Article Text

Abstract
Background Stereotactic body radiotherapy (SBRT) induces immunogenic cell death, leading to subsequent antitumor immune response that is in part counterbalanced by activation of immune evasive processes, for example, upregulation of programmed cell death-ligand 1 (PD-L1) and adenosine generating enzyme, CD73. CD73 is upregulated in pancreatic ductal adenocarcinoma (PDAC) compared with normal pancreatic tissue and high expression of CD73 in PDACs is associated with increased tumor size, advanced stage, lymph node involvement, metastasis, PD-L1 expression and poor prognosis. Therefore, we hypothesized that blockade of both CD73 and PD-L1 in combination with SBRT might improve antitumor efficacy in an orthotopic murine PDAC model.
Methods We assessed the combination of systemic blockade of CD73/PD-L1 and local SBRT on tumor growth in primary pancreatic tumors, and investigated systemic antitumor immunity using a metastatic murine model bearing both orthotopic primary pancreatic tumor and distal hepatic metastases. Immune response was quantified by flow cytometric and Luminex analyses.
Results We demonstrated that blockade of both CD73 and PD-L1 significantly amplified the antitumor effect of SBRT, leading to superior survival. The triple therapy (SBRT+anti-CD73+anti-PD-L1) modulated tumor-infiltrating immune cells with increases of interferon-γ+CD8+ T cells. Additionally, triple therapy reprogramed the profile of cytokines/chemokines in the tumor microenvironment toward a more immunostimulatory phenotype. The beneficial effects of triple therapy are completely abrogated by depletion of CD8+ T cells, and partially reversed by depletion of CD4+ T cells. Triple therapy promoted systemic antitumor responses illustrated by: (1) potent long-term antitumor memory and (2) enhanced both primary and liver metastases control along with prolonged survival.
- Adenosine
- Radioimmunotherapy
- Gastrointestinal Neoplasms
- Tumor Microenvironment
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
CD73 is upregulated in pancreatic ductal adenocarcinoma (PDAC) compared with normal pancreatic tissue and high expression of CD73 in PDACs is associated with poor prognosis. The antitumor immune response stimulated by radiotherapy can be counterbalanced by immune suppressive effects, including radiation-induced upregulation of programmed cell death-ligand 1 (PD-L1) and adenosine generating enzyme CD73. However, whether blockade of both CD73 and PD-L1 in combination with stereotactic body radiotherapy (SBRT) improves antitumor efficacy in local and metastatic PDAC models remains to be elucidated.
WHAT THIS STUDY ADDS
Dual blockade of CD73 and PD-L1 greatly augmented local SBRT-induced antitumor efficacy in orthotopic PDAC murine models by modulating the immunosuppressive tumor microenvironment in PDAC toward a more immunostimulatory phenotype, which resulted in long-term antitumor memory. Importantly, local SBRT treatment of pancreatic cancer and systemic blockade of CD73 and PD-L1 enhanced control of liver metastases and prolonged survival.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
SBRT in combination with blockade of CD73 and PD-L1 could induce not only local but also systemic/abscopal antitumor immune responses in the PDAC model providing proof of principle for the translation of triple therapy in human PDAC.
Background
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive and deadly cancers, with a 5-year survival rate of approximately 11%.1 PDAC is predicted to be the second leading cause of cancer-related deaths in the USA by 2030.2 Surgical resection remains as the only curative treatment. However, over 80% patients present with locally advanced or metastatic disease at the time of diagnosis. The current standard of care, chemotherapy with FOLFIRINOX (5-fluorouracil, leucovorin, irinotecan, oxaliplatin) or gemcitabine/nab-paclitaxel, provides only modest improvement of effectiveness compared with gemcitabine single treatment.3 4 Therefore, new effective treatment strategies are greatly needed to improve survival in PDAC.
Immune checkpoint blockade (ICB) has shown promising benefits for patients in various solid tumors, especially those with high mutation burdens or programmed cell death-ligand 1 (PD-L1) expression.5–7 However, ICB with anti-cytotoxic T-lymphocyte antigen 4 (CTLA-4) or combination of anti-CTLA-4 and anti-PD-L1 has proven ineffective for patients with PDAC in clinical trials.8 9 The lack of ICB response is largely due to the unique PDAC tumor microenvironment (TME) which consists of a desmoplastic stroma with high density of immunosuppressive cells including myeloid derived suppressor cells (MDSCs), regulatory T cells (Tregs), tumor-associated macrophages (TAMs).10 In addition, low immunogenicity which is characterized as low tumor mutational burden in PDAC may also explain the ineffectiveness of ICB.11 12 Therefore, the current challenge is how to overcome the barriers of this immunosuppressive TME and convert them into immunostimulatory.
Strategies to circumvent these barriers using conventional cancer treatments to prime the immune response in combination with ICB are under active exploration. Among them, radiotherapy, especially a new generation of radiotherapy, such as stereotactic body radiotherapy (SBRT), appears to be a promising candidate due to its immunomodulatory ability, favoring local tumor control and even abscopal effect (non-irradiated and distant metastases).13 14 Our previous studies have shown that SBRT induces immunogenic cell death in PDAC, resulting in the release of damage-associated molecular patterns (DAMPs), which attract and activate dendritic cells, leading to subsequent adaptive immune responses.15–17 One previous preclinical study demonstrated that radiotherapy induced PD-L1 upregulation and PD-L1 blockade enhanced the response of PDAC to radiotherapy.18 Therefore, SBRT in combination with ICB immunotherapy, is a promising approach to modulate the immunosuppressive PDAC tumor towards one that is now immunostimulatory.
ATP, as an important DAMP released by irradiated cancer cells during immunogenic cell death, is rapidly hydrolyzed stepwise by CD39, converting ATP to AMP, and CD73, as the rate-limiting step of this enzymatic cascade, converting AMP to extracellular adenosine.19 20 ATP promotes inflammation via ATP receptors, whereas adenosine dampens inflammation via adenosine receptors. Adenosine, via interaction with specific receptors (A1, A2A, A2B or A3), enhances the suppressive function of immune cells, such as TAMs, MDSCs, and Tregs, and suppresses the protective immune cells such as T cells, natural killer (NK) cells.14 Therefore, CD73 and CD39, as adenosine-generating enzymes, have emerged as novel immune checkpoints.
CD73 is upregulated in PDAC compared with normal pancreatic tissue and high expression of CD73 in PDACs is associated with increased tumor size, advanced stage, lymph node involvement, metastasis, PD-L1 expression and overall poor prognosis.21 22 Furthermore, recent research showed that radiotherapy could increase CD73 and CD73 blockade in combination with radiotherapy and ICB improved the efficacy.23 CD73 blockade is currently being tested in combination with ICB, including anti-programmed cell death protein-1 (PD-1)/PD-L1 and anti-CTLA-4, with synergistic effects of this combined therapy being observed in preclinical models and clinical trials.24 25 Given that both CD73 and PD-L1 are radiation-induced checkpoints, we propose that blockade of both CD73 and PD-L1 in combination with SBRT might improve antitumor efficacy in PDAC models.
Here, we demonstrated that dual blockade of CD73 and PD-L1 in combination with SBRT resulted in superior local tumor control and survival when compared with untreated, monotherapy or dual combination of these therapies in orthotopic PDAC murine models. Triple therapy (SBRT+anti-CD73+anti-PD-L1) modulated the TME toward immunostimulatory based on the change of tumor-infiltrating immune cells and tumor cytokines/chemokines milieu. The beneficial effects of triple therapy were dependent mainly on CD8+ T cells and partially on CD4+ T cells. Importantly, local SBRT treatment of pancreatic cancer and systemic blockade of CD73 and PD-L1 enhanced liver metastases control. Together, these preclinical results suggest that dual blockade of CD73 and PD-L1 in combination of SBRT may be a promising strategy for PDAC treatment.
Methods
Cells and reagents
The murine PDAC KCKO and luciferase-expressing KCKO (KCKO-Luc) cell lines were provided by Dr Pinku Mukherjee (University of North Carolina, Charlotte, North Carolina, USA, 2010). Luciferase-expressing KP2 cells (KP2.1-Luc) were generated by transfecting the KP2 cells (provided by Dr David DeNardo, Washington University of Medicine, St. Louis, Missouri, USA, 2016) with luciferase-containing vectors. All cell lines were negative for Mycoplasma and cultured in RPMI1640 supplemented with 10% fetal bovine serum (FBS) and 1% penicillin/streptomycin. All cell lines used for experiments were within three passages of subsequent culture.
Anti-CD73 (2C5 mouse IgG1), anti-PD-L1 (clone 80) and related isotype IgG controls are provided by AstraZeneca. For in vivo experiments, 10 mg/kg of anti-CD73, anti-PD-L1 or isotype control IgG were administered by intraperitoneal injections (diluted in phosphate buffered saline (PBS), 100 µL per mouse) two times per week starting on 1 day before SBRT treatment. For CD4+ T cell, CD8+ T cell or neutrophil depletion, 200 µg of anti-CD4 (clone: YTS191), anti-CD8 (clone: 53–6.7), anti-Ly6G (clone: 1A8) or isotype IgG (diluted in PBS, 100 µL per mouse) were administered intraperitoneally every 3 days.
Murine orthotopic model and hepatic metastases model of pancreatic cancer
Female C57BL/6J mice, 6–8 weeks old, were purchased from Jackson Laboratory and allowed to acclimate in the institutional animal facility. All animal studies have been approved by the University Committee on Animal Resources at the University of Rochester Medical Center (Rochester, New York, USA). Orthotopic or hepatic metastases models were established as described previously with minor adjustments.16 17 In brief, for the orthotopic model, mice were anesthetized with isoflurane and injected in the tail of the pancreas with 2×105 KCKO-Luc cells or 5×104 KP2.1-Luc cells in a 1:1 PBS to Matrigel suspension. Two small titanium clips were placed on either side of the tumor for identification at the time of SBRT. For the hepatic rechallenge model, mice that cured primary pancreatic tumors after SBRT+anti-CD73+anti-PD-L1 treatment were rechallenged with a hemi-splenic injection of 5×105 KCKO-Luc cells in PBS to develop hepatic metastases. For the murine model with both orthotopic tumor and hepatic metastases, mice were injected in the hemi-spleen with 5×105 KCKO-Luc cells and injected in the tail of the pancreas with 2×105 KCKO cells.
SBRT treatment
As previously described,16 17 26 mice were anesthetized with isoflurane and transferred to a Small Animal Radiation Research Platform (XStrahl) equipped with a CT scanning device that is controlled by MuriPlan software. Pancreatic tumor was identified by a CT image based on two small titanium fiducial clips placed on either side of the tumor at the time of tumor injection. A dose of 6 Gy was delivered to the tumor for four consecutive days, precisely targeting the tumor and minimizing normal tissue radiation exposure.
Flow cytometry
Mouse tumors were minced and digested with 30% collagenase (30 min, 37oC). Single-cell suspensions were generated by passing tumor fragments resuspended in 5% FBS in PBS through 40 µm cell strainer. Single-cell suspensions were subsequently incubated with Fc (Fragment, crystallizable) receptor blocking solution followed by fluorophore-conjugated mouse antibodies (BD Biosciences or BioLegend). For cell surface staining, fluorescently labeled antibodies including anti-CD45-FITC(clone 30-F11), anti-CD45-PE-Cy5(clone 30-F11), anti-CD3-FITC(clone 145–2 C11), anti-CD4-APC-Cy5(clone GK1.5), anti-CD8-BV605(clone 53–6.7), anti-NK1.1-PE-Cy7(clone PK136), anti-CD11b-eFluor450(clone M1/70), F4/80-APC(clone BM8), anti-Ly6C-APC-Cy7(clone AL-21), anti-Ly6G-PE-Cy7(clone 1A8), anti-CD11c-PE-Cy7(clone HL3), anti-MHC-II(I-A/I-E)-PerCP-Cy5.5(clone M5/114.15.2), anti-CD69-APC(clone H1.2F3), anti-CD73-Alexa Fluor488(clone TY/23), anti-PD-L1-BV605(clone 10F.9G2), anti-CD103-APC(clone M290), anti-XCR1-BV421(clone ZET), anti-CD80-BV786(clone 16–10 A1), anti-CD86-BV510(clone PO3), anti-PD-1-BV711(clone J43), or anti-CTLA-4-APC-R700(clone UC10-4F10-11), were added to samples for 30 min at 4oC in the dark. For further intracellular staining, cells were washed with PBS supplemented with 5% FBS, fixed/permeabilized with an FoxP3/Transcription factor staining buffer set (eBiosciences), and stained with fluorescence-labeled mouse antibodies including anti-interferon (IFN)-γ-BV786(clone XMG1.2) and anti-FoxP3-APC(clone FJK-16s) for 30 min at room temperature in the dark. Stained cells were washed and resuspended in 5% FBS in PBS. Flow cytometry was performed on an LSR II, and data analyzed using FlowJo.
Immunohistochemical staining
The cleaved caspase-3, HMGB1, or HSP70-positive cells were determined by immunohistochemical staining as previously described.16 17 Briefly, the frozen sections of tumor tissue from KCKO-Luc bearing mice were stained with primary antibodies including cleaved caspase-3 (#9664S, Cell Signaling Technology), anti-HMGB1 antibody (ab18256, Abcam), or anti-HSP70 antibody (ab79852, Abcam), followed by horseradish peroxidase-labeled secondary antibody staining. DAB (3,3′-Diaminobenzidine) was applied as substrate and hematoxylin as counterstain. Positive cells were enumerated using a computerized Olympus DP80 imaging system. Ten randomly selected fields (×400, magnification) of each tumor tissue section were enumerated, and the means were reported.
Analysis of cytokines and chemokines by multiplexed magnetic Luminex assay
As previously described,17 tumor tissue samples were homogenized and digested with Lysis Buffer #11 (R&D Systems) containing protease inhibitors on ice for 1 hour. The samples were then centrifuged at 14,000 rpm for 20 min at 4oC, and supernatants were collected and then delivered to Eve Technologies Corporation (Calgary, AB. Canada) for cytokines/chemokines detection using multiplexed magnetic Luminex assay.
Adenosine analysis
Mice bearing KCKO-Luc tumors in the pancreas were treated with SBRT (6 Gy×4) on day 7–10 and anti-CD73 on day 6 and 10 post tumor implantation. Mice were sacrificed on day 11. Tumors were collected, weighed and snap frozen in liquid nitrogen into the tissue homogenizing CKMix tube (Fisher, cat# 50-154-2938). Samples were analyzed for adenosine using liquid chromatography-mass spectrometry.27
Statistical analysis
Statistical analyses were performed with GraphPad Prism V.9.3.1 software. Unless indicated, data are expressed as mean±SEM. For growth curve multiple comparison, one-way analysis of variance (ANOVA) was used, followed by a Bonferroni method adjustment. For survival curve multiple comparison, log-rank (Mantel-Cox) with Bonferroni adjustment was used. For other multiple group comparison studies, one-way ANOVA was used, followed by the Dunnett’s test for comparing experimental groups against the untreated group as a single control. For a single comparison between the two groups, the paired student t-tests were used. P value<0.05 or p<0.01 was considered to be significant.
Results
Radiation-induced upregulation of CD73 and PD-L1 on pancreatic cancer cells
The antitumor immune response stimulated by radiotherapy can be counterbalanced by immune suppressive effects, including radiation-induced upregulation of PD-L118 28 29 and adenosine generating enzymes, such as CD73.14 23 To investigate whether pancreatic cancer cells respond to radiation by upregulation of PD-L1 and CD73, we treated mouse PDAC cell lines KCKO and KP2 with 15 Gy and analyzed the expression of CD73 and PD-L1 at different time points after radiation. As shown in online supplemental figure 1, mean fluorescence intensity of CD73 and PD-L1 significantly increased in the radiation-treated KCKO and KP2 cells compared with the untreated control. To further confirm the effect of radiation on expression of CD73 and PD-L1 in vivo, we treated mice bearing KCKO-Luc orthotopic pancreatic tumors with SBRT (6 Gy×4, on day 7, 8, 9 and 10 post tumor implantation) and analyzed expression of CD73 and PD-L1 on tumor cells on day 11 (1 day after SBRT). Shown in online supplemental figure 2, both CD73 and PD-L1 significantly increased in the SBRT group compared with untreated. These data demonstrated that radiotherapy induces these immunosuppressive pathways suggesting that blockade of both CD73 and PD-L1 may improve the antitumor efficacy of SBRT.
Supplemental material
Supplemental material
Blockade of CD73 and PD-L1 amplifies antitumor efficacy of SBRT in murine orthotopic PDAC models
To determine whether blockade of CD73 and/or PD-L1 can improve the antitumor efficacy of SBRT, we use two murine PDAC orthotopic models, KCKO-Luc, a luciferase-expressing cell line, derived from spontaneous PDAC tumor in p48-Cre/LSL-KrasG12D mice and KP2-Luc, derived from PDAC tumors in p48-Cre/LSL-KrasG12D/p53flox/+ mice. Blockade of CD73 was effective at reducing the intratumoral concentration of adenosine in both untreated and SBRT treated tumor-bearing mice (figure 1A). Tumor bearing mice were divided into eight groups: no treatment, anti-CD73, anti-PD-L1, anti-CD73+anti-PD-L1, SBRT (6 Gy×4), SBRT+anti-CD73, SBRT+anti-PD-L1 or combination of SBRT, anti-CD73 and anti-PD-L1 as shown in figure 1B. In the KCKO model (figure 1C–E), compared with no treatment, anti-CD73+anti-PD-L1, SBRT+anti-PD-L1, or triple therapy (SBRT+anti-CD73+anti-PD-L1) significantly reduced tumor growth; triple therapy has significantly better antitumor effect than SBRT or SBRT+anti-PD-L1, with 60% survival in the triple therapy compared with 30% survival in SBRT+anti-PD-L1. Similarly, in the KP2 model (figure 1F–H), triple therapy achieved enhanced tumor control and survival, compared with no treatment or SBRT groups, with enhanced tumor growth control and a trend of improved survival (66.7% in triple therapy and 40% in SBRT+anti-PD-L1) when compared with SBRT+anti-PD-L1 group. These data demonstrated that the combination of SBRT, anti-CD73 and anti-PD-L1 could be a promising strategy to treat pancreatic cancer.
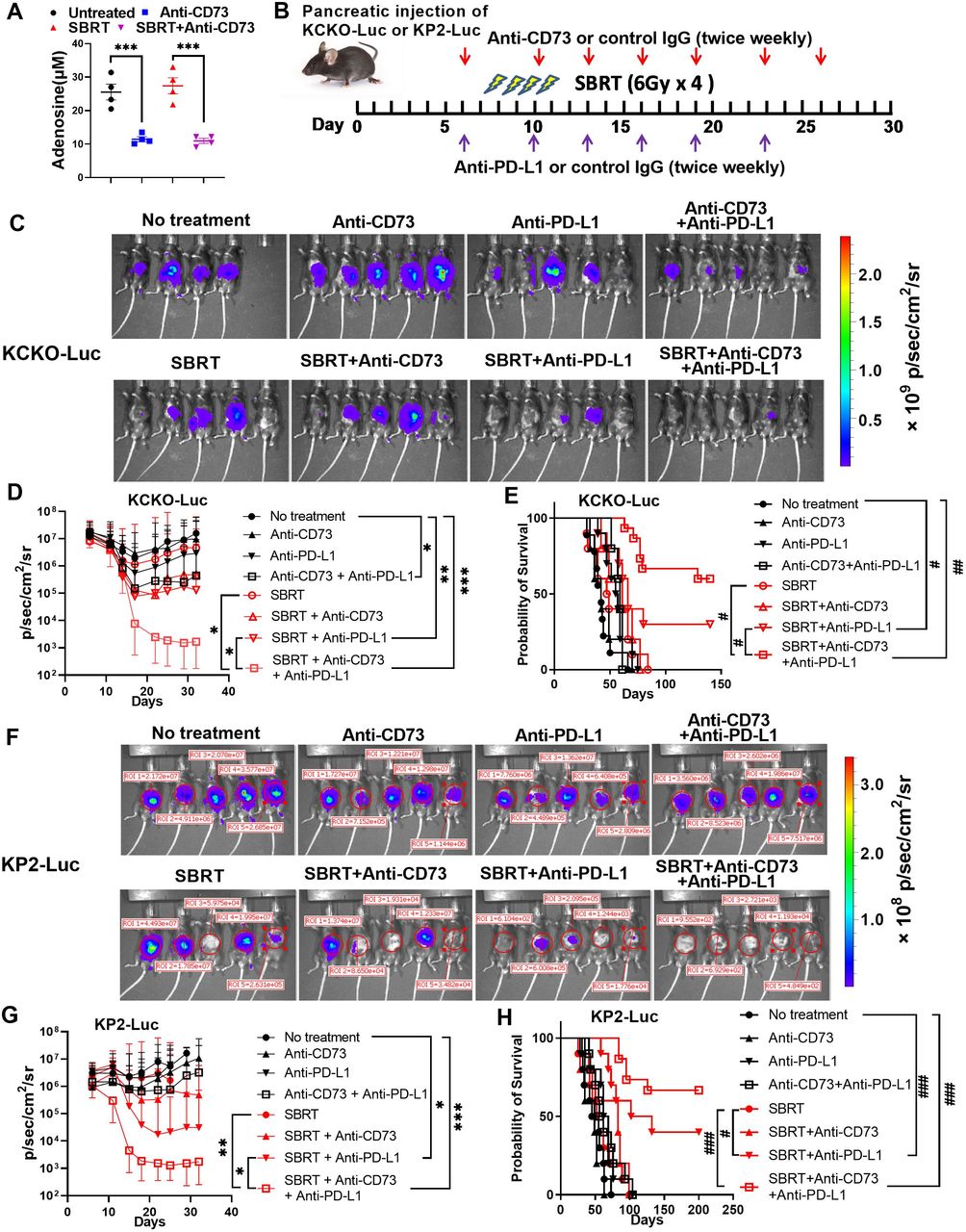
Blockade of CD73 and PD-L1 significantly enhances the antitumor efficacy of SBRT in the murine orthotopic model of pancreatic cancer. (A) Blockade of CD73 decreases adenosine in mice pancreatic ductal adenocarcinoma tumor. Mice bearing KCKO-Luc in pancreas were treated with SBRT (6 Gy×4) on day 7–10 and anti-CD73 on day 6 and 10 post tumor implantation. Mice were sacrificed on day 11. Tumors were collected, and adenosine was analyzed using liquid chromatography-mass spectrometry.27 Results were expressed as mean±SEM from four mice/group and analyzed by one-way analysis of variance (ANOVA) with Dunnett’s post test. ***, p<0.001. (B) Schematic of the experimental design. C57BL/6J mice were injected with KCKO-Luc or KP2-Luc cells in the tail of pancreas and treated with SBRT, anti-CD73, or anti-PD-L1 or combinations of two or three of these. Tumor growth was analyzed by IVIS two times a week. (C) and (F) Representative IVIS images from day 18 after KCKO-Luc2 or KP2-Luc (F) implantation. (D) and (G) Tumor growth curves in KCKO-Luc (D) or KP2-Luc (G) were determined by IVIS imaging. Data shown are geometric mean of IVIS value±SD from 10 to 15 mice/group. (E) and (H) Kaplan-Meier survival curves of mice bearing KCKO-Luc (E) or KP2-Luc (H) were observed. *, adjusted p<0.05, **, adjusted p<0.01, ***, adjusted p<0.001, analyzed by one-way ANOVA with multiple comparison (adjusted by Bonferroni method) for growth curve. #, adjusted p<0.01, ##, adjusted p<0.001, ###, adjusted p<0.0001, analyzed by log-rank (Mantel-Cox) test with multiple comparison (adjusted by Bonferroni method) for survival curve. IVIS, in vivo imaging system; KCKO-Luc, luciferase-expressing KCKO; KP2-Luc; luciferase-expressing KP2 cells; PD-L1, programmed cell death-ligand 1; SBRT, stereotactic body radiation therapy.
Radiotherapy-induced immunogenic cell death is enhanced by blockade of PD-L1, not CD73
Our previous work has shown that SBRT can induce immunogenic cell death (ICD) in both KCKO and KP2 orthotopic PDAC models.16 17 We investigated whether blockade of CD73 and/or PD-L1 can enhance ICD induced by SBRT. Tumors (KCKO model) from different treatment groups (day 14 post tumor implantation) were examined for expression of cleaved caspase-3 (apoptotic cell death marker, figure 2A), or two DAMP markers HMGB1 (figure 2B) and HSP70 (figure 2C) by immunohistochemistry. SBRT alone could induce increased ICD. Blockade of PD-L1, but not CD73, induced increased ICD in combination with SBRT. In addition, triple therapy (SBRT+anti-PD-L1+anti-CD73) did not further enhance ICD induced by SBRT+anti-PD-L1. Collectively, only anti-PD-L1 further enhanced the SBRT-induced ICD.
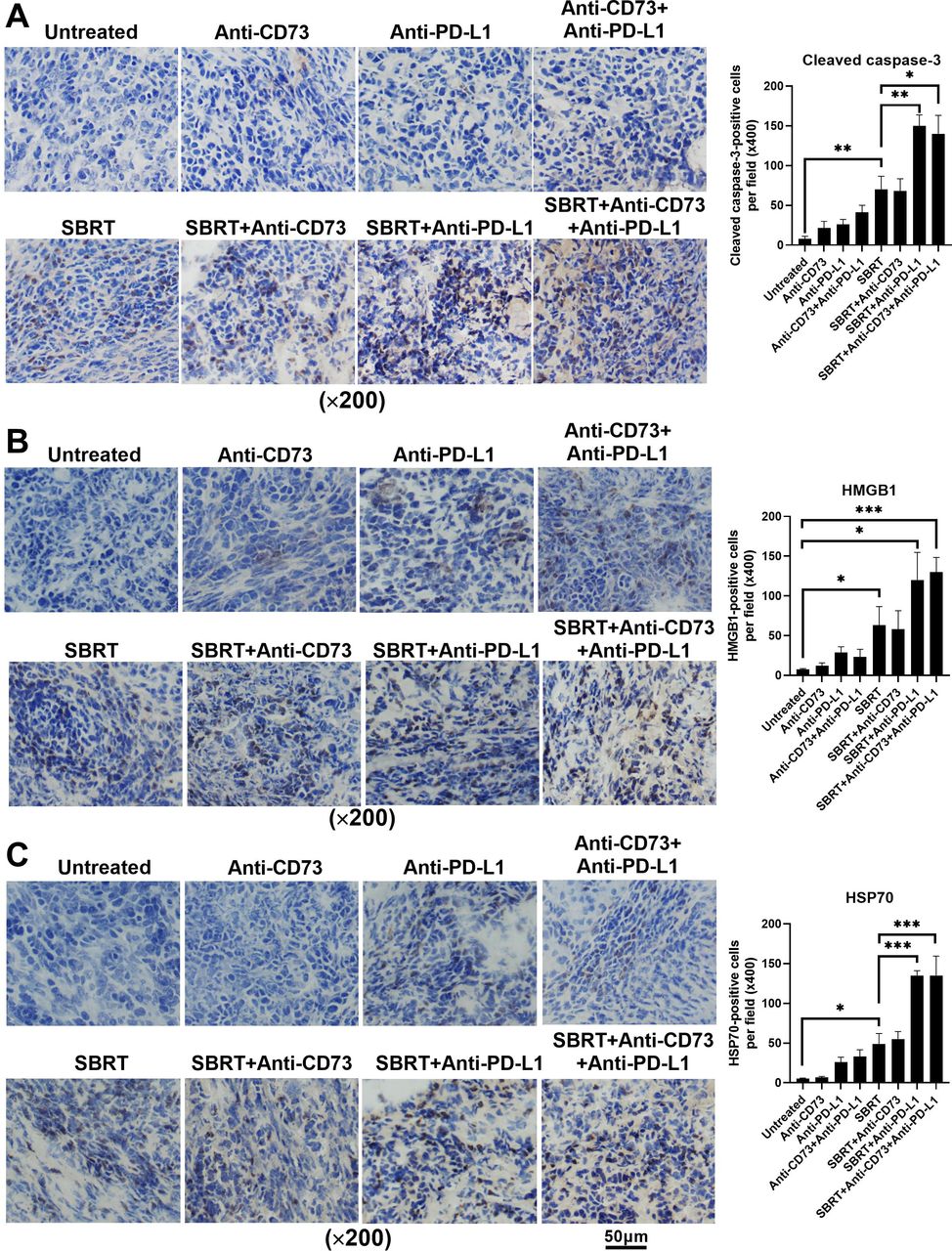
Blockade of PD-L1, but not CD73 induced increased ICD in combination with SBRT in the orthotopic model of murine pancreatic cancer. Mice bearing KCKO-Luc orthotopic tumors were treated with SBRT, anti-CD73 or anti-PD-L1, and ICD was determined by immunohistochemistry staining of cleaved caspase-3, HMGB1, and HSP70. Results are expressed as the mean±SEM from five mice per group and analyzed by one-way analysis of variance with Dunnett’s post test. *, p<0.05, **, p<0.01, ***, p<0.001, compared with the untreated group or monotherapy group. ICD, immunogenic cell death; KCKO-Luc, luciferase-expressing KCKO cells; PD-L1, programmed cell death-ligand 1; SBRT, stereotactic body radiation therapy.
Triple therapy modulates intratumor immune populations
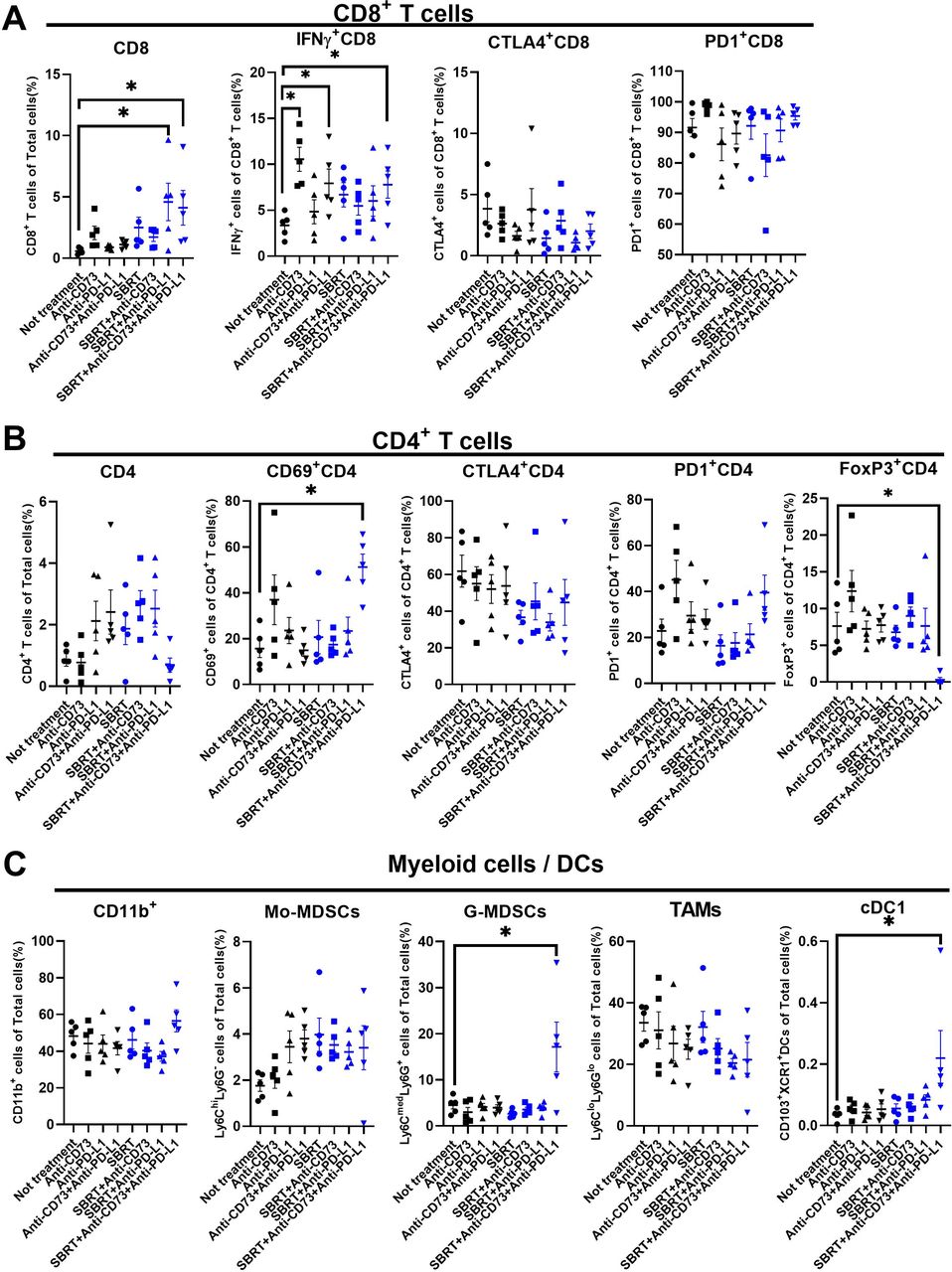
To determine the impact of SBRT/anti-CD73/anti-PD-L1 on the tumor immune microenvironment, we assessed the change in tumor-infiltrating immune cells by flow cytometry at day 14, which is 1 day after the third dose of anti-CD73+anti-PD-L1. We determined that not only were CD8+ T cells significantly increased in SBRT+anti-PD-L1 and triple therapy groups, these cells also exhibited heightened IFN-γ in the anti-CD73, anti-CD73+anti-PD-L1, and triple therapy groups (figure 3A, online supplemental figure 4). Triple therapy also increased CD69+CD4+ T cells (figure 3B, online supplemental figure 4). Of note, although anti-CD73 alone increased IFN-γ+CD8+ T cells, it also induced a trend of increase in PD-1+CD4, which may partially explain why anti-CD73 alone has no antitumor effect (figure 3B). Triple therapy also induced a significant increase of granulocytic myeloid derived suppressor cells (G-MDSCs) and type 1 classical dendritic cells in tumor (figure 3C). Additionally, we observed a significant increase of activation of CD8 and CD4 positive T cells in the spleen (online supplemental figure 3) following triple therapy, suggesting that triple therapy may induce a systemic antitumor immune response.
Supplemental material
Supplemental material

Triple therapy with SBRT, anti-CD73 and anti-PD-L1 enhances antitumor immune response in the orthotopic model of murine pancreatic cancer. Mice bearing luciferase-expressing KCKO cells orthotopic pancreatic cancer were treated as in figure 1 and sacrificed on day 14. Tumor-infiltrating immune cells were determined by flow cytometry. (A) Tumor-infiltrating CD8+ T cells and their expression of IFN-γ, CTLA-4, and PD-1 were analyzed. (B) Tumor infiltrating CD4+ T cells and their expression of CD69, CTLA-4, PD-1, and FoxP3 were analyzed. (C) Tumor-infiltrating CD11b+ cells, Mo-MDSCs, G-MDSCs, TAMs and cDC1 cells were analyzed. Results are expressed as mean±SEM from five mice per group and analyzed by analysis of variance with Dunnett’s post test. Significance is indicated by *, p<0.05. cDC1, type 1 classical dendritic cells; CTLA-4, cytotoxic T-lymphocyte antigen 4; DC, dendritic cell; G-MDSC, granulocytic myeloid derived suppressor cell; IFN-γ, interferon-γ; Mo-MDSCs, monocytic myeloid derived suppressor cells; PD-1, programmed cell death protein-1; PD-L1, programmed death ligand-1; SBRT, stereotactic body radiotherapy; TAMs, tumor-associated macrophages.
CD8+ T cells are critical for the antitumor effect in the orthotopic PDAC model
To evaluate the impact of CD8+ T cells, CD4+ T cells and G-MDSCs in the triple therapy-mediated immune response, cell depletion with antibodies against these cell populations was performed in the orthotopic KCKO-Luc PDAC model. Depletion of CD8+ T cells completely abrogated treatment efficacy (figure 4) whereas depletion of CD4+ T cells partially diminished the antitumor efficacy of triple therapy (figure 4). Depletion of G-MDSCs led to a trend of enhanced antitumor effect however with no significant difference (figure 4). These data suggest that T cells, especially CD8+ T cells, are essential to mediate the antitumor efficacy of triple therapy.
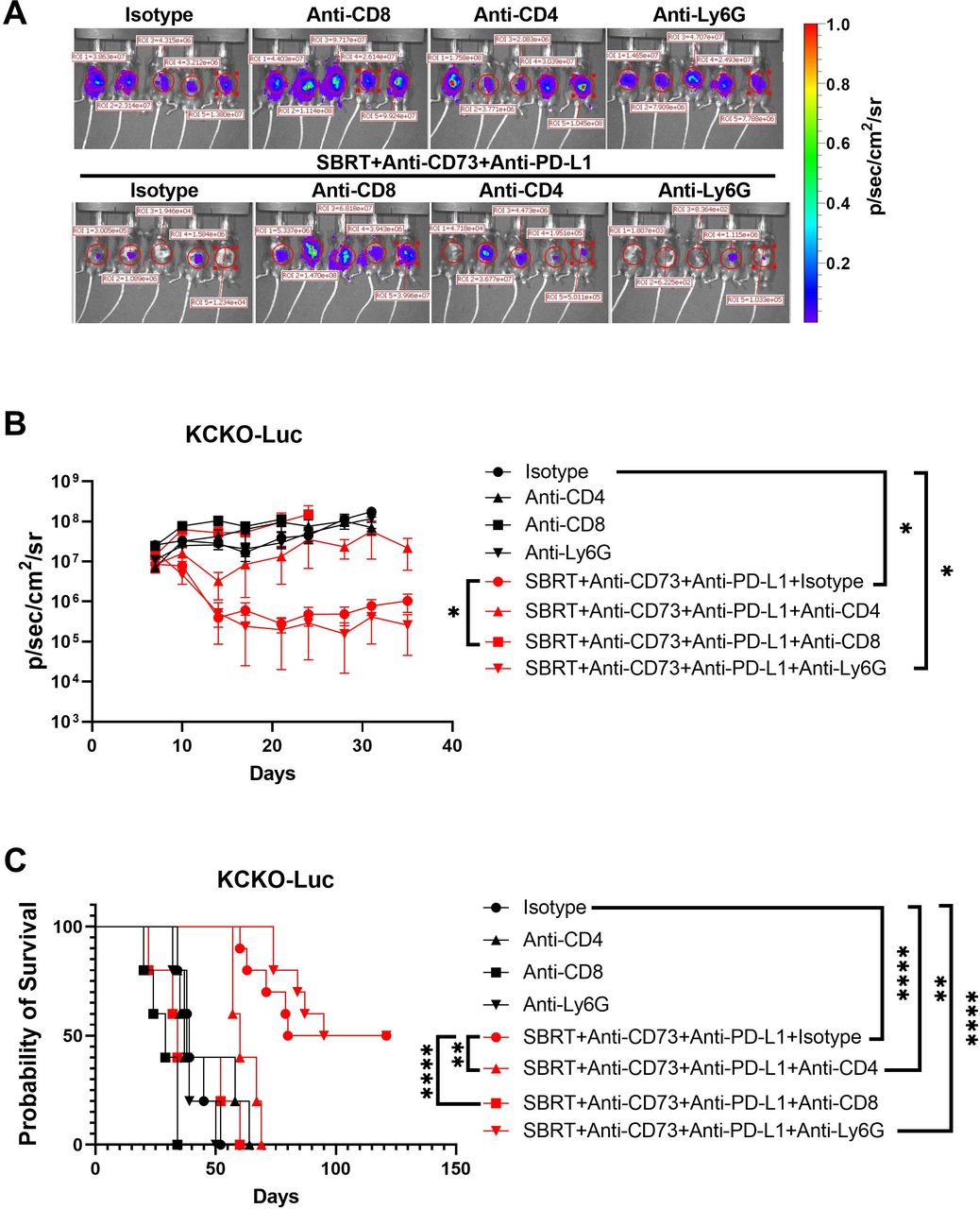
CD8+ T cells are critical for the antitumor effect in the orthotopic pancreatic ductal adenocarcinoma model. KCKO-Luc tumor-bearing mice were treated with SBRT+anti-CD73+anti-PD-L1 as in figure 1. Mice were given isotype or antibodies against CD8, CD4 or Ly6G to deplete CD8+ T cells, CD4+ T cells, or granulocytes, respectively. Tumor growth was measured by IVIS and survival observed. (A) Representative of IVIS on day 17 post tumor injection. (B) Tumor growth curve. Data are represented as geometric mean±SD (n=5 for each group). *, p<0.05. (C) Survival. **, p<0.01, ***, p<0.001, ****, p<0.0001. ROI, region of interest; IVIS, in vivo imaging system; KCKO-Luc, luciferase-expressing KCKO cells; PD-L1, programmed cell death-ligand 1; SBRT, stereotactic body radiotherapy.
Triple therapy modulates intratumor cytokine/chemokine profiles
The change of intratumoral cytokines and chemokines after therapy was assessed using Luminex technology on day 14 post tumor implantation (figure 5A). Triple therapy induced a significant decrease of several protumor, predominately myeloid-derived factors including interleukin (IL)-6, IL-7, LIF(leukemia inhibitory factor), LIX(Lipopolysaccharide-induced CXC chemokine), MCP-1(Monocyte chemoattractant protein-1), MIP(Macrophage Inflammatory Protein)-1α/β, and VEGF(Vascular endothelial growth factor), (figure 5B,C, online supplemental figure 5). These data indicate that triple therapy shifts TME toward a more immunostimulatory phenotype mainly through the downregulation of inhibitory factors.
Supplemental material

Triple therapy modulates intratumor cytokine/chemokine profiles. The change of intratumoral cytokines and chemokines after therapy was assessed using Luminex technology on day 14 post tumor implantation. (A) Fold changes of cytokines and chemokines in the tumor following treatment of SBRT/anti-CD73/anti-PD-L1. The levels of cytokines and chemokines of tumors from no treatment groups were set as 1, and data were fold changes as compared with untreated groups. (B) and (C) IL-6, IL-7, LIF, LIX, MCP-1, MIP-1α, MIP-1β, and VEGF. Results are expressed as mean±SEM from five mice per group and analyzed by one-way analysis of variance with Dunnett’s post test. Significances are indicated by *, p<0.05, and **, p<0.01, ***, p<0.001, compared with the untreated group. IFN, interferon; IL, interleukin; PD-L1, programmed cell death-ligand 1; SBRT, stereotactic body radiotherapy; MCP-1, Monocyte chemoattractant protein-1; LIF, leukemia inhibitory factor; LIX, Lipopolysaccharide-induced CXC chemokine; MIP-1, Macrophage Inflammatory Protein 1; VEGF, Vascular endothelial growth factor.
Triple therapy resulted in long-term antitumor memory and liver metastatic tumor control
Given that triple therapy could illicit T-cell activation in the spleen (online supplemental figure 3), we proposed that triple therapy can induce not only local but also systemic antitumor responses. To test that hypothesis, mice cured of KCKO orthotopic pancreatic tumor by triple therapy (figure 1) for at least 90 days were confirmed by in vivo imaging system as tumor free and then rechallenged with a hemi-splenic injection, which facilitates liver metastases, of KCKO-Luc cells. Shown in figure 6A,B, age-matched naïve mice developed liver metastases well after hemi-splenic injection. However, mice cured by therapy were completely refractory to metastatic rechallenge, suggesting that triple therapy results in long-term systemic antitumor memory capable of rejecting liver tumors. We then determined if triple therapy could control established liver metastases using a mouse model bearing both orthotopic KCKO (unlabeled) primary pancreatic tumor and metastatic KCKO-Luc tumors in liver (figure 6C). Mice received SBRT only at pancreatic tumor site but systemic anti-CD73 and anti-PD-L1 (figure 6C). As shown in figure 6D,E, anti-PD-L1 and anti-CD73+anti-PD-L1 significantly slowed down hepatic tumor growth compared with the untreated group but did not promote survival. In contrast, both SBRT+anti-PD-L1 and triple therapy significantly delayed hepatic tumor growth compared with untreated or SBRT groups, however only triple therapy (not SBRT+anti-PD-L1) improved survival when compared with the SBRT group. In addition, the triple therapy demonstrated a trend of enhanced liver tumor control and survival compared with SBRT+anti-PD-L1. Together, these data demonstrated that systemic blockade of CD73 and PD-L1 in combination with local SBRT treatment could induce a systemic antitumor response resulting in enhanced metastatic tumor control.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Local SBRT treatment of pancreatic cancer and systemic blockade of CD73 and PD-L1 enhanced liver metastasis control. (A) and (B) mice that were cured by SBRT+anti-CD73+anti-PD-L1 in figure 1 were refractory to tumor rechallenge. Mice cured by triple therapy (SBRT+anti-CD73+anti-PD-L1) and aged matched naïve mice received 5×105 KCKO-Luc cells by hemi-splenic injection. Tumor growth was analyzed by IVIS. (A) Representative of IVIS on day 7 post injection. (B) Growth curve of tumor liver metastasis. *, p<0.05, by multiple t-tests. (C) Schematic of mice orthotopic pancreatic cancer and hepatic metastasis establishment and treatment. (D) The growth of liver metastases analyzed by IVIS and the value of IVIS on day 6 set as one. Results are expressed as the mean of folds change of IVIS value±SEM from 10 to 15 mice/group. The significance was analyzed by one-way analysis of variance with multiple comparison (adjusted by Bonferroni method). (E) Survival. The significance was analyzed using a log-rank (Mantel-Cox) test (adjusted by Bonferroni method). i.p., intraperitoneal; IVIS, in vivo imaging system; KCKO-Luc, luciferase-expressing KCKO cells; PD-L1, programmed cell death-ligand 1; SBRT, stereotactic body radiation therapy.
Discussion
As the immunosuppressive PDAC TME is a major obstacle for ICB response, converting an immunosuppressive TME into a more inflammatory and immunogenic TME with SBRT appears to be a promising strategy to reactivate the host immune system and increase ICB response. However, this inflammatory response induced by SBRT may not be durable since an immunosuppressive cascade can also be triggered by SBRT.30 31 One such mechanism is generating immunosuppressive adenosine from extracellular ATP released from irradiated tumor cells. We demonstrated that systemic administration of anti-CD73 and anti-PD-L1 greatly augmented local SBRT-induced antitumor efficacy in both mouse orthotopic and metastatic models. Moreover, this triple therapy also generates a long-term systemic antitumor immune response, thereby providing a promising strategy for PDAC treatment.
CD73, as a speed-limiting ectonucleotidase, attenuates tumor immunity via cooperating with CD39 to generate immunosuppressive adenosine. Our data showed that anti-CD73 alone did not achieve a significant antitumor response, which is consistent with other reports,23 32 supporting the use of this reagent in combination with other therapies (such as anti-PD-L1 and SBRT).
Radiotherapy can upregulate the expression of CD73 on PDAC tumor cells representing a potential therapeutic target to be combined with radiotherapy. Improved antitumor efficacy with the combination of radiotherapy and CD73 blockade has been demonstrated in non-PDAC tumors.33 However, it is unclear whether blockade of CD73 can enhance radiotherapy efficacy in PDAC. Recently, one report showed that combination therapy of radiofrequency ablation (RFA) and a small molecule CD73 inhibitor AB680 reduced tumor growth and enhanced antitumor immune responses in a subcutaneous syngeneic PDAC model.34 In the current study, CD73 expression of PDAC tumor cells was upregulated following radiation in vitro or SBRT in vivo, which is consistent with other reports.35 36 However, in contrast to the earlier report using AB680,34 we observed no synergic effect between SBRT and anti-CD73 as well as no significant change of immune cells and cytokine/chemokines profiles in the tumor. This inconsistency is likely due to the different models: subcutaneous versus orthotopic and different treatments: RFA (1.82 W over 10–20 s) versus SBRT (6 Gy×4).
Another mechanism limiting the SBRT-induced antitumor immune response is the upregulation of PD-L1 on tumor cells following SBRT.18 28 SBRT-induced IFN-γ, mainly from activated CD8+ T cells, was demonstrated to be responsible for upregulation of tumor cell PD-L1 expression.18 28 Concurrent blockade of PD-L1 with SBRT augments the generation of durable systemic antitumor immune responses.18 28 In accordance with these reports, we observed that PD-L1 expression was upregulated by radiotherapy (SBRT) and SBRT in combination with anti-PD-L1 modestly improved the antitumor response compared with untreated or SBRT alone. The efficacy of this combination is associated with increased tumor-infiltrating CD8+ T cells and IFN-γ+CD8+ T cells (trending), demonstrating that addition of anti-PD-L1 can enhance T-cell recruitment and activation.18 28
The combination of CD73 blockade and other ICB is reported in clinical and preclinical studies.24 25 Given both CD73 and PD-L1 expression were upregulated on SBRT treatment, we hypothesized that dual blockade of both radiation-induced checkpoints, CD73 and PD-L1, may enhance SBRT-induced antitumor efficacy. To the best of our knowledge, this is the first preclinical study testing the efficacy of SBRT+anti-CD73+anti-PD-L1 in a PDAC model. We confirmed the importance of T cells in this model through immune cell depletion assays as CD8+ T cells were essential with CD4+ T cells partially mediating the response. Interestingly, we also observed a significant increase of G-MDSCs in tumors after triple therapy. Our group and others have shown that targeting G-MDSCs could enhance chemotherapeutic and immunotherapeutic responses in PDAC.37 38 However, in the current study, depletion of this population with anti-Ly6G did not significantly enhance the triple therapy-induced antitumor effect, suggesting triple therapy might induce a partial reversal of the immunosuppressive nature of this population.
Chemotherapy or chemoradiotherapy followed by anti-PD-1/PD-L1 and anti-CD73 or CD73 inhibitor have shown promising results in clinical trials including in patients with PDAC.25 39 We also tested the efficacy of chemotherapy in combination (sequentially) with blockade of CD73 and PD-L1 in the PDAC model. Our data showed that chemotherapy (gemcitabine/nab-paclitaxel)+anti-CD73+anti-PD-L1 resulted in improved tumor control than chemotherapy alone or anti-CD73+anti-PD-L1, leading to prolonged survival (online supplemental figure 6). However, no mouse survived past 75 days following chemotherapy+anti-CD73+anti-PD-L1 whereas SBRT+anti-CD73+anti-PD-L1 combination resulted in over 60% mice surviving well past 150 days (presenting as cures). Thus, in this preclinical model of PDAC, SBRT appears to be a better candidate than chemotherapy to be combined with this regime of immunotherapy. This may be due to the ability of SBRT to modulate the immune system by inducing ICD.16 17
Supplemental material
Accumulating evidence indicates that local radiotherapy can induce a systemic antitumor effect (regression of tumor in distant unirradiated sites), although the clinical cases of abscopal effects are rare.40 SBRT, as a modern radiotherapy technique, can deliver a few fractions of high doses per fraction to a small target volume enhancing the potential to generate heightened systemic immune response.41 However, SBRT also induced higher expression of CD73 and PD-L1 in the PDAC mouse model, which may partially explain why SBRT alone has limited abscopal effect in our liver metastatic model. CD73 blockade enhances the local and systemic tumor control (asbcopal effect) of radiotherapy in murine rectal cancer model32 and mammary carcinoma.23 However, similar as in our orthotopic PDAC model, CD73 blockade in combination with SBRT did not improve the liver metastatic tumor control, again indicating additional therapy is required to reverse the strong immunosuppressive TME in PDAC. The abscopal response has been more frequently observed in patients receiving the combination of radiotherapy and immunotherapy in various tumors.42 43 The combination of radiotherapy and ICB has been explored in PDAC in a clinical trial,44 but no abscopal effect has been reported thus far. One preclinical study demonstrated a significant delay in tumor growth in a model where pre-irradiated PDAC cells were injected into the liver and treated with anti-PD-L1. Although this was not a perfect abscopal model, the authors claimed the possible systemic/abscopal effect for combination of SBRT and anti-PD-L1(18). In another preclinical PDAC study, two subcutaneous KPC tumors were established on both flanks with only one tumor receiving irradiation. Radiotherapy in combination with ICB did not affect the growth of the unirradiated tumor or prolong survival, and additional immunomodulatory treatment with anti-CD40 was required to overcome the immunosuppressive PDAC.45 In contrast, in our clinically relevant mouse model bearing both tumor in the pancreas (radiated) and liver (unirradiated), combining SBRT and anti-PD-L1 modestly improved survival when compared with the untreated group. This inconsistency could be attributed to differences in models (eg, orthotopic tumor (irradiated) plus liver metastasis in our model vs two subcutaneous KPC tumors on both flanks45). Together, our data clearly demonstrated that SBRT in combination with blockade of CD73 and PD-L1, two radiation-induced checkpoints, could induce not only local but also systemic/abscopal antitumor immune responses in a PDAC model.
The models (KCKO-Luc and KP2-Luc) were engineered to express luciferase in order to monitor tumor burden longitudinally in vivo. This has both advantages and limitations for the current immunotherapy study. In addition to tracking tumor size, luciferase itself is a moderate immunostimulatory antigen46 that may enhance the immunogenicity properties of ICB and therefore, our model more closely resembles patients with PDAC with higher levels of tumor-infiltrating CD3+ T cells.47 As a result, the current model may not directly mimic the poorly immunogenic PDAC TME where few T cells are present.
In summary, our data demonstrated that triple therapy combining SBRT, anti-CD73 and anti-PD-L1 could be a promising strategy to overcome immunosuppressive barriers in PDAC. Clinical trials combining ICB and anti-CD73 (NCT03611556, NCT04940286, NCT05431270) or CD73 inhibitor (NCT04104672, NCT04148937) are underway or completed in PDAC paving the way for translation of the triple therapy scheme presented here into the clinic. Our results provide proof of principle for the translation of triple therapy combining SBRT, anti-CD73, anti-PD-L1 as neoadjuvant or adjuvant therapy in human PDAC.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design: JY, DL, and SAG. Development of methodology: JY, CJJ, and SAG. Acquisition of data: JY, NWG, DCK, ALH, GH, TGV, and MLL. Analysis and interpretation of data: JY and SAG. Writing, review, and/or revision of the manuscript: JY, EL, GH, JE and SAG. Administrative, technical, or material support: ALH, NWG, DCK, CJJ, BAB and JE. Guarantors: SAG. Study supervision: DL and SAG.
Funding This work was supported by grants from the NIH (R01CA230277 to SAG; R01CA236390 to SAG and ER; R01CA262580 to SAG and DL). We additionally thank Eric Hernady of the Small Animal Radiation Research Core for mice SBRT treatment and Eric Gosselin from AstraZeneca, Waltham, Massachusetts, USA, for adenosine analysis.
Competing interests JE holds AstraZeneca stock.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.