Article Text

Abstract
Background Bellmunt Risk Score, based on Eastern Cooperative Oncology Group (ECOG) performance status (PS), hemoglobin levels and presence of liver metastases, is the most established prognostic algorithm for patients with advanced urothelial cancer (aUC) progressing after platinum-based chemotherapy. Nevertheless, existing algorithms may not be sufficient following the introduction of immunotherapy. Our aim was to develop an improved prognostic model in patients receiving second-line atezolizumab for aUC.
Methods Patients with aUC progressing after cisplatin/carboplatin-based chemotherapy and enrolled in the prospective, single-arm, phase IIIb SAUL study were included in this analysis. Patients were treated with 3-weekly atezolizumab 1200 mg intravenously. The development and internal validation of a prognostic model for overall survival (OS) was performed using Cox regression analyses, bootstrapping methods and calibration.
Results In 936 patients, ECOG PS, alkaline phosphatase, hemoglobin, neutrophil-to-lymphocyte ratio, liver metastases, bone metastases and time from last chemotherapy were identified as independent prognostic factors. In a 4-tier model, median OS for patients with 0–1, 2, 3–4 and 5–7 risk factors was 18.6, 10.4, 4.8 and 2.1 months, respectively. Compared with Bellmunt Risk Score, this model provided enhanced prognostic separation, with a c-index of 0.725 vs 0.685 and increment in c-statistic of 0.04 (p<0.001). Inclusion of PD-L1 expression did not improve the model.
Conclusions We developed and internally validated a prognostic model for patients with aUC receiving postplatinum immunotherapy. This model represents an improvement over the Bellmunt algorithm and could aid selection of patients with aUC for second-line immunotherapy.
Trial registration number NCT02928406.
- Immunotherapy
- Urinary Bladder Neoplasms
Data availability statement
Data are available upon reasonable request. The data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Immune checkpoint inhibitors are standard of care following progression on platinum agents in patients with advanced urothelial cancer, but tools for selection of patients likely to benefit are lacking. The only validated prognostic model in this setting, proposed by Bellmunt et al, was based on the use of postplatinum chemotherapy. Recent studies suggest that factors not included in this model may be important for the new treatment paradigm.
WHAT THIS STUDY ADDS
We describe the development and internal validation of a new prognostic model based on patients treated with atezolizumab in second-line setting. Our results suggest that the 3-factor (hemoglobin, Eastern Cooperative Oncology Group performance status, liver metastases) Bellmunt prognostic model can be significantly improved with the addition of alkaline phosphatase, neutrophil-to-lymphocyte ratio, bone metastases and time from last chemotherapy in a 4-tier model.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The model we are proposing incorporates easily accessible factors and could be used for patients’ counseling, physicians’ decisions and clinical trial stratification.
Introduction
Immune checkpoint inhibitors (ICIs) are standard therapies for advanced urothelial carcinoma (aUC) following progression on platinum-based chemotherapy.1 2 Despite rapid expansion of ICIs in the treatment of aUC, only 13%–24% of patients will derive a long-term benefit.3 There is therefore an unmet need for risk categorization of this population to aid risk-directed treatment selection and patients’ counseling in everyday practice but also to better stratify patients in clinical trials.
The Bellmunt model4 is the only validated prognostic model, which is based on a score derived from three adverse baseline factors (hemoglobin<10 g/dL, the presence of liver metastases and an Eastern Cooperative Oncology Group performance status (ECOG PS) of >0). While it achieves a satisfactory prognostic discrimination of patients with aUC relapsing after platinum-based chemotherapy, it was derived from treatment with chemotherapy. The few prognostic algorithms that have been developed in patients with aUC treated with ICIs have not been validated outside clinical trials5 or included a small number of patients and overall survival (OS) was not the primary outcome of their analyses.6 Thus, new prognostic profiles are needed to reflect the current treatment paradigm for aUC.
The prospective phase IIIb SAUL study (A study of atezolizumab in locally advanced or metastatic urothelila or non-urothelial carcinoam of the urinary tract, Clinical Trials Gov identifier: NCT 02928406), is the largest ‘real-world’ study in this setting.7 Since it more accurately reflects everyday practice than interventional, randomized trials,8 SAUL represents the ideal platform to study prognostic factors in ICI second-line therapy. In a subanalysis of this study,9 the Bellmunt algorithm was associated with prognostic significance for second-line or subsequent-line atezolizumab but other factors, such as time from last chemotherapy (TFLC), PD-L1 expression and use of perioperative chemotherapy, were also found to be significant. Other analyses have suggested the importance of neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII).6 10–12
This analysis aimed to develop and internally validate a novel prognostic model in patients with aUC treated with atezolizumab following progression on previous platinum-based chemotherapy, taking into consideration features of interest identified in recent analyses and not included in the Bellmunt algorithm.
Materials and methods
Study design and patients
Deidentified data from the SAUL database were provided by the sponsor (data cut-off on 16 September 2018). The database was not updated for the present analysis.
The SAUL study has been published.7 Briefly, SAUL (NCT02928406) was a single-arm phase ΙΙΙb study of atezolizumab in a real-world patient population with locally advanced or metastatic UC or non-UC of the urinary tract. Patients were required to have ECOG PS≤2 and disease progression during or following 1–3 prior treatments. Patients with treated central nervous system (CNS) metastases, autoimmune disease, concomitant corticosteroids or renal impairment were eligible. Prior treatment with an ICI was not allowed. Patients were excluded from the current substudy if they had pure non-urothelial histology and/or had not received prior cisplatin or carboplatin-based chemotherapy.
Atezolizumab 1200 mg was administered intravenously every 3 weeks, with a maximum follow-up of 4 years for disease progression and OS.
Immunohistochemical staining of PD-L1 expression was performed on formalin-fixed, paraffin-embedded tissues using VENTANA SP142 rabbit monoclonal antibody (VENTANA benchmark ULTRA reader).13
Statistical methods
Associations between clinical features and OS, calculated from the first day of atezolizumab treatment to death from any cause, was the primary outcome. Variables included in the univariate analysis are listed in online supplemental table S1. Univariate association between each covariate and clinical outcome (OS) was assessed by Cox proportional hazards model. SII was calculated according to platelet count multiplied by neutrophil count/lymphocyte count.11 All variables with a p<0.2 in the univariate analysis were selected for inclusion in the multivariate model. An initial multivariate Cox model was built by a backward selection method eliminating factors not statistically significant at the 5% level. Cut-offs for categorical variables with no established cut-offs were chosen according to the variables’ discriminatory ability.
Supplemental material
Our model was internally validated by generating 1000 bootstrap samples with replacement from our dataset that included all univariate variables with a p<0.2. A backward stepwise Cox regression procedure was applied to each sample with a removal criterion of p<0.05. The variables that remained in more than 70% of the bootstrap samples were included in the final risk model. Risk groups were created according to the number of unfavorable risk factors for each patient and analyzed by Kaplan-Meier. Calibration of the Cox model was graphically assessed.14 Effect modification was assessed by including all pairwise combinations of interaction terms in our model. The alternative measures of discrimination of Harrell’s c-index and Gönen & Heller statistic, which is insensitive to censoring, were also calculated.15 Adjustment for ‘optimism’, the tendency for a model to predict better on the data on which it was derived than on new data, was done via a bootstrap-based method (1000 replications). All but one covariate had a missing rate of <2% (PD-L1 expression, 6.7%). To account for missing data, the complete case analysis (CCA) method was considered likely to give unbiased results based on the data being ‘missing completely at random’, as assessed by Little’s χ2 test.16 To ensure minimal bias due to missing data, multiple imputation (MI) methods were also applied (number of imputations n=20 to achieve adequate efficiency for parameter estimates).17 Our imputation model included the dependent variable of status and variables with complete data (ECOG PS, previous lines of therapy, number of sites, smoking history, perioperative chemotherapy, prior therapy, TFLC) to estimate the sets of plausible values for the missing data. The type of imputation algorithm used was multivariate normal distribution. Diagnostics for MI used were the relative increase in variance, fraction of missing information and relative efficiency. All statistical analyses were done using Statistical software Stata/SE V.17.0 (StataCorp. 2021. College Station, Texas: StataCorp LLC).
Results
Of the 997 patients treated with atezolizumab in SAUL, 936 were eligible for inclusion in this analysis (online supplemental figure S1). Selected baseline characteristics are shown in online supplemental table S2. Median age was 68 years, 924 (99%) had pure UC, while 225 (24%) had non-bladder primary. At the time of database lock, after a median follow-up of 12.6 months, 515 patients (55%) had died, 468 (91%) due to UC. Median OS was 8.7 months, median progression-free survival 2.2 months and overall response rate 13.6%. Overall, 143 patients (15%) received poststudy therapy. None received enfortumab vedotin, sacituzumab govitecan or erdafitinib.

{kind=link}
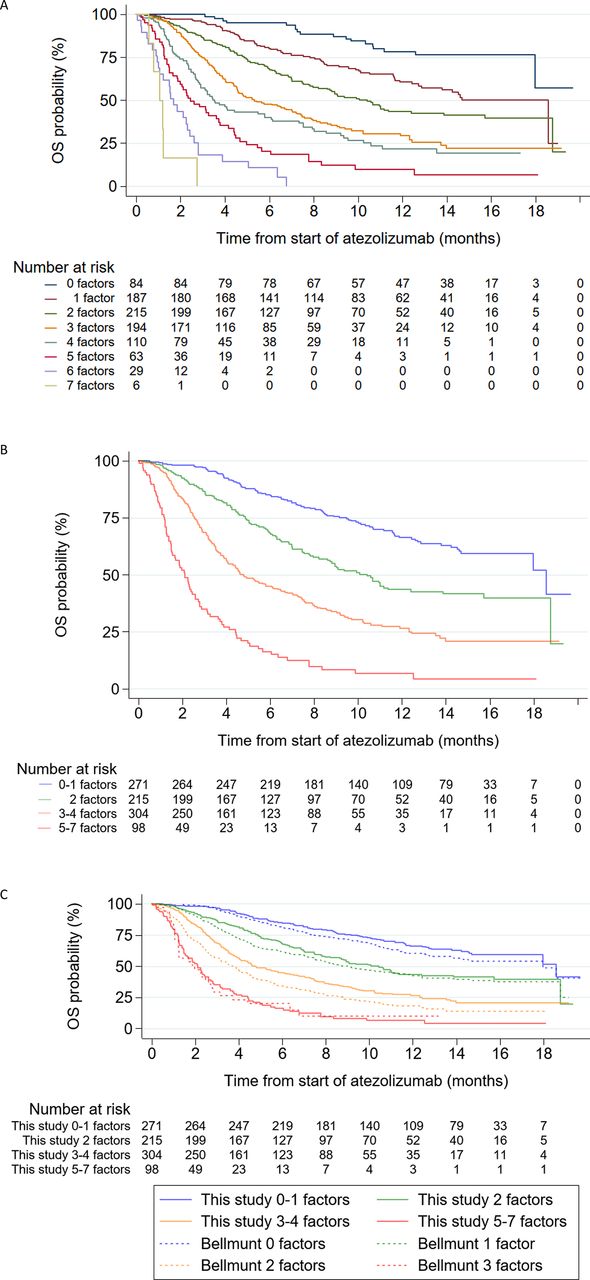
Association between OS and the following risk stratification: (A) an 8-tier risk model; (B) a 4-tier risk model; (C) a 4-tier risk model versus the Bellmunt risk factors. OS, overall survival.
Univariate Cox regression analysis
Univariate analyses of the 26 covariates and their effect on OS are presented in online supplemental table S3. Well-established clinical factors, such as ECOG PS and non-lymph node metastases, laboratory features including anemia and alkaline phosphatase (ALP), as well as all biological markers, that is, PD-L1 expression, NLR and SII, were associated with OS. The presence of mixed histology, CNS metastases, high aspartate transaminase levels and creatinine clearance ≤30mL/min were also correlated with OS, but were not studied further since only 12 (1%), 14 (1%), 45 (5%) and 41 (4%), respectively, of the 936 patients had these features. Expectedly, there was a strong positive correlation between NLR and SII (Spearman’s rho: 0.89, p<0.001). Therefore, inclusion of both in a multivariate model was redundant and NLR was chosen for simplicity since it only needs 2 instead of 3 covariates to be calculated. For NLR, a cut-off of 5 was chosen for further analysis because it was associated with the highest HR and is well established in the literature.5 6 18 The use of PD-L1 in modeling is hampered by variations in diagnostic assays, which cannot be cross-used.19 We, therefore, performed analyses with and without PD-L1 to investigate the possibility of omitting it without compromising the discriminatory ability of the model. Finally, there was a strong correlation between TFLC and time from diagnosis to treatment (Spearman’s rho: 0.307, p<0.001), of which TFLC was chosen to avoid multicollinearity.
Multivariate analysis
Overall, 828 and 888 patients had full data sets for the multivariate analyses with and without PD-L1 expression, respectively (table 1). In the resulting Cox proportional hazards models, all factors previously identified by the Bellmunt model, that is, ECOG PS, hemoglobin and liver metastases, were independent predictors of survival. TFLC, previously identified as an important prognostic factor,12 ALP, bone metastases and NLR were also retained in both models. Tumor–node–metastases stage at diagnosis was not retained in the model without PD-L1 expression.
Multivariate risk models and bootstrap validation
Bootstrap validation and model development
Bootstrap validation was performed on patients with complete datasets of the variables included in the multivariate analysis. The stepwise Cox regression procedure was employed with each of the 1000 random bootstrap samples with the same selection criteria as for the multivariate analysis. The frequency of each variable in the bootstrap samples was 5.8%–100% (table 2).
Frequency of a selection of variables (p<0.05) that remained in 1000 bootstrap samples following stepwise Cox procedure
As previously mentioned, only variables that remained in >70% of the bootstrap samples were included in the final models. In both models, seven variables, all previously identified in the multivariate analysis, were selected. Six (ECOG PS, NLR, ALP, liver metastases, TFLC and hemoglobin) were common in both models, while PD-L1 expression and bone metastases were the remaining factors in the models with and without PD-L1 expression, respectively. We refit the Cox model by using the variables selected in the 1000 bootstrap samples and calculated the regression parameters and HRs (table 1). The results of the bootstrap analyses were similar to the original multivariate models, suggesting successful internal validation. Using MI instead of CCA to account for missing data produced similar results (online supplemental table S4).
For the development of a risk score, each of the seven variables was assigned one point since the HRs were comparable. The 8-tier model produced a clear prognostic discrimination, with a similar c-index of 0.728 (95% CI: 0.705 to 0.751) and 0.725 (95% CI: 0.702 to 0.748) with or without PD-L1, respectively. The Bootstrap-based adjusted for optimism c-indices for the two models were also similar: 0.726 (95% CI: 0.702 to 0.75) and 0.723 (95% CI: 0.7 to 0.746), respectively. C-index remained essentially unchanged when the model not including PD-L1 was restricted to the 828 patients with PD-L1 information. Based on these results, we further studied the model, which did not include PD-L1 (figure 1A) due to the aforementioned practical issues associated with the use of PD-L1 in routine practice. Since some of the eight groups included small numbers of patients, the model was simplified into 4-risk categories according to the number of prognostic factors: 0–1, 2, 3–4, 5–7. The 4-risk categories maintained their prognostic discrimination, with a median OS of 18.6, 10.4, 4.8 and 2.1 months for 0–1, 2, 3–4 and 5–7 risk factors, respectively (figure 1B and table 3).
Median OS and 18-month OSR for the risk groups of Bellmunt stratification and the model developed in this study
Categorization of the Bellmunt risk factors (ECOG PS, hemoglobin, liver metastasis) in this study produced a c-index of 0.685 (95% CI: 0.662 to 0.708). Thus, the increment in c-statistic when using the new 7-factor model compared with the older 3-factor model was 0.04 (p<0.001), which is adequate to enhance the prognostic separation (figure 1C), according to previously published recommendations.19 Calibration of the risk scores revealed a generally good concordance between predicted and observed events at most time points (3, 6, 9, 12, 15, 18 months) (online supplemental figure S2).
Discussion
Few data on modeling in patients receiving modern immunotherapy for aUC exist. Sonpavde et al proposed a model based on ECOG PS, liver metastasis, platelet count, NLR (cut-off 5) and lactate dehydrogenase.5 The model showed good prognostic discrimination with a c-index of 0.692 which compared with 0.635 for the Bellmunt model. In a more recent study by Khaki et al,18 which included patients with aUC treated with first-line ICIs, ECOG PS≥2, albumin<3.5 g/dL, NLR>5 and liver metastases were identified as significant prognostic factors. The median OS of patients with 0, 1, 2, ≥3 risk factors was 23, 12, 7 and 2 months, respectively. The c-index was 0.68 vs 0.63 of the first-line algorithm developed by the MSKCC.20
Our results, along with those of Sonpavde and Khaki,5 18 strongly support the need for new risk stratification models in the era of immunotherapy in aUC. In all three studies, the models developed produced better discrimination than the models developed from patients not treated with immunotherapy. Our model showed a robust discrimination between prognostic groups using easily accessible and affordable factors and significantly improved the discriminatory ability of the Bellmunt algorithm. The information derived is clinically meaningful: for example, patients with five or more risk factors had a median OS of 2.1 months and might benefit from non-immunotherapy options. Differences in populations, agents used and line of therapy do not allow for meaningful comparison of our model with those reported by Sonpavde and Khaki.5 18 Nevertheless, taking into consideration their respective c indices of 0.692 and 0.68, our c-index of 0.725 appears robust and one of the highest reported in the literature. Our sample size is the largest among the three studies and we derived data from a phase IIIb study, which ensures better quality and reduced biases compared with the retrospective collection of data from medical files. At the same time, our patients reflect everyday practice more accurately than patients included in clinical trials. Moreover, Khaki reported a prognostic model in patients treated with first-line ICI but the role of ICIs as monotherapy in this setting is not clearly defined. On the other hand, postplatinum recommendations of ICIs are universal1 2 21 and, therefore, information included in the study of Sonpavde and in our study may be more relevant for current practice.
We used four clinical factors (ECOG PS, TFLC, liver and bone metastases), two biochemical factors (hemoglobin, ALP) and one biomarker (NLR) to develop a risk score. ECOG PS, hemoglobin and liver metastases are included in the Bellmunt algorithm, while the prognostic significance of TFLC is in concert with previous studies.9 22 23 Bone metastases have also been recently identified as adverse prognostic factor in patients treated with ICIs,24 25 while ALP has not, to the best of our knowledge, been described before. Although elevated ALP is related to the presence of liver and/or bone metastases, this factor was independently associated with OS and its inclusion in the model increased its discriminatory ability. NLR has been described as a useful marker in a variety of tumors,11 12 26 27 including a subgroup of patients in the SAUL study.10 It was also included in the models described by Sonpavde and Khaki.5 18 Higher NLR is considered a biomarker of inflammation commonly observed in advanced solid tumors and has been associated with poor response as well as shorter disease-free survival and OS in patients receiving neoadjuvant chemotherapy for bladder cancer.28 29 It is currently unknown whether NLR can be considered a surrogate of tumor (and/or host) biology and/or ICI responsiveness.
We are the first to use PD-L1 expression in a study aiming to develop a selection tool for patients treated with immunotherapy. PD-L1 has been identified as a potentially useful biomarker in aUC.13 Nevertheless, methodological issues create challenges in incorporating it in a selection tool to be applied to all ICIs currently used in aUC. In this context, our finding that its omission did not impact on the discriminatory ability of our model is reassuring regarding the applicability of our model in everyday practice. This finding should not discourage research efforts to identify biomarkers, which could be effectively incorporated in risk stratification of patients treated with ICIs.
Limitations include the retrospective nature of the study and therefore lack of randomization, with possible selection and confounding biases, missing data, lack of external validation and relatively short follow-up. Our patients also did not receive recently approved non-immunotherapy agents, which prolong survival.30–32 Thus, the value of this model in an environment of wide use of these agents is unknown. In addition, all patients received atezolizumab, which has had its indication following platinum therapy in the US withdrawn, and therefore the performance of this model in the presence of other ICIs is unclear. However, we hypothesize that the model would likely be applicable for any second-line ICI for aUC, given that these agents have demonstrated similar activity across trials. The fact that most of the factors included in our model have been found significant in patients who also received other ICIs supports this notion.
In conclusion, we developed and internally validated a new 4-tier risk score based on seven clinical and biological prognostic factors in patients with aUC receiving postplatinum ICI. External validation with other data sets is being actively pursued. This model can be easily incorporated into clinical practice to help guide therapy-related decisions and inform eligibility, stratification and ‘benchmarking’ for endpoint assessment into clinical trials for patients with aUC who are ICI candidates.
Data availability statement
Data are available upon reasonable request. The data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The trial was approved by the institutional review board or ethics committee at each participating site. All patients provided written informed consent. Due to the number of institutions, it has not been possible to include all of their reference numbers. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the patients participating in the trial and their families, the investigators, and F Hoffmann-La Roche for providing the clinical trial data from the SAUL study. Editorial support was provided by Katrin Gudmundsdottir, PhD (KG Medical Writing Ltd) funded by the HGUCG.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AB had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: AB and KT. Acquisition of data: AB, AM, YL, NJ, EC, DC, FL-R, FC, MK, GdV, RZ and CNS. Analysis and interpretation of data: AB, AM, YL, NJ, EC, DC, FL-R, FC, MK, GdV, RZ, KT and CNS. Drafting of the manuscript: AB and KT. Critical revision of the manuscript for important intellectual content: AB, AM, YL, NJ, EC, DC, FL-R, FC, MK, GdV, RZ, KT and CNS. Statistical analysis: AB and KT. Obtaining funding: AB. Administrative, technical or material support: AB. Supervision: AB.
Funding The SAUL trial was sponsored and funded by F. Hoffmann-La Roche, Basel, Switzerland. F Hoffmann-La Roche played a role in the design and conduct of the original study and in the collection, management, analysis, and interpretation of the original study data but had no involvement in the analysis reported in this manuscript. This sub-analysis of the SAUL trial was funded by the Hellenic Genito-Urinary Cancer Group (HGUCG). HGUCG provided support in the preparation of this manuscript but had no involvement in the design of the study or the collection, management, analysis and interpretation of the data.
Competing interests AB: Honoraria, advisory and research funding from Roche, BMS, MSD, Ipsen, Debiopharm, Basilea, Pierre Fabre and Janssen; and steering committee member for Roche. AM: Lectures/speaker honoraria from AstraZeneca, Bristol-Myers Squibb, Eisai, Ipsen, MSD, Merck Serono, Janssen, Takeda, TEVA, Astellas, Novartis, Pfizer and Roche; consultant for AstraZeneca, Astellas, Bristol-Myers Squibb, Ipsen, Janssen, EUSA Pharm, MSD, Merck Serono, Novartis, Takeda, Teva, Pfizer and Roche; research and clinical trials support from AstraZeneca, Astellas, Bristol-Myers Squibb, Ipsen, Janssen, EUSA Pharm, MSD, Merck Serono, Novartis, Takeda, Teva, Pfizer and Roche. YL: Personal fees from Roche, Janssen, Astellas, MSD, Pfizer, BMS, Immunomedics, AstraZeneca, Sanofi and Seattle Genetics; grants from Janssen, MSD and Sanofi; non-financial support from Janssen, Roche, AstraZeneca and Sanofi. NJ: Consultancy from Merck, Roche and AstraZeneca; trial funding (to institution) from Merck, Roche and AstraZeneca. EC: Research grants from Bio-Cancer, Biogen, Novartis, Pfizer, Roche, Sanofi and UCB; consultancy from Abbvie, Amgen, Biogen, Biocon, Chugai Pharma, Eli Lilly, Gilead, Janssen, Merck Serono, Novartis, Pfizer, Regeneron, Roche, R-Pharm and Sanofi; and speakers fees from Abbvie, Amgen, Bristol Myers Squibb, Chugai Pharma, Eli Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, Regeneron, Roche, Sanofi and UCB. DC: Personal fees for advisory boards/speaker engagements from Roche, Janssen, Astellas, MSD, Ipsen, Pfizer, Bristol-Myers Squibb, Bayer, AstraZeneca, Novartis, Lilly, Sanofi, Pierre Fabre and Boehringer Ingelheim. FL-R: Honoraria from AstraZeneca, Bayer, BMS, Lilly, MSD, Pfizer, Roche and Thermo Fisher; and research funding from Lilly, Roche and Thermo Fisher. FC: Advisory role for BMS, MSD, Pfizer and AstraZeneca. MK: Honoraria/consultation for Bayer, BMS, Eusai, Novartis, Merck, MSD, Pfizer and Roche; travel grants from Ipsen, Janssen, Merck and Novartis. GdV: Support for clinical trials and scientific projects for Pfizer, Roche and Ipsen; and speaker fees and consulting for Pfizer, Novartis, Roche, MSD, Astellas, Bayer, Ipsen, Janssen, Merck, EUSA Pharma and BMS. RZ: None. KT: None. CNS: Consultant for Pfizer, Merck, MSD, AstraZeneca, Astellas, Sanofi Genzyme, Roche-Genentech, Incyte, BMS, Foundation Medicine, Immunomedics (now Gilead), Medscape, UroToday, CCO Clinical, Janssen and NCI.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.