Article Text

Abstract
Background An elevated peripheral blood derived neutrophil-to-lymphocyte ratio (dNLR) is a negative prognostic marker for patients with non-small cell lung cancer (NSCLC) receiving chemotherapy and immune checkpoint inhibitors. Whether dNLR is also associated with clinical outcomes to first-line pembrolizumab among patients with NSCLC and a programmed cell death ligand 1 (PD-L1) Tumor Proportion Score (TPS) of ≥50% is uncertain. How dNLR relates to the tumor immune microenvironment is also unclear.
Methods In two participating academic centers, we retrospectively analyzed the dNLR (defined as the absolute neutrophil count/white cell count – absolute neutrophil count) prior to initiation of first-line pembrolizumab in patients with metastatic NSCLC and a PD-L1 TPS ≥50% and lacking genomic alterations in EGFR and ALK. An unbiased recursive partitioning algorithm was used to investigate an optimal dNLR cut-off with respect to objective response rate (ORR). Multiplexed immunofluorescence for CD8+, FOXP3+, PD-1+, and PD-L1 was performed on a separate cohort of NSCLCs to determine the immunophenotype associated with dNLR.
Results A total of 221 patients treated with first-line pembrolizumab were included in this study. The optimal dNLR cut-off to differentiate treatment responders from non-responders was 2.6. Compared with patients with a dNLR ≥2.6 (n=97), patients with dNLR <2.6 (n=124) had a significantly higher ORR (52.4% vs 24.7%, p<0.001), a significantly longer median progression-free survival (mPFS 10.4 vs 3.4 months, HR 0.48, 95% CI 0.35 to 0.66, p<0.001), and a significantly longer median overall survival (mOS 36.6 vs 9.8 months, HR 0.34, 95% CI 0.23 to 0.49, p<0.001). After adjusting for age, sex, tobacco use, performance status, histology, serum albumin level, oncogenic driver status, and PD-L1 distribution (50%–89% vs ≥90%), a dNLR <2.6 was confirmed to be an independent predictor of longer mPFS (HR 0.47, 95% CI 0.33 to 0.67, p<0.001) and mOS (HR 0.32, 95% CI 0.21 to 0.49, p<0.001). Among advanced NSCLC samples with a PD-L1 TPS of ≥50%, those with a dNLR <2.6 had significantly higher numbers of tumor-associated CD8+, FOXP3+, PD-1 +immune cells, and PD-1 +CD8+T cells than those with a dNLR ≥2.6.
Conclusions Among patients with NSCLC and a PD-L1 TPS ≥50%, a low dNLR has a distinct immune tumor microenvironment and more favorable outcomes to first-line pembrolizumab.
- derived neutrophil-to-lymphocyte ratio
- PD-L1 TPS ≥50%
- pembrolizumab
- multiplexed immunofluorescence
- and non-small cell lung cancer
Data availability statement
Data are available on reasonable request. The data that support the finding of our study are available on request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- derived neutrophil-to-lymphocyte ratio
- PD-L1 TPS ≥50%
- pembrolizumab
- multiplexed immunofluorescence
- and non-small cell lung cancer
Background
Neutrophils are the most abundant myeloid-derived leukocytes in the peripheral blood with a critical role in innate immunity after infection or injury.1 In cancer, neutrophils play a key function as a regulatory component in the tumor microenvironment (TME), promoting stromal remodeling, metastasis, angiogenesis, thrombosis, and impairment of T-cell-dependent anti-tumor immunity.2 3 To date, most clinical data on the role of neutrophils in cancer have come from analyses of peripheral blood neutrophils rather than intratumoral (IT) neutrophils.4 5 Moreover, neutrophils accumulate in the peripheral blood, and a high neutrophil-to-lymphocyte ratio (NLR) is associated with poorer survival and a lower probability of response to immunotherapy in the advanced setting for various cancers.6–9
Immune evasion is a crucial process involved in cancer development. The mechanistic basis for immune escape is thought to occur through an increase in immunosuppressive molecules, such as programmed cell death ligand 1 (PD-L1), and an enrichment of immunosuppressive cells, including regulatory T cells,10 myeloid-derived suppressor cells,11 and tumor-associated neutrophils.3 Notably, recent evidence suggests that a low neutrophil cellular content in tumors may result in enhanced interferon-gamma T-cell signaling, increased CD8 +cytotoxic T cells, and improved efficacy of anti-PD(L)1 immune checkpoint inhibitors (ICIs) in non-small cell lung cancer (NSCLC).5 Whether NLR is a surrogate to identify a higher degree of infiltration of myeloid cells or correlates with diminished lymphocytes in the TME remains unknown.
In NSCLC, a baseline derived NLR (dNLR, defined as the absolute neutrophil count/white cell count – absolute neutrophil count) is associated with prognosis irrespective of treatment modality for patients with metastatic disease.12 13 An exploratory retrospective analysis on 3987 patients from pooled clinical trials showed that a baseline dNLR ≥3 was independently associated with impaired progression-free survival (PFS) and overall survival (OS) to second-line immunotherapy.13 Currently, little is known about the impact of dNLR on first-line immunotherapy efficacy in advanced NSCLC. In addition, with multiple approved first-line immunotherapy +/−chemotherapy regimens for patients with advanced NSCLC,14–19 the identification of easily determined, accessible biomarkers beyond PD-L1 Tumor Proportion Score (TPS) is needed to determine which patients may be less likely to respond to anti-PD-(L)1 monotherapy.
To determine whether dNLR influences immunotherapy efficacy in treatment-naïve patients with NSCLC and a PD-L1 TPS of ≥50%, we assessed the impact of the pretreatment dNLR on clinical outcomes to pembrolizumab, and examined the relationship between dNLR and tumor immunophenotype in NSCLC.
Methods
Study population
We retrospectively analyzed data from two participating academic centers: the Dana-Farber Cancer Institute (DFCI) and the Massachusetts General Hospital (MGH). Patients were included if they had consented to institutional review board-approved medical record review protocols at each institution and had advanced NSCLC without EGFR mutations or ALK rearrangements and a PD-L1 TPS of ≥50%. Patients were eligible if they received at least one dose of commercial pembrolizumab monotherapy in the first-line setting. Patients who had previously received cytotoxic chemotherapy and/or radiation therapy for early-stage NSCLC were eligible if they had completed prior therapy ≥6 months before the start of pembrolizumab. Patients were excluded if they had a concurrent hematological malignancy, untreated HIV infection, or recent infection, antibiotic use, or corticosteroid administration within 7 days prior to the blood draw used to assess dNLR.
The most proximal complete blood count (CBC) with differential and serum albumin levels obtained prior to pembrolizumab initiation (up to 30 days before the first treatment) and prior to cycle 2 were extracted from electronic medical records. We obtained data for an additional cohort of patients treated at the DFCI for validation of the continuous nature of dNLR analyzed in the primary cohort, including patients treated with immune checkpoints inhibitors in the second-line and beyond. The patient studies were conducted under the ethical guidelines of the Declaration of Helsinki.
The CBC and white cell differential was abstracted at the time of tumor biopsy.
Statistical analysis
Clinicopathological data and immunotherapy response data were abstracted from the electronic medical record. The objective response rate (ORR) and PFS were determined by blinded radiology (DFCI cohort) and investigator (MGH cohort) review using Response Evaluation Criteria In Solid Tumors, V.1.1. PFS was defined as the time from pembrolizumab start to progression or death, and for those without progression, censoring was done at the time of the last disease assessment scan showing no progression. OS was calculated from the time of pembrolizumab start to death. Patients who were still alive at the time of data analysis were censored at the date of last contact. Event-time distributions were estimated using the Kaplan-Meier method and compared with the log-rank test. All p values are two sided and CIs are at the 95% level. Linear correlations were evaluated using Spearman’s test, and categorical variables were evaluated using Fisher’s exact test. An unbiased recursive partitioning algorithm was used to investigate an optimal grouping of dNLR with respect to the ORR to first-line pembrolizumab, using the partykit function in R. Log-rank tests were used to test for differences in event-time distributions, and Cox proportional hazards models were fitted to obtain estimates of HRs in univariate and multivariate models. Multivariable Cox regression was analyzed in each of independent cohorts (DFCI and MGH) and in the combined cohort. A backward stepwise selection was used to generate the final models. All p values are two sided and CIs are at the 95% level, with significance predefined to be at <0.05.
Programmed death ligand 1 testing
The PD-L1 TPS was determined by immunohistochemistry using validated anti-PD-L1 antibodies: E1L3N (Cell Signaling Technology, Danvers, Massachusetts, USA) and 22C3 (Dako North America Inc, Carpinteria, California, USA).
Multiplexed immunofluorescence (ImmunoProfile)
Multiplexed immunofluorescence (mIF) was performed on samples from the DFCI by staining 5 µm formalin-fixed, paraffin-embedded whole tissue sections with standard, primary antibodies sequentially and paired with a unique fluorochrome, followed by staining with nuclear counterstain/4′,6-diamidino-2-phenylindole (DAPI).20 21 All samples were stained for PD-L1 (clone E1L3N), PD-1 (clone EPR4877(2)), CD8 (clone 4B11), FOXP3 (clone D608R), cytokeratin (clone AE1/AE3), and DAPI (nuclear counterstain). Each sample had a single slide stained and scanned at ×20 resolution by a Vectra Polaris imaging platform. Regions of interest (ROIs) were defined for each image, and only these regions were used for quantitative image analysis currently. Within each ROI, InForm Image Analysis software (PerkinElmer/Akoya) was run to phenotype and score cells based on biomarker expression. A custom script quantified the number/percentage of cells which are positive for relevant biomarkers in specific tissue regions. Each ROI was divided into one or more of these defined regions: IT, which was defined as the region of the slide consisting of tumor beyond the tumor-stroma interface (TSI); TSI, which was defined as the region within 40 microns to either side of the defined border between tumor and stroma; and total (IT+TSI). Cell count was calculated per ROI and averaged (unweighted) across ROIs, reported as count per millimeter squared±SE. Statistical significance of differential cell type enrichment between groups was estimated with Wilcoxon rank sum test.
Results
Patient population and dNLR
A total of 221 patients met eligibility criteria and were included in this study, with 147 (66.5%) in the DFCI cohort and 74 (33.5%) in the MGH cohort. The baseline clinicopathological characteristics of the 221 patients with advanced NSCLC (EGFR and ALK negative) and a PD-L1 TPS ≥50% who received first-line pembrolizumab are shown in table 1. The median age was 70 (range: 42–92), 95.9% were current/former smokers, and 80.1% had adenocarcinoma histology. In the entire cohort of patients, the median baseline dNLR was 2.5 (range 0.87–13.31). In 86.9% of cases (n=192), the CBC used for analysis was collected on the same day prior to the first dose of pembrolizumab (range 0–21 days prior to infusion).
Clinical and pathological characteristics of the 221 patients
Efficacy of pembrolizumab according to dNLR group
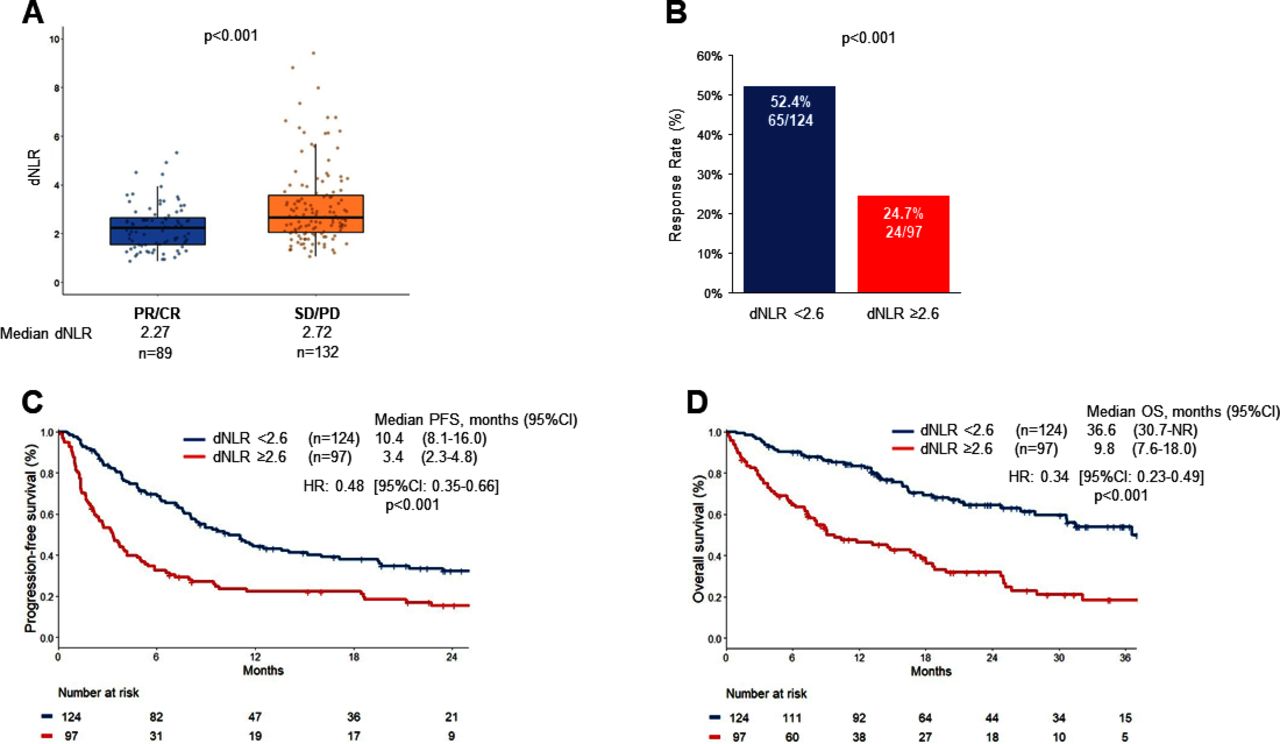
Among 221 patients with NSCLC and high-level PD-L1 treated with first-line commercial pembrolizumab, the ORR was 40.2% (95% CI 33.1% to 47.3). At a median follow-up of 26.9 months (95% CI 23.6 to 31.7), the median PFS (mPFS) was 6.8 months (95% CI 5.1 to 8.6), and the median OS (mOS) was 24.8 months (95% CI 17.8 to 30.7) calculated from the start date of immunotherapy. Patients who experienced a complete or partial response to pembrolizumab had a significantly lower median dNLR than patients with a best objective response of stable or progressive disease in the combined DFCI +MGH cohort (dNLR 2.27 vs 2.72, p<0.001, figure 1A), as well as in the individual DFCI and MGH cohorts (online supplemental figure 1).
Supplemental material
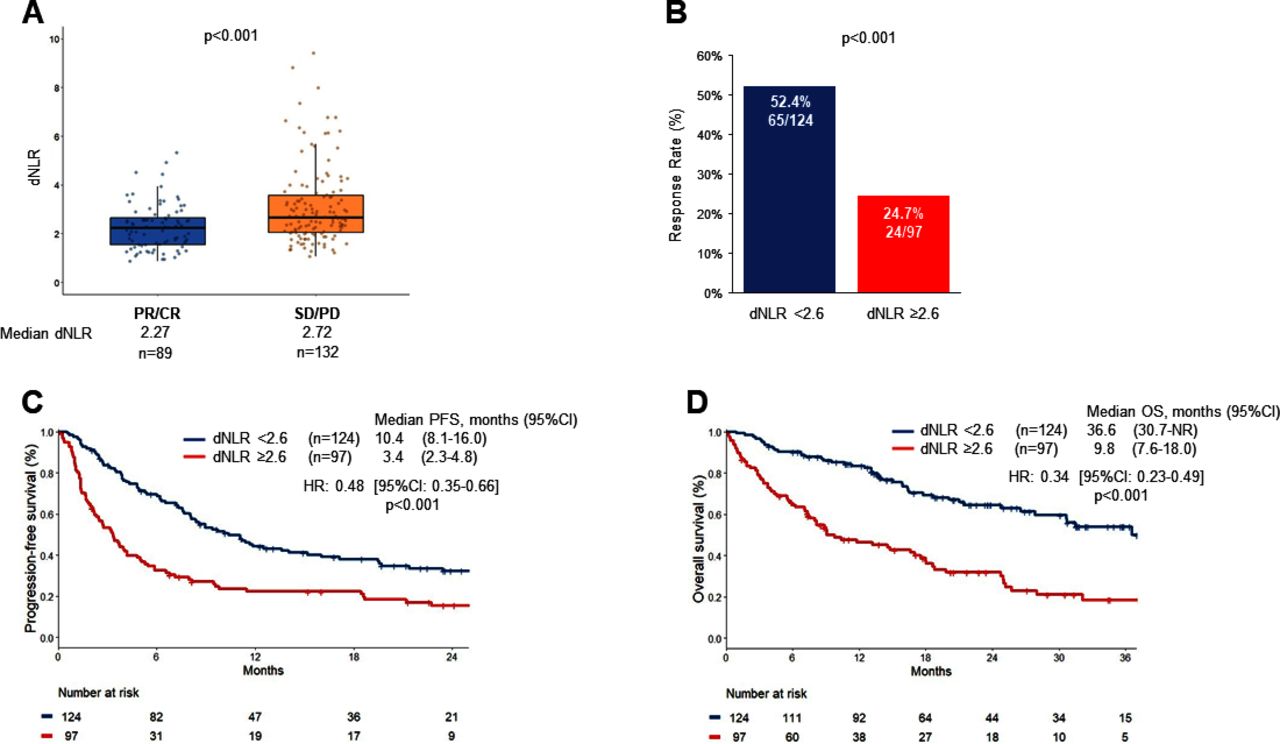
(A) Derived neutrophil-to-lymphocyte ratio (dNLR) from patients with NSCLC who experienced complete/partial response (CR/PR) or stable/progressive disease (SD/PD) as the best objective response to pembrolizumab. (B) Objective response rate, (C) progression-free survival (PFS), and (D) overall survival (OS), in patients with a dNLR <2.6 vs ≥2.6. NSCLC, non-small cell lung cancer. NR (not reached).
An unbiased recursive partitioning algorithm was used to assess for an optimal dNLR value with respect to ORR (online supplemental figure 2), which identified a primary split at a dNLR level of 2.59. This dNLR value was rounded up to 2.6 for further investigation; 124 patients (56.1% of the combined cohort) had a dNLR <2.6 and 97 patients (43.9% of the combined cohort) had a dNLR ≥2.6. Baseline clinicopathological characteristics were generally balanced between the two cohorts in terms of age, sex, performance status, tobacco use, histology, KRAS mutation status, presence of other potentially targetable driver mutations (BRAF, MET, HER2, RET), and PD-L1 TPS distribution (50%–89% vs ≥90%). Tumor mutational burden (TMB) was available for a subset of patients (n=111, 50.2%), and there was no significant difference between the groups. Higher albumin levels ≥3.5 g/dL were more common among patients with a dNLR <2.6 than ≥2.6 (p<0.001, table 2).
Supplemental material
Distribution of clinical characteristics by dNLR level
In patients with a dNLR <2.6, the ORR to pembrolizumab was 52.4% (95% CI 41.4% to 63.4%), which was significantly higher than the ORR of 24.7% (95% CI 16.2% to 33.2%) observed in patients with a dNLR ≥2.6 (p<0.001, figure 1B). The mPFS was significantly longer in the dNLR <2.6 group compared with dNLR ≥2.6 group (10.4 vs 3.4 months, HR 0.48, 95% CI 0.35 to 0.66, p<0.001, figure 1C). The mOS was also significantly longer in the dNLR <2.6 group compared with the dNLR ≥2.6 group (36.6 vs 9.8 months, HR 0.34, 95% CI 0.23 to 0.49, p<0.001, figure 1D). In each of the independent cohorts (DFCI and MGH), a dNLR <2.6 was associated with a significantly higher ORR, longer mPFS, and longer mOS to first-line pembrolizumab (online supplemental figure 3) (online supplemental table 1).
Supplemental material
Supplemental material
We also found that the ORR, PFS, and OS rates improved with decreasing dNLR values when dNLR was divided into tertiles (online supplemental figure 4A-C) or quartiles (online supplemental figure D-F) in the combined cohort of 221 patients. We found that a dNLR in the lowest vs highest quintile was associated with higher ORR (62.2 vs 18.2%), longer mPFS (17.1 vs 3.2 months), and longer mOS (not reached vs 7.4 months) to first-line pembrolizumab (figure 2). Individual immune cells and outcomes to pembrolizumab are shown in online supplemental figure 5). Highlighting the continuous nature of dNLR, we also observed the impact of increasing dNLR values and worsening clinical outcomes to ICI in a larger cohort of patients (n=924, (online supplemental table 2) who received immunotherapy as any line of therapy (first-line or subsequent line, online supplemental figure 6).
Supplemental material
Supplemental material
Supplemental material
Supplemental material

(A) Objective response rate, (B) progression-free (PFS), and (C) overall survival (OS) by quintiles of derived neutrophil-to-lymphocyte ratio (dNLR) values in the cohort of first-line pembrolizumab-treated patients.
As a very high PD-L1 expression levels (TPS ≥90%) are associated with improved clinical outcomes to pembrolizumab in the first-line setting,22 23 we also investigated the impact of dNLR among NSCLCs with a PD-L1 TPS of ≥90% and 50%–89%. In the cohort of 221 cases, 100 (45.2%) and 121 (54.8%) of NSCLCs had a PD-L1 expression level of ≥90% and 50%–89%, respectively. In the PD-L1 TPS ≥90% subgroup, a dNLR grouping of <2.6 vs ≥2.6 was also significantly associated with immunotherapy efficacy in terms of ORR (59.3% vs 34.8%; p=0.01), mPFS (13.6 months vs 4.0 months; HR 0.52, 95% CI 0.32 to 0.86; p=0.01), and mOS (40.1 months vs 13.2 months; HR 0.34, 95% CI 0.19 to 0.63; p<0.001) (online supplemental figure 7A-C). Similarly, among cases with a PD-L1 TPS of 50%–89%, a dNLR <2.6 conferred a higher ORR (47.1% vs 15.7%; p<0.001), a significantly longer mPFS (8.4 months vs 2.8 months; HR 0.40, 95% CI 0.27 to 0.61; p<0.001), and a significantly longer mOS (36.6 months vs 8.1 months; HR 0.33, 95% CI 0.20 to 0.54; p<0.001) compared with cases with dNLR ≥2.6 (online supplemental figure 7D-F).
Supplemental material
Multivariable analysis
After adjusting for age, sex, tobacco use, performance status, histology, serum albumin level, oncogenic driver status, and PD-L1 distribution (50%–89% vs ≥90%), the presence of a dNLR <2.6 was confirmed to be independently associated with longer mPFS (HR 0.47, 95% CI 0.33 to 0.67, p<0.001) and mOS (HR 0.32, 95% CI 0.21 to 0.49, p<0.001) in multivariable analysis (online supplemental table 3). A low dNLR <2.6 also demonstrated improved immunotherapy outcomes in univariate and multivariable analysis in the independent DFCI (online supplemental table 4) and MGH cohorts (online supplemental table 5
Early dNLR change correlates with clinical outcomes to pembrolizumab
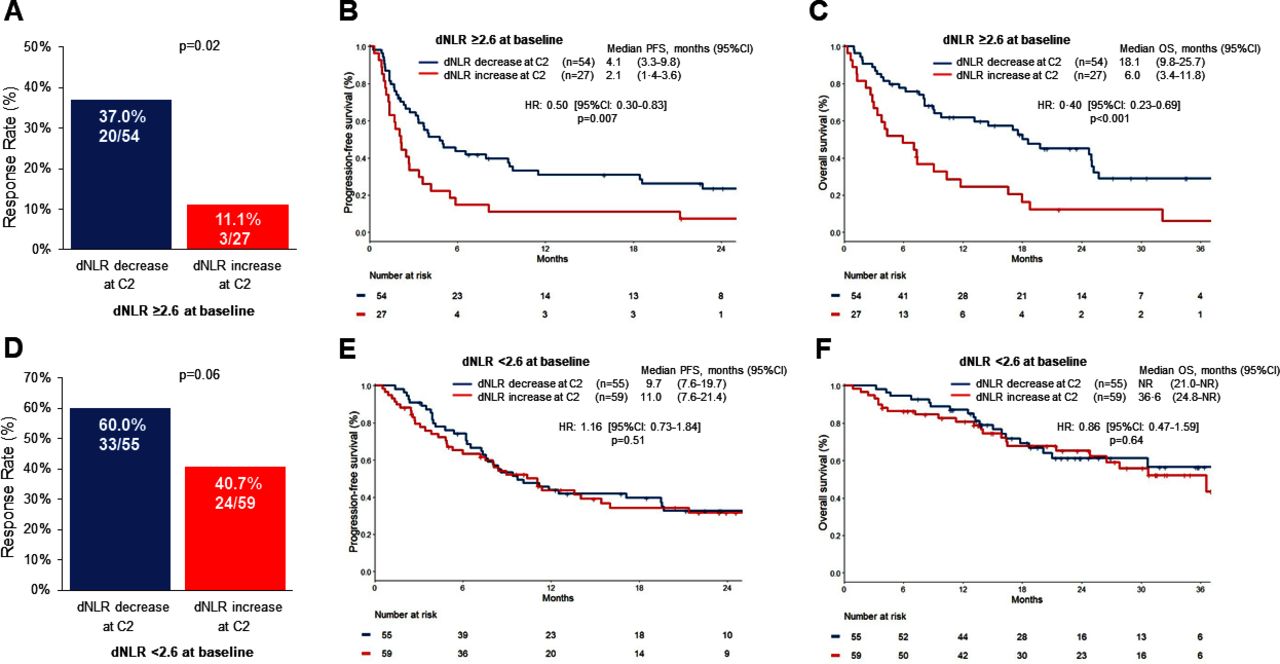
We next examined whether a change in the dNLR between baseline to the second cycle of pembrolizumab was associated with clinical outcomes. Among patients who initially had an unfavorable baseline dNLR ≥2.6 prior to starting first-line pembrolizumab we found that a decrease in dNLR at cycle 2 was associated with a higher ORR (37% vs 11.1%; p=0.02), longer mPFS (4.1 months vs 2.1 months; HR 0.50, 95% CI 0.30 to 0.83; p=0.007), and longer mOS (18.1 months vs 6.0 months; HR 0.40, 95% CI 0.23 to 0.69; p<0.001), when compared with patients with an increase in dNLR at cycle 2 (figure 3A–C). By contrast, among patients with a favorable baseline dNLR <2.6, we did not observe significant differences in clinical outcomes to pembrolizumab whether there was a subsequent increase or decrease in dNLR at cycle 2 (figure 3D–F). Among patients with a decrease in dNLR at cycle 2, the level of decrease (<25% vs ≥25%) did not significantly impact clinical outcomes to pembrolizumab (online supplemental figure 8).
Supplemental material
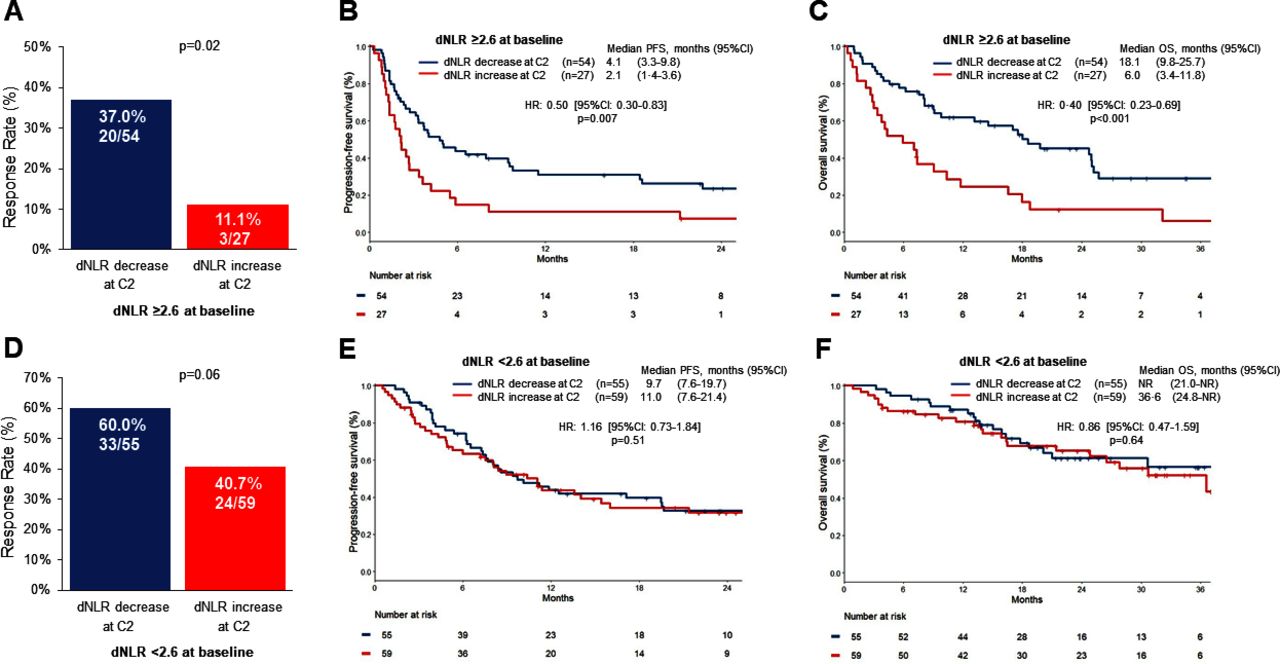
(A) Objective response rate, (B) progression-free survival (PFS), and (C) overall survival (OS) to pembrolizumab in patients with a baseline dNLR of ≥2.6, followed by a decrease or an increase in dNLR at cycle 2 (C2) of pembrolizumab. (D) Objective response rate, (E) PFS, and (F) OS to pembrolizumab in patients with a baseline dNLR of <2.6, followed by a decrease or an increase in dNLR at cycle 2 (C2) of pembrolizumab. dLNR, derived neutrophil-to-lymphocyte ratio. NR (not reached).
Association of dNLR with immunophenotype of the TME
To better understand how a peripheral blood dNLR might be associated with improved tumorous responses to ICIs, we performed mIF for CD8, FOXP3, PD-1, and PD-L1 on a separate cohort of 243 NSCLCs at DFCI (n=141 early stage; n=102 advanced stage) to correlate dNLR with tumor immunophenotype.
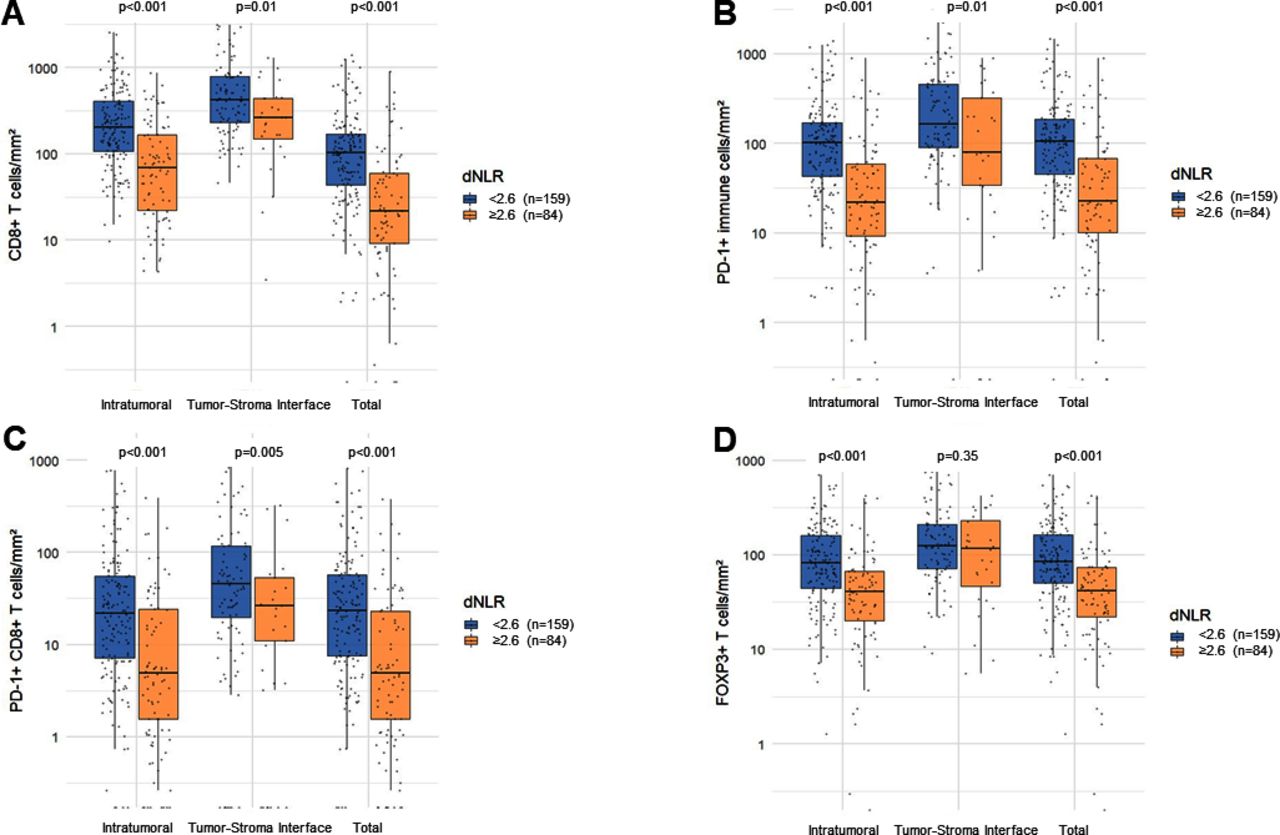
Compared with cases with dNLR ≥2.6 (n=84), we found that patients with a dNLR <2.6 (n=159) at the time of tumor biopsy had significantly higher numbers of CD8+, PD-1 +immune cells, and PD-1 +CD8+T cells, IT, within the TSI, and in total (IT+TSI) (figure 4). Additionally, patients with a dNLR <2.6 also had significantly higher number of FOXP3 +T cells both IT and in total, as shown in figure 4. By contrast, the PD-L1 expression levels on tumor cells, on immune cells, and in total, were not significantly different between dNLR high and low groups (online supplemental figure 9). We also observed that the immune cell subsets increased with decreasing dNLR values when dNLR was divided into quartiles and quintiles (online supplemental figures 10 and 11). Among the subset of NSCLCs with advanced stage disease and a PD-L1 TPS ≥50% by IHC (n=46), a dNLR <2.6 was still significantly associated with enrichment of IT CD8+, PD-1+, PD-1 +CD8+, and FOXP3 +cells (online supplemental figure 12). In this subgroup, 33 of 46 cases subsequently received first-line pembrolizumab, with a median interval between biopsy with ImmunoProfile and treatment initiation of 40 days (range 6–180).
Supplemental material
Supplemental material
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of intratumoral, tumor-stroma interface, and total (intratumoral +tumor-stroma interface) (A) CD8 +T cells, (B) PD-1 +immune cells, (C) PD-1 +CD8+T cells, and (D) FOXP3 +T cells in tumors according to derived neutrophil-to-lymphocyte ratio (dNLR) group (<2.6 vs ≥2.6).
An increasing dNLR was associated with decreases in CD8+, PD-1+, PD-1 +CD8+, and FOXP3 +cells IT and in total but not at the tumor-stromal interface (online supplemental figure 13). An increasing dNLR was associated with increasing tumorous PD-L1 expression, but there was no significant association with PD-L1 expression on immune cells or in total (online supplemental figure 14).
Supplemental material
Supplemental material
Discussion
In this study, we report that among patients with NSCLC and a PD-L1 expression level ≥50% treated with first-line pembrolizumab, clinical outcomes are improved with decreasing dNLR levels and particularly a dNLR <2.6. Additionally, for patients with an unfavorable baseline dNLR ≥2.6 prior to starting pembrolizumab, a subsequent decrease in dNLR at cycle 2 of pembrolizumab was associated with better clinical outcomes than for patients who experienced an increase in dNLR at cycle 2. We also demonstrate that an increased peripheral blood dNLR is associated with decreased immune cells within the TME. To our knowledge, this study represents the largest retrospective cohort of patients with advanced NSCLC and a PD-L1 TPS ≥50% treated with first-line pembrolizumab and dNLR analysis to date.
PD-L1 expression levels often impact current treatment decisions in the first-line setting for patients with NSCLC lacking targetable genomic alterations.14 24 Although high levels of PD-L1 on tumor cells enrich for response to immunotherapy, less than half of patients with NSCLC and a PD-L1 TPS ≥50% respond to pembrolizumab monotherapy.14 A lingering question is whether to use single-agent PD-(L)1 inhibition or a PD-(L)1 inhibitor plus chemotherapy in patients with NSCLC and a PD-L1 level of ≥50% since there has been no direct comparison between the two regimens in this population. Our results suggest that patients with NSCLC and a low baseline dNLR might have favorable outcomes to pembrolizumab monotherapy and avoid the potential added toxicities of immunotherapy plus chemotherapy.22 23
Our observation that an early increase in dNLR between cycle 1 and cycle 2 of pembrolizumab in patients with a baseline dNLR value ≥2.6 is associated with worse clinical outcomes may identify individuals who are at greatest risk for disease progression on pembrolizumab monotherapy prior to radiological assessment. In these patients, an early identification of non-response to pembrolizumab through dNLR monitoring could potentially inform how to implement alternative therapeutic approaches in a timely fashion. In contrast to a previous report showing that a moderate decrease in NLR, but not a steep decrease, was associated with response to immunotherapy,9 we did not find that a drop in dNLR by ≥25% vs<25% impacted ORR, PFS, or OS to pembrolizumab. While the prior study was also conducted on a large cohort of patients, baseline clinicopathological characteristics were not reported among those who received ICIs; therefore, whether imbalances in such features and other contributors could have impacted the outcomes is unknown. Lastly, a recent retrospective analysis of 115 patients with NSCLC treated with PD-(L)1 inhibitors showed that a low pretreatment NLR may predict for the occurrence of immune-related adverse events (irAEs); whether dNLR changes may further correlated with the risk of irAE develop needs to be assessed in future studies.25
There are an increasing number of continuous biomarkers associated with ICI efficacy, including PD-L1 expression, infiltrating immune cells, and TMB.26–28 Likewise, dNLR appears to behave in a continuous fashion, both in terms of therapeutic outcomes to ICI, and also with the tumor immunophenotype. To gain insight of the potential mechanism by which dNLR in the peripheral blood was associated with PD-1 efficacy in NSCLC, we interrogated the immune cell infiltrates by mIF, and found that tumors display distinct immunophenotypes according to dNLR level. In our cohort of NSCLC samples, increasing dNLR values were associated with decreases in tumor immune infiltrates. Importantly, increasing levels of CD8 +T cells and PD-1 expression by CD8 +T cells within the TME of NSCLCs have shown improved clinical outcomes with PD-1 blockade.29 Therefore, integration of TMB and PD-L1 expression with dNLR may refine treatment selection for patients with NSCLC.6 30 In addition, examination of the immunophenotype of circulating immune cells along with dNLR may help determine which patients are more likely to respond to ICIs.10 31
Our study is limited by its retrospective nature. Furthermore, a different dNLR cut-off of 2.6 was used in this study compared with a dNLR of 3 previously reported in NSCLC.32 However, the dNLR threshold of 3 was previously derived from patients with melanoma receiving ipilimumab.32 33 Here, using an unbiased approach, we identified a dNLR cut-off of 2.6 as the strongest discriminator of response to first-line pembrolizumab in two independent cohorts of NSCLC. In contrast to similar studies that included patients on corticosteroid therapy at the time of dNLR assessment, our study only examined cases with no history of steroid use, which may reflect a more accurate relationship between dNLR and ICI efficacy because corticosteroid administration can increase the peripheral neutrophil count.34 Lastly, the predictive role of dNLR for first-line treatment with pembrolizumab in patients with NSCLCs and a PD-L1 TPS ≥50% needs to be validated prospectively.
In conclusion, NSCLCs with PD-L1 TPS ≥50% and a low dNLR have a distinct immune microenvironment and more favorable outcomes to first-line pembrolizumab. Therefore, additional strategies to antagonize neutrophils and correlated pathways may represent a viable secondary therapeutic strategy to enhance ICI treatment outcomes. Furthermore, incorporation of dNLR may have implications for treatment decision making, guide the design of clinical trials, and the direction of future research in this area.
Supplemental material
Data availability statement
Data are available on reasonable request. The data that support the finding of our study are available on request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
We also included a separate cohort of 243 NSCLCs from DFCI who provided written informed consent to institutional review board-approved protocols DF/HCC #11-104 or #17-000 and who underwent successful multiplexed immunofluorescence (mIF) testing on tumor samples.
Acknowledgments
We are grateful to Howard Cox for his support of ImmunoProfile and the DFCI.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1
- Data supplement 2
- Data supplement 3
- Data supplement 4
- Data supplement 5
- Data supplement 6
- Data supplement 7
- Data supplement 8
- Data supplement 9
- Data supplement 10
- Data supplement 11
- Data supplement 12
- Data supplement 13
- Data supplement 14
- Data supplement 15
- Data supplement 16
- Data supplement 17
Footnotes
Twitter @alessi_joao, @DrMarkAwad
Contributors The study conducts and design: JVA, BR, JFG, and MMA; data acquisition: JVA, BR, SLA, AAB, MN, and MS; statistical analysis: JVA and BR; data interpretation: JVA, BR, JJL, JFG, and MMA; drafting the manuscript or revising it critically: all authors; final approval of the manuscript: all authors.
Guarantors: JVA, BR, and MMA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MMA serves as a consultant to Merck, Bristol-Myers Squibb, Genentech, AstraZeneca, Nektar, Maverick, Blueprint Medicine, Syndax, Abbvie, Gritstone, ArcherDX, Mirati, NextCure, and EMD Serono. Research Funding: Bristol-Myers Squibb, Lilly, Genentech and AstraZeneca. JFG has served as a compensated consultant or received honoraria from Bristol-Myers Squibb, Genentech, Ariad/Takeda, Loxo, Pfizer, Incyte, Novartis, Merck, Agios, Amgen, Jounce, Karyopharm, GlydeBio, Regeneron, Oncorus, Helsinn, Jounce, Array, and Clovis Oncology, has an immediate family member who is an employee with equity in Ironwood Pharmaceuticals, has received research funding from Novartis, Genentech/Roche, and Ariad/Takeda, and institutional research support from Tesaro, Moderna, Blueprint, BMS, Jounce, Array, Adaptimmune, Novartis, Genentech/Roche, Alexo and Merck. JJL has served as a compensated consultant for Genentech, C4 Therapeutics, Blueprint 2 Medicines, Nuvalent, Turning Point Therapeutics, and Elevation Oncology; received honorarium 3 and travel support from Pfizer; received institutional research funds from Hengrui Therapeutics, 4 Turning Point Therapeutics, Neon Therapeutics, Relay Therapeutics, Bayer, Elevation 5 Oncology, Roche, and Novartis; received CME funding from OncLive, MedStar Health, and 6 Northwell Health. MN Consultant to Daiichi Sankyo, AstraZeneca; Research grant from Merck, Canon Medical Systems, AstraZeneca, Daiichi Sankyo; Honorarium from Roche. MN is also supported by R01CA203636 and U01CA209414 (NCI)). JVA, BR, SLA, AAB, MS, VRV, JL, MMT, KP, BS, KDF, and SJR: nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.