Article Text

Abstract
Background Chimeric antigen receptor (CAR) T-cell therapy is an immunotherapy which uses genetically modified T cells engineered to express CARs to recognize and kill cells that harbor specific antigens. CAR T-cell products designed to target the tumor specific antigens have been used for the treatment of relapse and/or refractory of acute lymphoblastic leukemia, non-Hodgkin lymphomas, myeloma, and solid tumor in clinical trials at our institution. Several side effects have been reported including increased risk of infection.
Methods Retrospective review of morphologic, microbiologic and flow cytometric evaluations done on bronchioalveolar lavages (BAL), pleural effusions, and tissue biopsy specimens from post CAR T-cell adult patients with respiratory complications at our institution from March 2013 to January 2020.
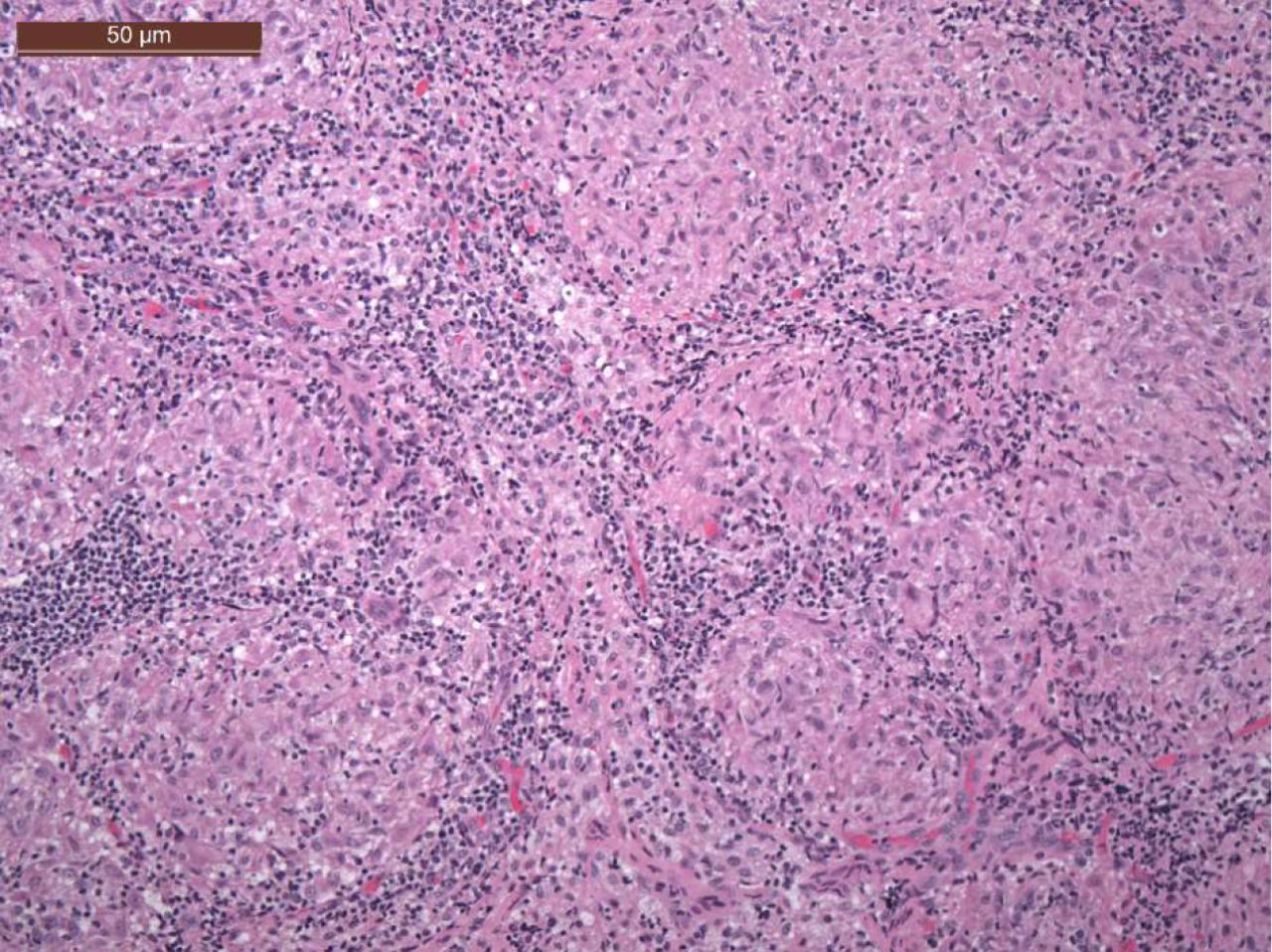
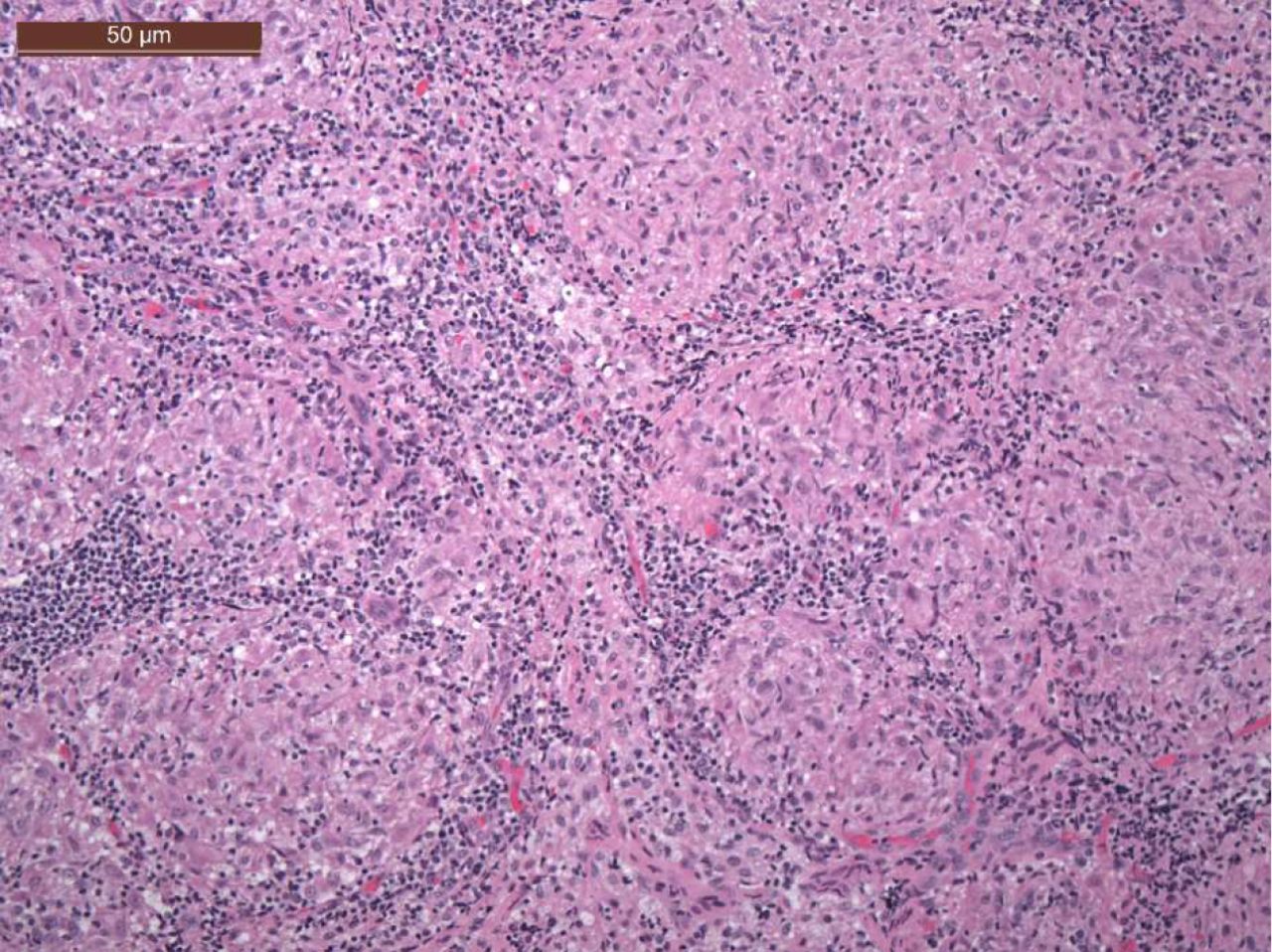
Results Thirteen cases with BAL, 8 cases with biopsy (including lymph node and lung tissue) and 5 cases with pleural effusion are reviewed. All infectious diseases were detected on BAL specimens; while primary disease involvements were mainly seen on biopsy and pleural effusion specimens (figure 1). Interestingly, we found a case of a patient with refractory diffuse large B cell lymphoma that had developed mediastinal lymphadenopathy 9 months after CD19 CAR T-cell infusion (defined composition CD4 and CD8 CAR T-cells). Subsequent biopsies showed granulomatous inflammation with minimal evidence of necrosis (figure 2). Special stains with AFB, Gram, Warthin Starry, and Wright Giemsa showed no evidence of infectious organisms. Special stains were negative for acid fast, fungal, bacterial, or spirochetal organisms. Polymerase chain reaction for Mycobacterium tuberculosis complex DNA by hsp65 amplified probe, and nontuberculous mycobacteria (including Mycobacterium avium complex) by 16s rDNA, hsp65, and rpoB pruner sets were both negative. No abnormal B or T cell population was found by concurrent flow cytometry; however, CAR T-cells were detected at low levels.

Infectious complications were only observed in BAL specimens, while primary disease involvement post-CAR-T cell therapy was mostly observed in pleural effusions and tissue biopsies
{kind=link}
{kind=link}
Hematoxylin and eosin stain of a lymph node biopsy from 329 days post-CAR-T cell infusion (10x magnification) demonstrating extensive noncaseating granulomatous inflammation
Conclusions Granulomatous inflammation is a chronic, histiocytic response to various chemical mediators of cell injury caused by broad etiologies. δγT cells and T helper cells play roles on recruiting circulating monocytes and maturating of macrophages and ultimately the formation of granulomas. In our case, the patient has no documented autoimmune disease. Extensive infectious disease work-ups failed to identified infectious etiology. The presence of CAR T-cells in mediastinal lymph node 9 months after infusion is not unexpected given CAR T-cells can be detected in the blood for years in some patients. The granulomatous inflammation can be part of exaggerated tissue repair process after lymphoma cells killed by CAR T-cells. However, it may complicate or even mislead assessment of therapeutic effect on post-CAR T-cell cases. The finding of enlarged lymph nodes by imaging study certainly raises concern of disease persistent or relapse.
Ethics Approval The study was approved by Fred Hutchinson Cancer Research Center’s Ethics Board, approval numbers 1837, 9364
Consent Written informed consent was obtained from the patient for publication of this abstract and any accompanying images. A copy of the written consent is available for review by the Editor of the this journal.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.