chemotherapy and overall have a poor prognosis.16 Three out of nine patients with carcinosarcoma in our trial demonstrated durable responses to immunotherapy. A significant percentage of uterine carcinosarcomas shows mismatch repair protein (MMRP) deficiency/microsatellite instability which is associated with response to single-agent anti-PD-1/PD-L1 therapy.6 17 In keeping with these findings, one of our patients had a tumor with MLH-1/PMS-2 loss and an ongoing treatment response; the remaining two responders however had mismatch repair proficient tumors suggesting that combination immunotherapy should be further investigated in this patient group independently of MMRP status.
The observation that two of the six patients with ovarian clear cell carcinoma responded to study treatment adds to the emerging evidence that clear cell carcinoma is the subtype of ovarian epithelial cancer with the highest sensitivity to anti-PD-1-based immunotherapy4 18 and future trials will be required to determine if combined anti-CTLA-4/PD-1 blockade is superior to single-agent anti-PD-1 therapy19
In keeping with recent observations, a patient with vaginal squamous cell carcinoma obtained a complete response to study treatment lasting close to 2 years.20 Additional responses were observed in patients with low-grade serous ovarian carcinoma and uterine clear cell carcinoma, malignancies that have so far not been reported to be responsive to immunotherapy.
Very limited activity was seen in our trial in patients with uterine serous carcinoma which contrasts with the significant clinical efficacy that has been observed in this tumor type with lenvatinib and pembrolizumab combination therapy21 suggesting that concomitant antiangiogenic treatment is required in serous carcinoma to overcome resistance to immunotherapy using anti-PD-1 blockade.
We also report here the first treatment experience with immunotherapy using checkpoint inhibition in patients with ovarian sex cord stromal tumors.22 We observed no treatment response in four patients with granulosa cell or Leydig-Sertoli cell tumors although one patient with a granulosa cell tumor obtained a mixed response with a 30% reduction in target lesions.
Ten patients rapidly progressed after enrolment into the trial and received only one or two treatment doses which likely reflects the aggressive biology of many of these malignancies when advanced and the delayed response kinetics of immunotherapy. However, a negative impact of checkpoint inhibition by stimulating tumor growth in this patient population (as it has been reported in other malignancies) cannot be fully excluded.23
High-grade irAEs were only observed in 16% of patients which is lower than observed in other trials using the same dosing regimen,8 9 likely due to the limited drug exposure of the subgroup of patients who progressed rapidly after enrolment into the trial.
The low incidence of each individual rare tumor type makes it very difficult to conduct clinical trials for each rare cancer histological subtype and we therefore thought to identify a tumor agnostic biomarker that could predict a treatment response in this trial cohort. TMB and PD-L1 expression on tumor cells have previously been shown to predict responses to anti-PD-1/PD-L1 blockade in several tumor types.24 There is currently only limited evidence for the predicative power of these markers in patients treated with combined anti-PD-1/CTLA-4 blockade.25 The tumor types that were included in our trial had overall a low TMB which is in keeping with previous analyses.26 Therefore, not surprisingly TMB had no discriminatory power in our trial cohort. Three patients had tumors with a very high TMB which is generally associated with high immunogenicity by generation of an increased number of neoepitopes but surprisingly, only one of the three patients with a hypermutated tumor responded to study treatment. An analysis of baseline tumor tissue of the two non-responding patients suggests different mechanisms of primary resistance with one tumor showing only minor immune cell infiltration, while the other tumor was heavily infiltrated by CD8 T cells. Although both showed a concomitant loss of MHC-I class expression on tumor cells, the latter also showed an abundant infiltration of regulatory T cells in keeping with immune evasion by tumor intrinsic and extrinsic mechanisms. Our observations highlight that interrogation of tumor tissue can uncover underlying mechanisms of treatment failure and should allow for personalized treatment approaches to overcome resistance to checkpoint blockade.27
PD-L1 IHC enriched for treatment response with a four times higher response rate in patients with PD-L1-positive tumors, a finding that is in keeping with observations in patients with non-small cell lung cancer,25 metastatic bladder cancer28 and gastroesophageal cancer29 who were treated with nivolumab and ipilimumab combination immunotherapy.
Overall, our trial demonstrates significant clinical efficacy of nivolumab and ipilimumab combination immunotherapy with a favorable safety profile across a range of rare gynecological cancers. The majority of patients with durable responses had tumors with a low TMB highlighting that TMB has no predictive value in a pan-cancer cohort that is treated with anti-PD-1/CTLA-4 combination immunotherapy. Expression of PD-L1 on tumor cells as measured by IHC may however enrich for responders and should be further evaluated in this setting.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified participant data.
Ethics statements
Patient consent for publication
Ethics approval
The clinical trial protocol was reviewed and approved by the Institutional Review Board at Austin Health (Melbourne, Australia) and was undertaken in accordance with the Declaration of Helsinki and the guidelines of Good Clinical Practice.
References
Footnotes
Twitter @JessDGDuarte, @LukeTQuigley
Contributors Conception and design: OK, JP, AB and JC. Acquisition of data and writing and review of the manuscript: OK, DK, BG, BM, JdGD, LQ, LJ, RL, AS, LM, JP, MC, AB and JC. Analysis and interpretation of data: OK, JdGD, LJ, AB, JP and JC.
Funding The study received funding and drug support from Bristol Myers Squibb. Funding support was also provided in part by a grant from the Commonwealth of Australia, Department of Health Accelerated Research Program. AB was supported by a fellowship from the Department of Health and Human Services acting through the Victorian Cancer Agency. JdGD was supported by Cure Cancer Australia through the Cancer Australia Priority-driven Cancer Research Scheme (grant 1187815).
Competing interests JC reports honoraria/advisory board fees from Bristol Myers Squibb, Amgen, Novartis and MSD and speaker fees from Roche. OK reports speaker fees from Bristol Myers Squibb and MSD and travel support from Bristol Myers Squibb. DK reports honoraria/advisory board fees from Novartis and travel support from Bristol Myers Squibb. MC reports honoraria/advisory board fees from Bristol Myers Squibb, Amgen, Novartis, MSD, Roche, Pierre Fabre, Ideaya, Sanofi, Merck and Nektar. BM reports honoraria/advisory board fees from Novartis and Amgen.
Provenance and peer review Not commissioned; externally peer reviewed.