Article Text

Abstract
Background Basal cell carcinoma (BCC) is the most common malignancy worldwide, yet the management of patients with advanced or metastatic disease is challenging, with limited treatment options. Recently, programmed death receptor 1 (PD-1) inhibition has demonstrated activity in BCC after prior Hedgehog inhibitor treatment.
Methods We conducted a multicenter, retrospective analysis of BCC patients treated with PD-1 inhibitor therapy. We examined the efficacy and safety of PD-1 therapy, as well as clinical and pathological variables in association with outcomes. Progression-free survival (PFS), overall survival (OS) and duration of response (DOR) were calculated using Kaplan-Meier methodology. Toxicity was graded per Common Terminology Criteria for Adverse Events V.5.0.
Results A total of 29 patients with BCC who were treated with PD-1 inhibition were included for analysis, including 20 (69.0%) with locally advanced and 9 (31.0%) with metastatic disease. The objective response rate was 31.0%, with five partial responses (17.2%), and four complete responses (13.8%). Nine patients had stable disease (31.0%), with a disease control rate of 62.1%. The median DOR was not reached. Median PFS was 12.2 months (95% CI 0.0 to 27.4). Median OS was 32.4 months (95% CI 18.1 to 46.7). Two patients (6.9%) developed grade 3 or higher toxicity, while four patients (13.8%) discontinued PD-1 inhibition because of toxicity. Higher platelets (p=0.022) and any grade toxicity (p=0.024) were significantly associated with disease control rate.
Conclusions The clinical efficacy of PD-1 inhibition among patients with advanced or metastatic BCC in this real-world cohort were comparable to published trial data. Further investigation of PD-1 inhibition is needed to define its optimal role for patients with this disease.
- immunotherapy
- skin neoplasms
- programmed cell death 1 receptor
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
KEY MESSAGES
Historically, systemic treatment options have been limited for patients with advanced basal cell carcinoma. In February 2021, the Food and Drug Administration approved use of the PD-1 inhibitor cemiplimab for patients who have been treated with prior Hedgehog inhibition. In this multicenter, retrospective study, PD-1 inhibition led to a response rate of 31.0% for patients with basal cell carcinoma; these responses were durable, lasting greater than 12 months. Furthermore, treatment was well tolerated with a discontinuation rate of 13.8%. Our results provide real-world confirmation of those from the REGN 1620 trial and support the incorporation of PD-1 inhibition into the management of patients with unresectable or metastatic basal cell carcinoma.
Introduction
Basal cell carcinoma (BCC) is the most common cancer in the USA,1 2 with more than 2 million cases diagnosed annually. Small, localized lesions are typically cured with minimally invasive approaches, including surgery, topical or photodynamic therapy, with good long-term outcomes.3–5 However, a subset of BCC patients may present with recurrent disease, local invasion of adjacent structures, or metastatic disease, resulting in significant morbidity or mortality.6–8 Risk factors for recurrent or metastatic BCC include a history of immune suppression, larger primary tumor size, location on the head/neck, perineural invasion and aggressive histology, such as morpheaform or basosquamous histology.9–13 Management of advanced BCC may be clinically challenging, and should be discussed in a multidisciplinary setting. In addition to surgical management, radiation and systemic therapy may be considered. However, due to the rarity of locally advanced and especially metastatic BCC, there are no standard management guidelines for this clinical scenario, thus presenting an important, unmet need.
At a molecular level, BCC is characterized by upregulation of the Hedgehog pathway, whereby mutations of PTCH1, SMO or SUFU drive translocation of SMO and downstream transcription of GLI target genes. Inhibitors of the Hedgehog pathway (HHI) have been established as the first-line systemic therapy for patients with advanced or metastatic BCC,14–16 but the use of these agents may be limited by toxicity and tolerability issues, requiring frequent dose interruptions or modifications.17 18 Moreover, resistance to HHI may occur as a result of mutations of SMO, SUFU, or GLI2, or via upregulation of other synergistic pathways.19–21 As such, salvage therapy options for patients who fail HHI are needed.
Blockade of the programmed death-1 protein (PD-1) has demonstrated efficacy in cutaneous malignancies, among others.22–24 Specifically, PD-1 inhibitors produce durable responses, resulting in improved survival, and even allow some patients to safely discontinue therapy while continuing to benefit from treatment.25 Moreover, PD-1 inhibitor therapy is well tolerated compared with many systemic agents, and has been shown to be safe among older, frail patients.26 27
Multiple levels of evidence support the use of PD-1 inhibition in advanced BCC. Similar to other cutaneous malignancies, BCC are characterized by a UV radiation mutational signature and high tumor mutational burden (TMB).28 29 In addition, programmed death-ligand 1 (PD-L1) expression has been reported on BCC tumor cells, as well as associated tumor-infiltrating lymphocytes and macrophages.30 The increased incidence of BCC among patients with immune suppression, as well as the efficacy of other immune modulating therapies, such as imiquimod, further supports the use of PD-1 inhibition in this malignancy. In a phase II study of 84 patients with locally advanced, unresectable BCC who had failed prior HHI, PD-1 inhibitor therapy led to an objective response rate (ORR) of 31% (25% partial response (PR), 6% complete response (CR)); median progression-free survival (PFS) was 19 months, and responses were durable, with 79% of responses maintained beyond 6 months.31 In February 2021, the US Food and Drug Administration (FDA) approved use of the PD-1 inhibitor, cemiplimab, as second-line therapy for BCC after prior therapy with HHI. Here, we present a multi-institutional, retrospective study of BCC patients treated with PD-1 inhibition.
Patients and methods
We conducted a multi-institutional, retrospective analysis of BCC patients treated with PD-1 inhibitor therapy between 2016 and 2021 across eight academic medical centers in the USA. Patients who had locally advanced or metastatic BCC and received at least 1 cycle of PD-1 inhibition in any line of therapy were eligible for inclusion. Clinical data were collected from patient medical records at each respective institution, then deidentified and merged into a central database prior to analysis. Patient demographics, including age, race, gender, and history of immune suppression were recorded. Tumor characteristics collected included date of diagnosis, tumor location, tumor diameter, presence of perineural invasion, poor vs well-defined borders, history of recurrent tumor, histology subtype, date of advanced disease, extent of disease (locally advanced vs metastatic), prior therapy for advanced disease (including surgery, radiation and HHI), Eastern Cooperative Oncology Group (ECOG) performance status at start of PD-1 therapy, TMB, baseline labs (complete blood count, liver function tests, creatinine, albumin), sites of metastatic disease, PD-1 inhibitor agent used, total cycles of PD-1 therapy, toxicity (including grade), best response, and reason for discontinuation. Dosing of PD-1 inhibitors was carried out using standard FDA approved labeling, with either (1) cemiplimab 350 mg every 3 weeks, (2) pembrolizumab 200 mg every 3 weeks, or 400 mg every 6 weeks, or (3) nivolumab 240 mg every 2 weeks or 480 mg every 4 weeks.
Efficacy was assessed by Response Evaluation Criteria in Solid Tumors V.1.1, as conducted by site investigators at each participating institution. Patients were evaluable for response if they had measurable disease, either by radiographic imaging, or by caliper measurement with medical photography for superficial cutaneous lesions. ORR was defined by the presence of CR or PR. Disease control rate (DCR) comprised patients who achieved CR, PR or stable disease (SD). Toxicity was retrospectively graded by each respective institutional investigator, per the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) V.5.0. PFS and overall survival (OS) were calculated from the date of the first cycle of PD-1 inhibition to the date of progression or death from any cause, respectively. Duration of response (DOR) was calculated from the time of initial response (PR or CR) until death or progression. Patients who did not experience death or progression, or those lost to follow-up, were censored.
All analyses were performed utilizing SPSS Statistics V.28.0.0. Descriptive statistics for all categorical data were reported. Categorical variables were reported as total numbers and percentages. No imputation was made for missing data. PFS, OS and DOR were estimated by Kaplan-Meier methodology and expressed as median values with two-sided 95% CIs. Survival curves were compared using log-rank test (Mantel-Cox) tests. Univariate analysis was performed using linear regressions and least squares on individual variables of interest with significance defined as p<0.05. For multivariate analysis, a correlation matrix was used to calculate Pearson correlation coefficient (Pearson’s r) values and their significance (p<0.05).
Results
Study population
In total, 29 BCC patients who were treated with PD-1 inhibitor therapy between August 2016 and June 2021 were included for analysis (figure 1). Complete baseline demographic and clinical information are listed in table 1. The median age at the time of PD-1 inhibition was 70 years (range 43–86), with 58.6% of patients 70 years or older, and 27.6% being 75 years or older. The majority of patients were male (75.9%) and Caucasian/white (86.2%). Most patients had good performance status, ECOG 0–1 (86.2%). Primary BCC tumors were located on the head/neck for more than half of all patients (55.2%), followed by the trunk (27.6%) and extremity (17.2%). Aggressive histology was reported in 19 patients (65.5%); aggressive subtypes included basosquamous (27.6%), morpheaform (13.8%) and micronodular (6.9%). Three patients (10.3%) had a history of immunocompromise, including one each with a history of autoimmune disease, hematological malignancy, or viral immune suppression. Among all 29 patients, 20 (69.0%) had locally advanced disease, while 9 (31.0%) had metastatic disease. The most common anatomic sites of metastasis included lung (24.1%) and lymph node (20.7%). Twenty-one patients (72.4%) had undergone prior surgery as therapy for BCC, while 18 (62.1%) had been treated with prior radiation. In addition, 24 patients (82.8%) had been treated with prior HHI, among which 18 (75.0%) discontinued therapy due to disease progression. TMB was available for 10 patients; the median TMB was 14 mutations/Mb (range 3.2–111).

CONSORT diagram of basal cell carcinoma patients included in analysis. CONSORT, Consolidated Standards of Reporting Trials.
Baseline characteristics of patients
Treatment outcomes
At the time of data collection (June 2021), the median follow-up for the overall study population was 11.0 months; 11 patients had died, while 17 were alive with at least 3 months of follow-up, and 1 was lost to follow-up and censored. The median number of cycles of PD-1 inhibition administered among all patients was 6 (range 1–57), while the median duration of therapy was 4.8 months (range 1–44). PD-1 inhibitors used included pembrolizumab (58.6%), cemiplimab (31.0%), and nivolumab (10.3%).
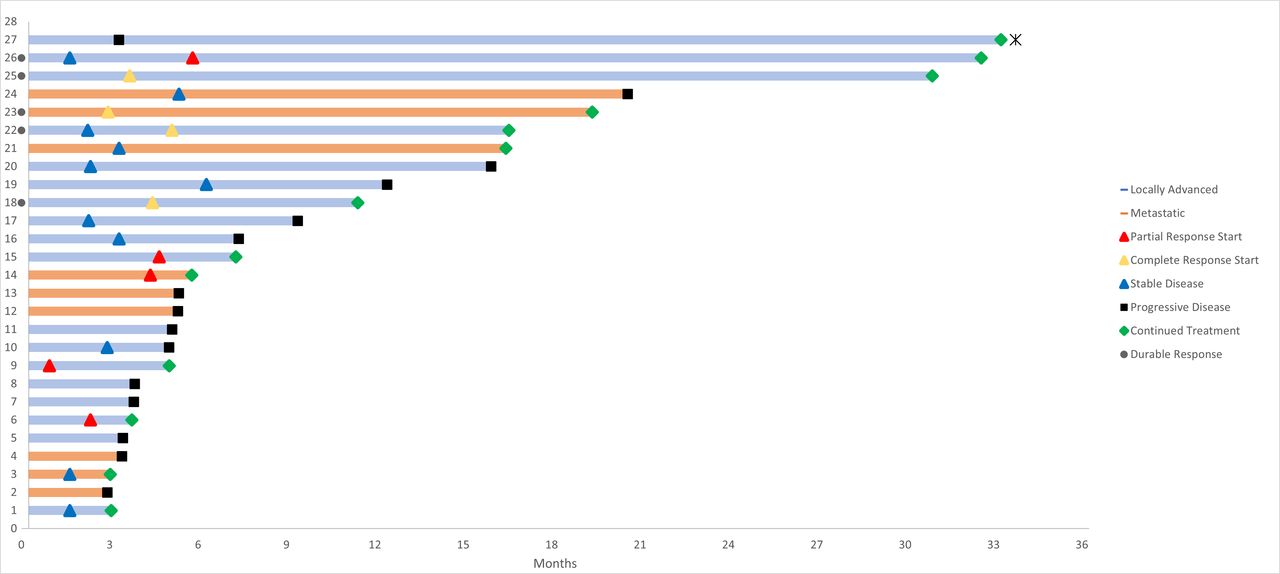
Efficacy data are summarized in table 2. Among all patients evaluable, there were five patients (17.2%) with PR and four patients (13.8%) with CR; the ORR was 31.0%. There were two patients who initially had SD, but subsequently converted to a response (one PR and one CR). The median time to response among patients with PR or CR was 4.0 months (range 0.7–5.6). One patient who had PD at 3.5 months underwent local ablation therapy to treat oligometastatic disease, then continued on therapy for another 29 months. In total, nine patients (31.0%) had SD as the best response, while another nine patients (31.0%) had progression of disease, and two were not evaluable (NE). DCR for the entire cohort was 62.1%.
Antitumor efficacy among patients with BCC treated with PD-1 inhibition
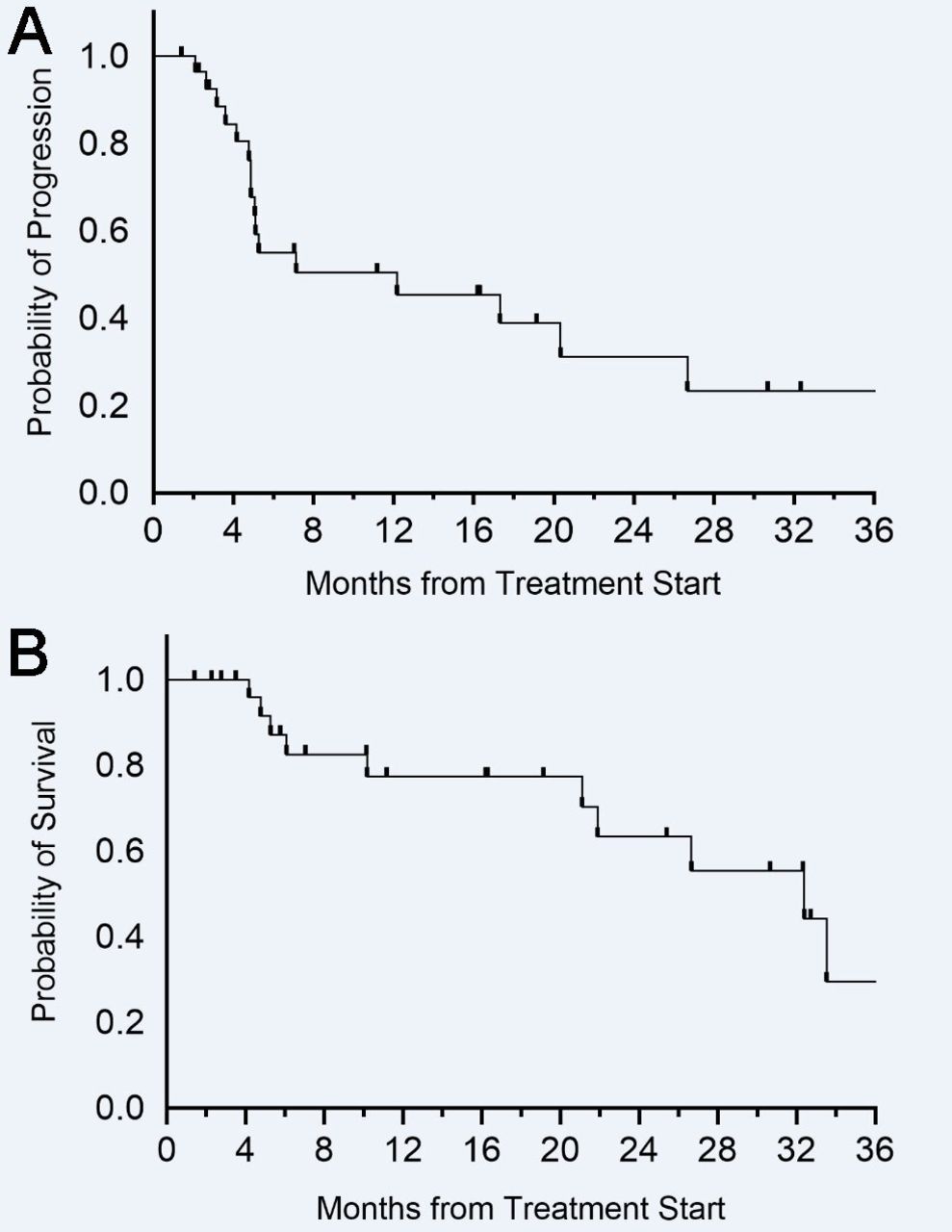
For patients who achieved PR or CR, the median DOR was not reached. Among responders, the proportion of those who remained in PR or CR at 12 months was 100% (6/6) (figure 2). Three responders had less than 6 months of follow-up and were excluded from assessment of DOR proportion. No progression events were observed in patients with a PR or CR. For patients with SD, the median duration of benefit was 10.1 months (range 4.1–15.2). The estimated median PFS for all patients included was 12.2 months (95% CI 0.0 to 27.4) (figure 3A); the median OS was 32.4 months (95% CI 18.1 to 46.7) (figure 3B). There were no clinical or pathological variables that were significantly associated with either PFS or OS.

Swimmer’s plot of BCC patients treated with PD-1 inhibition. BCC, basal cell carcinoma.

{kind=link}
{kind=link}
{kind=link}
(A) Progression-free survival of BCC patients treated with PD-1 inhibition. (B) Overall survival of BCC patients treated with PD-1 inhibition. BCC, basal cell carcinoma.
On subset analysis, the ORR for patients with locally advanced disease was 35.0% (four PR, three CR), while for patients with metastatic disease, the ORR was 22.2% (one PR, one CR). Among five patients who were naïve to therapy with HHI, there were three responders (2 PR, 1 CR), and two with SD. When assessing efficacy among older patients, the ORR for patients 70 years and older was 23.5% (4/17), with 1 PR and 3 CR, with DCR 58.8% (10/17), while the ORR for patients 75 years and older was 25.0% (1/8) with 1 CR and 0 PR, with DCR 62.5% (5/8). The ORR for primary tumors on the head/neck, trunk, and extremity were 31.3% (5/13), 25.0% (2/8), and 40.0% (2/5), respectively. For patients with aggressive histology, the ORR was 38.9% (7/18), compared with 18.2% (2/11) among those without. Regarding specific histology subtypes, three of eight patients with basosquamous histology achieved a response (two CR, one PR), while among four patients with morpheaform histology, there was one response, two non-responders, and a third patient was NE. There were two patients with micronodular histology, both were non-responders. Among the 3 immunocompromised patients, there were no responses seen, although 1 patient with metastatic BCC and a history of pemphigus vulgaris had SD and underwent a total 18 cycles of nivolumab. Among the responders, there were only two patients with TMB data available: one with 47 mutations/Mb, and another with 111 mutations/Mb. Among the non-responders, TMB was available for 8 patients: 3 patients had TMB of 5 mutations/Mb or lower, 3 had TMB 10–15 mutations/Mb, and 2 patients had TMB higher than 50 mutations/Mb (63 and 91). None of the variables mentioned above, nor any others, including gender, performance status, or prior therapy, were significantly associated with response to PD-1 therapy (online supplemental S1). Among baseline laboratory values, higher albumin showed a trend toward significance (p=0.052), in association with response. Higher platelets (p=0.022) and any grade toxicity (p=0.024) were significantly associated with DCR; there were no other variables associated with DCR (online supplemental S2).
Supplemental material
Supplemental material
Supplemental material
Salvage therapy outcomes were available for seven patients who progressed on PD-1 therapy. Among three patients retreated with HHI, there was one response. Among three patients treated with CTLA-4 as salvage therapy, there were zero responses reported, with two having SD and one with disease progression as best response. One patient treated with cytotoxic chemotherapy achieved a response.
Safety
Overall, there were 19 patients (65.5%) who developed any grade toxicity due to PD-1 therapy (table 3). The most common toxicities included constitutional symptoms (fatigue) affecting 34.5% of patients, dermatological symptoms (rash, pruritus) in 24.1%, and endocrinopathies (hypothyroidism) among 13.8%; all of these were CTCAE grade 2 or lower. Two patients (6.9%) developed treatment-related adverse events of CTCAE grade 3 or higher; these included one patient with grade 3 colitis and another patient who had concurrent grade 4 transaminitis and grade 4 nephritis. In total, 4 patients (13.8%) discontinued PD-1 therapy due to toxicity; in addition to the 2 patients with grade 3 or higher adverse events, there was one patient with grade 2 encephalitis and another patient who had both grade 2 arthralgias and grade 2 fatigue, who also discontinued treatment. Other reported adverse effects of grade 2 or lower included CK elevation and infusion reaction. There were no fatal adverse events in this population. There was no significant difference in toxicity of any grade (p=0.24), nor grade 3 or higher toxicity (p=0.66), when comparing patients who were older than 70 years old, vs those who were younger. When using a cut-off of 75 years or older, there was again no significant difference in any grade toxicity (p=0.98), nor for grade 3 or higher toxicity (p=0.32).
Adverse events among patients with BCC treated with PD-1 inhibition
Discussion
Here, we describe our real-world experience using PD-1 therapy in the treatment of advanced BCC. To our knowledge, this is the largest such retrospective study to date, and the first to provide a multi-institutional cohort across distinct academic medical centers that specialize in the treatment of advanced cutaneous malignancies. Given the low incidence of locally advanced and metastatic BCC, and limited prospective data, the overall intent of this study was to help impart greater clinical insight into the management of this challenging disease using PD-1 inhibition.
The findings of this study are largely reflective of those from the pivotal phase II REGN 1620 cohort of 84 locally advanced BCC patients .31 In our patient population, we observed an ORR of 31.0% for BCC patients treated with PD-1 therapy, which was the same as that seen in the REGN 1620 study. The DCR from our study was discernibly lower than that seen in REGN 1620 (62.1% vs 80.0%), as was the median PFS (12.2 vs 19.0 months). We found that 13.8% of patients in our cohort achieved a CR, which is approximately double that (6%) from REGN 1620; however, it must be noted that unlike REGN 1620, histological confirmation was not required for our study population, and among three locally advanced BCC patients who had CR, only one had a biopsy to confirm this response. These differences in outcomes may also derive from the fact that our patient population was more heterogeneous, having included patients with both locally advanced and metastatic disease. Within the metastatic cohort of 28 BCC patients treated with cemiplimab on REGN 1620, the ORR was 21.0%, with DCR 67.9% and median PFS 8.3 months,32 suggesting that PD-1 inhibition may have lower efficacy in the metastatic setting. Although our cohort had a much smaller sample size of patients with metastatic disease (n=9), we also found that efficacy was lower for these patients compared with those with locally advanced disease, both in terms of ORR (22.2% vs 35.0%) and DCR (55.5% vs 65.0%), but this was not statistically significant. Another difference within our cohort was the inclusion of five patients (17.2%) who were naïve to treatment with HHI; among these there were three responders, and two had SD. PD-1 inhibition results in greater efficacy when used as first-line treatment for melanoma33 34 and Merkel cell carcinoma,23 35 compared with later lines of therapy, although this difference is not as clear for cutaneous squamous cell carcinoma.36 37 Hence, future studies to delineate the role of checkpoint blockade as first-line treatment for BCC should be investigated.
Additionally, our study confirms that responses to PD-1 therapy among patients with advanced BCC are durable. In the locally advanced BCC cohort from REGN 1620, 79% had durable responses longer than 6 months, while in the metastatic cohort, this was noted in all six patients (100%). In our study, six of six responses exceeded 6 and 12 months as well. Moreover, we observed that two patients who initially presented with SD, subsequently achieved a response (one PR, one CR), suggesting that responses to PD-1 therapy may deepen over time, as seen in other malignancies.38 39 Despite these promising findings, there remains the question of whether tumor regressions will continue once PD-1 therapy has been stopped. In a retrospective study of 110 BCC patients who achieved CR to HHI but then discontinued treatment, nearly half of the patients (48.1%) experienced a relapse while off treatment.40 It has been shown that patients with advanced melanoma who experience CR following 2 years of treatment with PD-1 therapy can safely discontinue treatment.25 Meanwhile, patients with Merkel cell carcinoma who discontinue PD-1 therapy after CR appear to have higher risk of relapse,41 suggesting these outcomes may differ with tumor type. This question should be further evaluated for BCC patients who achieve CR, as the risk–benefit ratio of continuing treatment may change once patients are free of disease. Nevertheless, the possibility of durable response to salvage PD-1 inhibition fills a critical, unmet need for patients with BCC who have disease progression after treatment with HHI.
Our study found that PD-1 therapy was well tolerated in this real-world cohort of patients with advanced BCC, consistent not only with REGN 1620, but also other published trial data of PD-1 inhibitors.22–24 31 33–35 While nearly two-thirds of patients did experience toxicity of any grade, only two patients (6.9%) developed grade 3–4 toxicity, and four patients (13.8%) discontinued therapy because of toxicity. These safety data are notable when juxtaposed against those from HHI, which result in grade 3–4 toxicity among 43%–64% of patients, with drug discontinuation rates ranging from 14% to 31%.14–16 As BCC is predominantly a disease that afflicts the aged, we also sought to assess the safety of PD-1 therapy for these patients in particular. While our cohort also had a median age of 70 years old, similar to REGN 1620, we actually had a higher upper range age, with 27.6% of patients over 75 years, and 10.3% over 80 years old. Among these older age subsets, we did not observe any unusual safety signals, with grade 3–4 toxicity ranging from 11.8% to 25.0%, consistent with other studies using single agent PD-1 inhibitors in this population.26 27 42 Further observational studies are needed to monitor for toxicity in these patients, as they are often excluded from clinical trials.
Molecular biomarkers, to select which BCC patients will respond to PD-1 inhibition, remain a priority. Correlative biomarker analyses, including TMB, PD-L1 expression and MHC-I expression, failed to predict response to treatment in REGN 1620, although the authors found that downregulation of MHC-I was seen in some non-responders with high TMB.31 Although limited by sample size (34.5% of this cohort), we also found that TMB was not predictive of response; high TMB values greater than 50 mutations/Mb were seen in both responders and non-responders. When considering clinical variables, we noted a trend (not statistically significant) between aggressive histology subtypes and response to PD-1 therapy. Aggressive BCC subtypes may differ from low-risk subtypes in terms of PD-L1 expression and tumor infiltrating lymphocytes,43 44 as well as expression of p53, Bcl-2, and other molecular features,45–49 thus warranting further investigation of these aggressive subtypes, particularly in the context of immune response.
Going forward, future efforts should be pursued to better elucidate the role of PD-1 therapy in BCC. As PD-1 inhibition can lead to durable responses via activation of the antitumor immune response, and also is generally well tolerated, even among older patients, it would be worthwhile to understand how this approach can be combined with others. For patients with locally advanced, resectable BCC, who experience significant surgical morbidity and complexity, the use of neoadjuvant/adjuvant PD-1 inhibition together with surgery may have clinical advantages,50–52 and is being explored in clinical trials (NCT4323202). In the unresectable or metastatic setting, the combination of HHI with PD-1 has been explored in a proof-of-concept study,53 while other ongoing trials will also investigate PD-1 combined with other systemic therapies as well (NCT4679480, NCT3521830, NCT3767348).
We acknowledge the retrospective design, limited sample size and lack of biomarkers within this study. As noted earlier, another limitation of this study was the inability to obtain histological confirmation of tumor responses for patients with locally advanced disease, as used in prospective trials of both HHI and PD-1.15 31 Strengths of the study include participation from multiple institutions, and the inclusion of real-world patients. Given the very recent approval of this treatment approach for advanced and metastatic BCC, we believe these findings still prove clinically relevant and informative.
In conclusion, this retrospective, multi-institutional study provides real-world evidence to support the safety and efficacy of PD-1 in the treatment of advanced BCC. We advocate further incorporation of PD-1 inhibition into the care of patients with aggressive BCC, including both locally advanced and metastatic disease, as well as future studies to better understand the underlying mechanisms of antitumor immunity in this malignancy.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This retrospective study was approved by the institutional review board of the University of Southern California (approval# HS-16-00840-AM001) and was conducted in accordance with the principles of the Declaration of Helsinki in its current version.
Acknowledgments
The authors would like to thank the patients and their families, all investigators, and site personnel involved in the study. GKI was supported by the Cancer Center Support Grant (CCSG), award number P30CA014089, from the National Cancer Institute, and by the Southern California Clinical and Translational Institute (CTSI) grant, UL1TR001855 and UL1TR0001301, from the National Institutes of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Gino_K_In_USC
Contributors Conception, design: GKI, SC, GTG. Data analysis: GKI, SC. Writing of manuscript: GKI, SC, GTG. Collection of data: all authors. Manuscript editing and approval: all authors. Responsible for overall content as guarantor: GKI.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health.
Competing interests GKI reports having consulting/advisory board roles with Boehringer-Ingelheim, Novartis, BMS, Castle Biosciences, Regeneron, Sanofi; receiving research support from Regeneron, Array, Idera, Roche/Genentech, Replimune, Xencor, InstilBio, and having speaker roles for Merck. DYR reports having consulting/advisory board roles with Castle Biosciences. JCH reports having consulting/advisory board roles with Regeneron. All other authors have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.