Article Text

Abstract
While immune checkpoint inhibitors (ICI) can lead to sustained responses in metastatic renal cell carcinoma (mRCC), the optimal duration of therapy remains unknown. We aimed to examine treatment-free survival (TFS) in objective responders who discontinued ICI and to explore factors that may impact objective response rate (ORR) and TFS. MEDLINE/PubMed, Embase, and the Cochrane Library were searched for prospective studies reporting individual outcomes after ICI discontinuation in patients with mRCC. Pooled ORR and TFS were estimated using random-effects meta-analyses, and associations between ICI regimen type or treatment line and ORR or TFS were evaluated. Sixteen cohorts comprising 1833 patients treated with ICI were included. The pooled ORR was 43% (95% CI 33% to 53%), and significant differences in summary estimates existed among patients who received ICI monotherapy (22%, 95% CI 18% to 26%), ICI plus a vascular endothelial growth factor (VEGF) pathway inhibitor (57%, 95% CI 48% to 65%), and dual ICI (40%, 95% CI 36% to 44%). Of 572 responders who had available data, 327 stopped ICI, with 86 (26%) continuing to respond off-treatment. Pooled TFS rates at 6 and 12 months were 35% (95% CI 20% to 50%) and 20% (95% CI 8% to 35%), respectively, and were highest for responders treated with dual ICI and lowest for those treated with ICI plus a VEGF pathway inhibitor. Thus, a subset of patients with mRCC who are treated with ICI-based therapy can have durable TFS after therapy discontinuation. Prospective clinical trials and biomarkers are needed to identify patients who can discontinue ICI therapy without compromising clinical outcomes.
- clinical trials as topic
- immunotherapy
- kidney neoplasms
- review
- urologic neoplasms
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Kidney cancer is among the top ten most common cancers in both Europe and the USA, accounting for approximately 3.5% and 4.0% of all new cancer diagnoses, respectively.1 2 The incidence rate of renal cell carcinoma (RCC), the most prevalent form of kidney cancer, has significantly increased over the past several years.3 Current treatment strategies for metastatic RCC (mRCC) include cytoreductive nephrectomy and systemic therapies such as antiangiogenic vascular endothelial growth factor (VEGF) tyrosine kinase inhibitors, mTOR inhibitors and most recently, immune checkpoint inhibitors (ICI).4–6 ICI are monoclonal antibodies that target immune regulatory pathway proteins (eg, CTLA-4, PD-1, PD-L1) used by cancer cells to escape immunosurveillance, and their overall therapeutic effect is to unleash an effective T cell antitumor response.7 Either alone or in combination with other therapies, ICI have played an increasingly important role as first-line and subsequent-line agents for advanced RCC, especially in intermediate-risk and poor-risk patients.5 8–10
However, as a relatively novel advancement in mRCC treatment, ICI therapy still requires empirical optimization to minimize immune-related toxicity as well as determine ideal treatment duration and combinations with other therapies.5 11–13 Despite their efficacy, ICI can cause rare but serious immune-related adverse effects and are considerably more expensive than many other anticancer drug classes.14 15 Interestingly and in contrast to other systemic agents, ICI can potentially induce complete remission even after treatment cessation, a phenomenon best studied in metastatic melanoma and non-small cell lung cancer.12 16 17 Preliminary evidence indicates that a subset of patients with mRCC experience durable responses following ICI discontinuation and that intermittent ICI may be a feasible treatment approach.13 18 Although these data suggest that extended duration of therapy may not be necessary for sustained clinical benefit, there are currently no specified criteria for ICI cessation in the absence of progressive disease or unacceptable toxicities. Pinpointing specific parameters to guide ICI treatment duration in mRCC could therefore help maximize beneficial outcomes while reducing adverse effects and financial burden.13 The objective of this analysis is to assess rates of treatment-free survival (TFS) after ICI cessation in patients with mRCC who demonstrated partial or complete responses to ICI and to evaluate factors that may influence objective response rate (ORR) and TFS.
Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.19
Search strategy and study selection
MEDLINE/PubMed, Embase, and the Cochrane Library were queried from database inception to January 27, 2021 using the following algorithm: (immunotherapy OR “immune checkpoint” OR nivolumab OR ipilimumab OR pembrolizumab OR avelumab OR atezolizumab OR durvalumab) AND (“renal cell carcinoma” OR RCC OR “kidney cancer”) AND (metastatic OR advanced) AND (stop OR stopped OR discontinuation OR discontinue OR withdrawal OR withdrawn OR treatment free). In addition, reference lists of relevant review and study articles were manually searched for other studies. Two authors (AT, THT) independently screened titles, abstracts, and full-text publications for study eligibility, with any disagreements resolved by discussion.
Prospective studies fulfilling the following criteria were included: (1) involved patients ≥18 years old with advanced or mRCC who were treated with checkpoint blockade antibodies either as monotherapy or in combination with other therapies; (2) reported patient-level TFS after immunotherapy discontinuation for at least a subset of objective responders; and (3) written in English or included an English translation. TFS was defined as the period from therapy cessation until subsequent systemic therapy initiation, death, or censoring, whichever occurred first.20 Studies were excluded if they were case reports, cell culture or animal studies, reviews, systematic reviews or meta-analyses, comments/editorials, or conference abstracts. When the same population was described in separate publications, only the most recent article that met the inclusion criteria and had the largest sample size was included.
Data collection and quality assessment
Using a standardized form, two authors (AT, THT) independently extracted the following data from each included study: lead author; publication year and journal; clinical trial identifier and phase; immunotherapy regimen (specific immune checkpoint inhibitor and any other drug used in combination) and discontinuation criteria (online supplemental table S1); treatment arm sample size; patient characteristics (age, sex, performance status, prognostic risk group, nephrectomy, and systemic treatment history); follow-up and immunotherapy treatment duration; and ORR. TFS data for individual patients were extracted from published swimmer plots using WebPlotDigitizer V.4.4.21
Supplemental material
The same two authors independently evaluated the risk of bias in individual studies using a modified Newcastle-Ottawa Scale.22 Since intra-study comparability was not relevant to this systematic review and meta-analysis, each arm of an included study was assessed as an independent cohort as previously described,23 using the following six criteria: (1) cohort representative of patients with advanced/mRCC; (2) immunotherapy treatments documented in medical records; (3) outcome of interest demonstrated to be absent at start of study; (4) outcomes assessed using objective, predefined criteria; (5) adequate follow-up duration for outcomes to occur (≥12 months); and (6) adequate cohort follow-up (<10% lost to follow-up or description provided of patients lost to follow-up). Based on quality assessment standards employed in prior meta-analyses, studies meeting at least four of the above criteria were considered to be of higher quality.23 24 Discrepancies were resolved by consensus among all authors.
Data synthesis and analysis
Statistical analyses were performed using the meta25 and metafor26 packages in R V.4.0.3, and two-sided p<0.05 was considered statistically significant. For each study cohort, the proportion of patients with objective responses or with TFS at 6 and 12 months, along with the associated 95% CI, were calculated. The variance-stabilizing Freeman-Tukey double-arcsine transformation27 was then applied to the observed proportions. To estimate summary effect sizes, individual effect sizes and sampling variances were pooled based on the inverse-variance method using a random-effects model (restricted maximum-likelihood approach) to assign weights. Study cohorts were stratified by ICI regimen type and by treatment line to investigate potential factors correlated with ORR and TFS, and a Wald-type test was conducted to determine whether differences between subgroups were significant.26
Heterogeneity between study cohorts was assessed using Cochran’s Q test and the I2 statistic, with I2 values greater than 75% suggesting a high degree of heterogeneity.28 Outlying effect sizes were detected by identifying externally studentized residuals with absolute values greater than 2,29 and their influence on the summary proportions was evaluated using leave-one-out sensitivity analyses.26 Visual inspection of funnel plots, the rank correlation test, and Egger’s regression test were used to examine publication bias.30–32
Results
Search results
Our systematic database search yielded 1685 records, of which 780 remained after duplicates were removed. An additional seven records were identified through manual review of reference lists. After screening titles and abstracts, a further 708 records were excluded due to language, publication type, retrospective study design, or topic. Of the 79 full-text articles assessed for eligibility, 67 were excluded because they included duplicate cohorts from other studies or did not provide the data needed for this meta-analysis. Thus, 12 prospective studies published between 2017 and 2020 were included in the final quantitative synthesis (figure 1). Four of these studies comprised independent cohorts (separate treatment arms) that are presented individually in our meta-analysis,33–36 so a total of 16 cohorts are analyzed in this review (table 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram for study identification and selection.
Characteristics of included studies
Study and patient characteristics
Standardized characteristics of the included patient cohorts are summarized in tables 1 and 2. Overall, 1833 patients with mRCC treated with ICI were available for analysis. Among the selected cohorts, five included patients who received monotherapy,18 36–38 six included patients who received ICI plus a VEGF pathway inhibitor (VEGFi),33 34 39 40 and five included patients who received dual ICI.35 41–43 The median age ranged from 54 to 69 years, and a majority of patients (75%) were men. Based on available data for functional status, 98% of patients had Eastern Cooperative Oncology Group 0‒1 or Karnofsky Performance Score ≥80. Surgical history was reported for 93% of patients, and 86% had prior nephrectomy. ICI were used as first-line therapy in five cohorts,34 36 39 40 42 as refractory setting therapy in six cohorts,18 33 34 36–38 and as first-line or subsequent-line therapy in five cohorts.33 35 41 43 According to the modified Newcastle-Ottawa Scale, all studies were of high methodological quality (table 1).
Baseline patient characteristics
ICI treatment and ORR
The weighted mean ORR for patients with mRCC who received ICI was 43% (95% CI 33% to 53%) (figure 2), and significant heterogeneity was present between cohorts (I2=91%, p<0.01). No outlying cohorts were detected; concordantly, sensitivity analysis performed by removing one cohort at a time indicated that the estimated summary proportion was not significantly influenced by any single cohort (online supplemental figure S1A).
Supplemental material
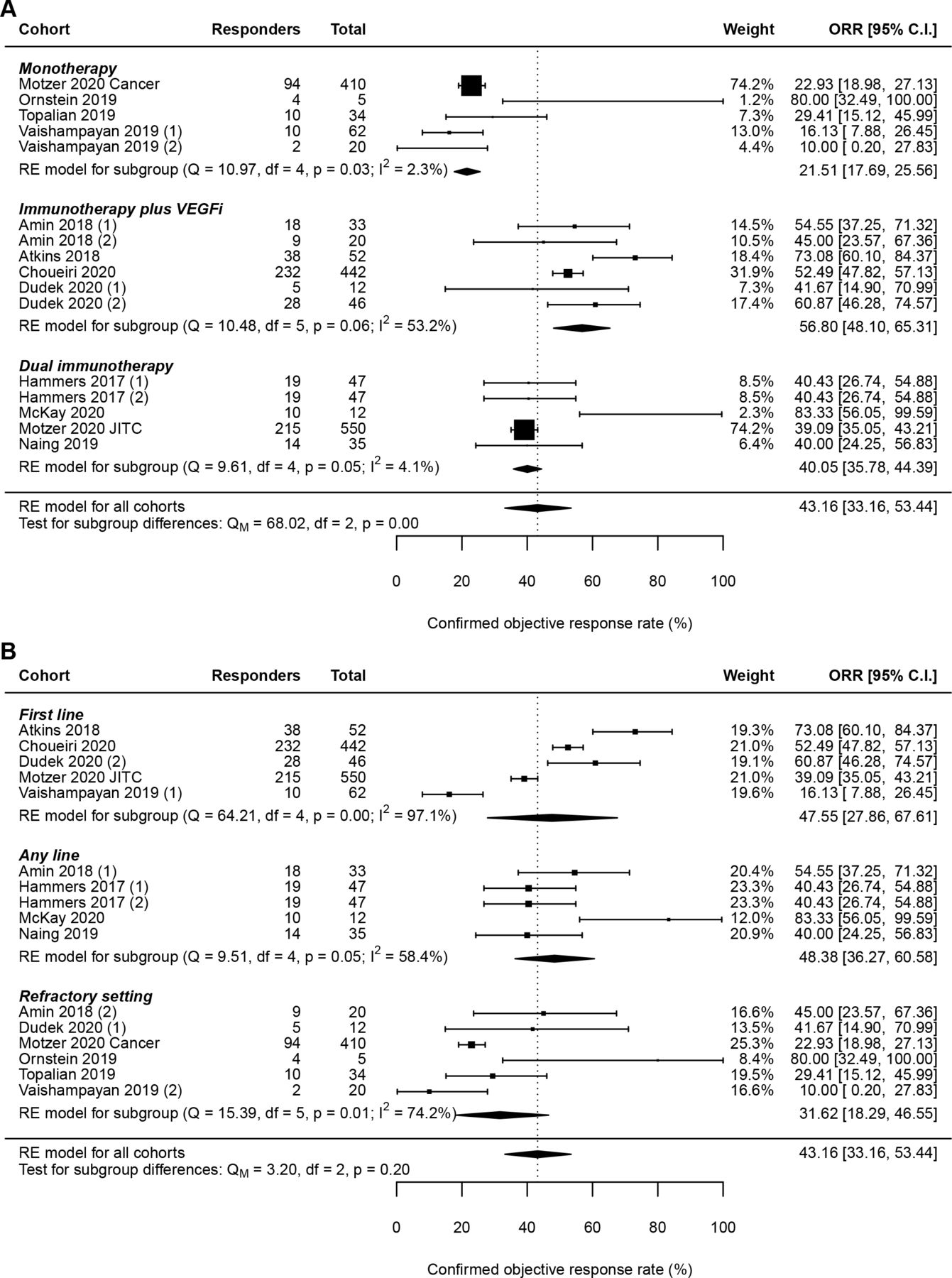
Random-effects (RE) meta-analysis of objective response rate (ORR) in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors (ICI) stratified by (A) ICI regimen type and (B) treatment line. Total: number of response-evaluable patients. VEGFi, vascular endothelial growth factor pathway inhibitor.
When stratifying by ICI regimen type, the pooled ORR differed significantly across subgroups (p<0.001) (figure 2A). Specifically, the weighted mean ORR was highest for patients treated with ICI plus VEGFi (57%, 95% CI 48% to 65%) and lowest for patients treated with ICI monotherapy (22%, 95% CI 18% to 26%). For patients treated with dual ICI, the pooled ORR was 40% (95% CI 36% to 44%). The extent of heterogeneity within subgroups was also lower (I2<55% in all subgroups) than that within the overall pool, indicating that differences in the type of ICI regimen could partially account for the variability in observed ORR across all cohorts.
By contrast, stratifying by ICI treatment line did not result in significantly different pooled ORR across subgroups (p=0.20), and within-subgroup heterogeneity remained moderate to high (figure 2B). These findings suggest a lack of relationship between treatment line and ORR in patients with mRCC receiving ICI.
ICI treatment and TFS rate
To better characterize outcomes in objective responders after ICI discontinuation, data from a total of 572 complete or partial responders were further analyzed (table 3). Of these patients, 327 had documented cessation of ICI therapy, with median TFS ranging from 0.0 to 23.5 months. Strikingly, 26% of the 327 responders who discontinued ICI demonstrated ongoing response off-treatment.
Treatment-free survival after discontinuation of immune checkpoint inhibitors in patients with objective response
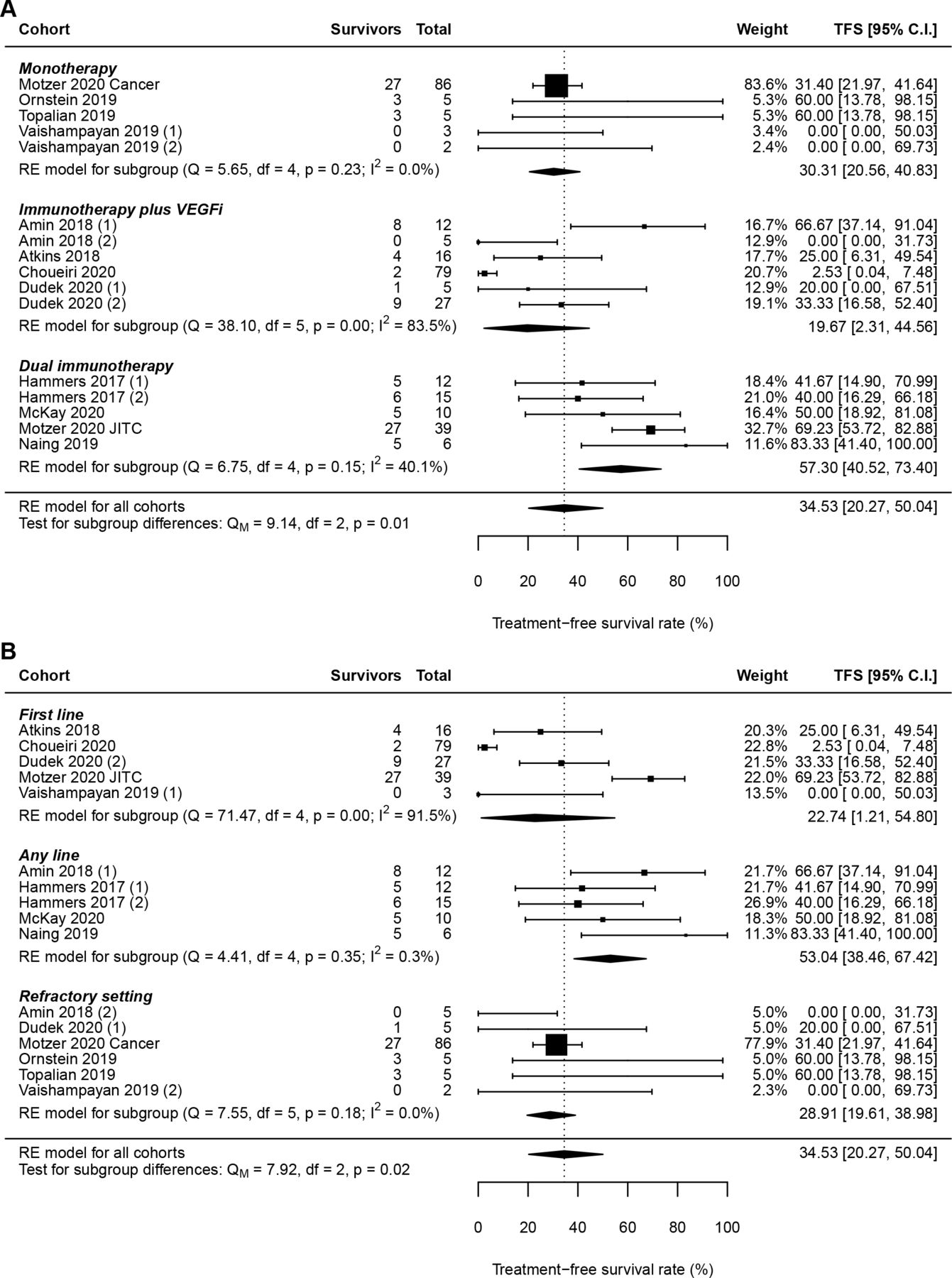
At 6 and 12 months, the weighted mean TFS rates for responders who stopped ICI were 35% (95% CI 20% to 50%) (figure 3) and 20% (95% CI 8% to 35%) (figure 4), respectively, with considerable heterogeneity present between cohorts (I2=85%, p<0.01 for 6-month and 12-month TFS rates). Of note, two cohorts did not have sufficient follow-up to calculate 12-month TFS rates and were therefore excluded from that analysis.18 41 One cohort was identified as an outlier with respect to both 6-month and 12-month TFS rates,40 although the estimated summary proportion did not change significantly when this cohort was removed (online supplemental figure S1B; online supplemental figure S1C). Analysis of 12-month TFS rates detected an additional outlier42 whose removal likewise did not significantly affect the estimated summary proportion (online supplemental figure S1C).

Random-effects (RE) meta-analysis of 6-month treatment-free survival (TFS) rate in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors (ICI) stratified by (A) ICI regimen type and (B) treatment line. Total: number of responders who discontinued ICI. VEGFi, vascular endothelial growth factor pathway inhibitor.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
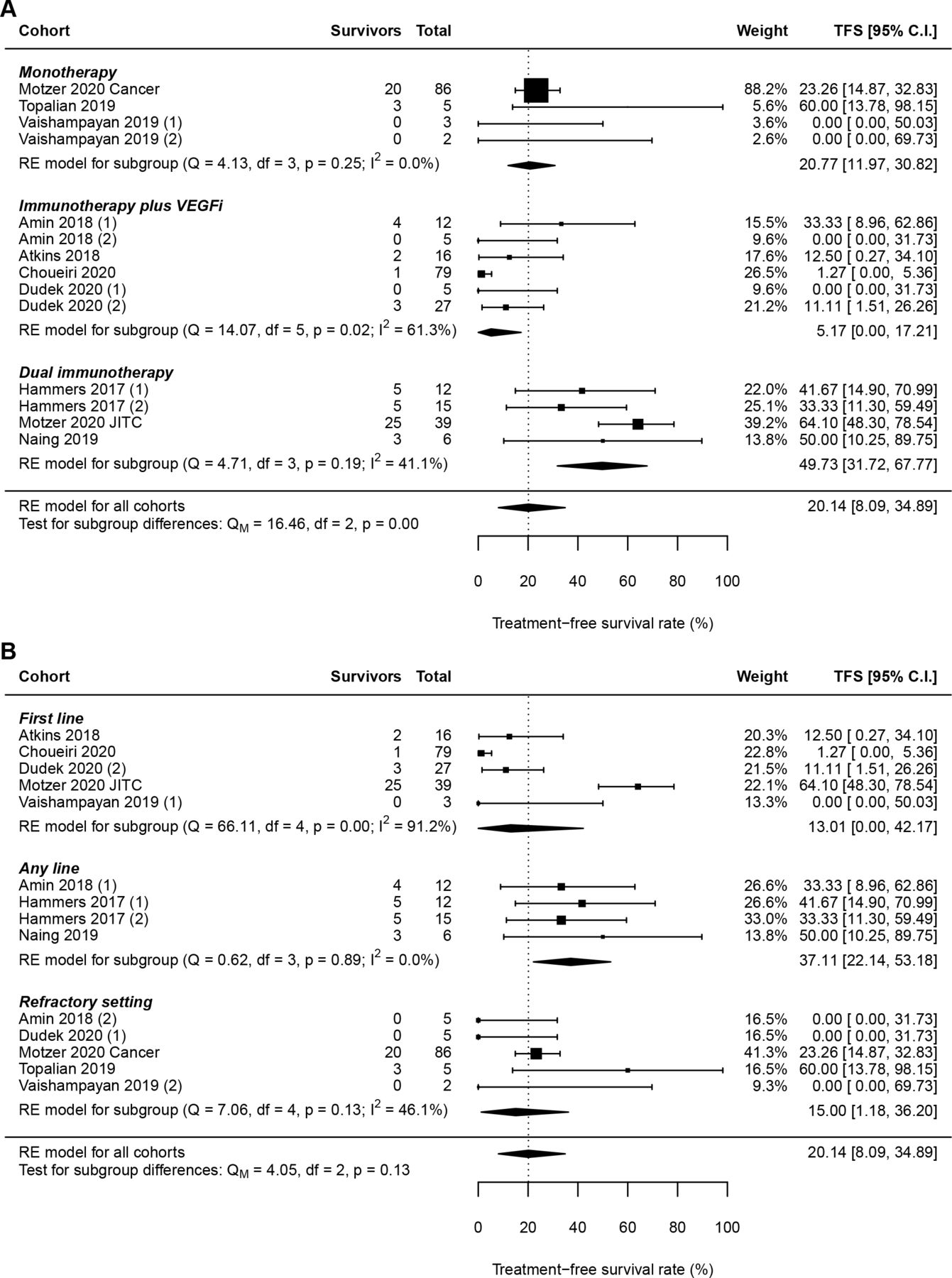
Random-effects (RE) meta-analysis of 12-month treatment-free survival (TFS) rate in patients with metastatic renal cell carcinoma treated with immune checkpoint inhibitors (ICI) stratified by (A) ICI regimen type and (B) treatment line. Total: number of responders who discontinued ICI. VEGFi, vascular endothelial growth factor pathway inhibitor.
Stratifying by ICI regimen type resulted in significantly different TFS rates across subgroups at both 6 (p=0.01) and 12 months (p<0.001) (figure 3A; figure 4A). In particular, patients treated with dual ICI had the highest weighted mean TFS rates at 6 (57%, 95% CI 41% to 73%) and 12 (50%, 95% CI 32% to 68%) months, and patients treated with ICI plus VEGFi had the lowest weighted mean TFS rates at 6 (20%, 95% CI 2% to 45%) and 12 months (5%, 95% CI 0% to 17%). Meanwhile, the pooled TFS rates for patients treated with ICI monotherapy were 30% (95% CI 21% to 41%) at 6 months and 21% (95% CI 12% to 31%) at 12 months. Whereas TFS rates did not exhibit significant within-subgroup variability for patients who received ICI monotherapy or dual immunotherapy, TFS rates for patients who received ICI plus VEGFi showed moderate-to-high heterogeneity (figure 3A; figure 4A).
Although subgroup analysis revealed significant differences in pooled TFS rates based on ICI treatment line at 6 months (p=0.02) (figure 3B), pooled TFS rates were comparable in the first-line, any-line, and refractory settings at 12 months (p=0.13) (figure 4B). Pooled TFS rates at both time points were highest for cohorts that included patients who received ICI in any treatment line (53%, 95% CI 38% to 67% at 6 months; 37%, 95% CI 22% to 53% at 12 months). At 6 months, pooled TFS rates for patients receiving first-line and refractory setting ICI were 23% (95% CI 1% to 55%) and 29% (95% CI 20% to 39%), respectively, which decreased to 13% (95% CI 0% to 42%) and 15% (95% CI 1% to 36%) at 12 months. However, in contrast to the other subgroups, significant heterogeneity was present in the first-line ICI subgroup (I2=92% at 6 months and 91% at 12 months) (figure 3B; figure 4B), suggesting that additional potential sources of systematic variation exist between cohorts in that subgroup. Collectively, these results indicate that ICI regimen type has a more consistent effect than treatment line on TFS in objective responders with mRCC.
Publication bias
Funnel plots were constructed to estimate the extent of publication bias in our pooled analyses (online supplemental figure 2). For ORR, neither the rank correlation test (p=0.50) nor Egger’s regression test (p=0.20) for funnel plot asymmetry showed strong evidence of publication bias. Similarly, for TFS rates at 6 and 12 months, the rank correlation test (p=0.89 for 6-month TFS rate; p=0.96 for 12-month TFS rate) and Egger’s regression test (p=0.90 for 6-month TFS rate; p=0.80 for 12-month TFS rate) did not reveal the presence of publication bias.
Discussion
In this systematic review and meta-analysis of mRCC clinical trials, TFS after ICI discontinuation in patients who demonstrated a partial or complete response was quantified. Three key findings emerge from these data. First, a relatively high percentage (26%) of patients who discontinue therapy after obtaining a response to ICI therapy exhibit sustained responses off therapy. Second, the TFS can be fairly durable with 6-month and 12-month mean TFS rates of 35% and 20%, respectively (figure 3; figure 4). Finally, 6-month and 12-month mean TFS rates were higher for patients treated with dual ICI therapy (57% and 50%, respectively) than for those treated with ICI and VEGF-directed therapy (20% and 5%, respectively).
Over the last few years, the treatment paradigm of mRCC has been revolutionized with the introduction of ICI-based therapy. One of the key features of such regiments is the potential for durable responses beyond that which was seen with VEGF-directed monotherapy. However, a critical unanswered question with ICI treatment is the duration of therapy necessary to achieve and sustain a response. This question has resulted in new investigations into the consideration of TFS in interpreting ICI-based clinical trials and even using TFS as a trial endpoint.20
The findings presented herein lend support to consideration of discontinuing ICI therapy even in the absence of disease progression or excessive toxicity. Indeed, this idea is already incorporated into certain clinical trials such as the KEYNOTE-426 trial (axitinib/pembrolizumab vs sunitinib in mRCC), in which patients discontinued pembrolizumab after 35 3-week cycles (approximately 2 years).44 Importantly, a subsequent analysis of patients in this trial who completed 2 years of therapy demonstrated that a high proportion had ongoing clinical benefit.45 Although these patients remained on axitinib, the data do highlight the feasibility of earlier discontinuation of ICI therapy.
An interesting result in the present analysis is the apparent inverse relationship between ORR and TFS in patients treated with ICI-based combinations. The pooled ORR was higher in ICI plus VEGFi versus ICI plus ICI (57% vs 40%). However, the pooled 6-month and 12-month TFS rates were lower for patients treated with ICI plus VEGFi (20% and 5%) than for those treated with dual ICI (57% and 50%). In addition to supporting the notion of prolonged responses off therapy, these data reflect clinical trial data that indicate a higher ORR in patients treated with ICI/VEGFi combinations compared with dual ICI.44 46 47 However, the rationale for using dual ICI therapy despite a lower initial response rate is the potential for the durable responses seen with ICI/ICI and not yet fully appreciated in ICI/VEGFi combinations.48 49
This analysis has a number of limitations. Prospective ICI-based clinical trials in mRCC that did not include TFS data were unable to be included in the present analysis.44 50–52 In addition, there was significant heterogeneity in clinical trial design among the included trials, requiring caution when interpreting these results. We suspect the increased heterogeneity in the TFS rates of patients treated with ICI/VEGFi compared with those treated with single-agent or dual ICI is related to the heterogeneity of specific therapies in each ICI regimen type. In particular, both the ICI/ICI and monotherapy subgroups encompassed only two different treatment regimens. Meanwhile, the ICI/VEGFi subgroup included five different regimens that nonetheless had similar mechanisms of action. Since patient-level TFS was digitally extracted from published swimmer plots, data extraction accuracy was limited by figure resolution. Importantly, the data presented in our analysis primarily originated from patients who achieved a response to ICI-based therapy. Data for patients who discontinued therapy with a best response of stable disease remain largely unavailable. Likewise, the reason for treatment discontinuation at an individual level was not available for all trials and perhaps clinical outcomes are different in patients who discontinue therapy due to adverse events compared with those who discontinue for other reasons.53
Despite these limitations, the data herein have key implications for clinical care and research as they demonstrate that treatment response to ICI can continue beyond treatment discontinuation. Financial and physical toxicity are critical considerations for patients undergoing chronic anticancer therapy. The use of ICI-based therapy until disease progression or intolerable toxicity likely causes unnecessary harm to a subset of patients who do not require indefinite therapy.
Fortunately, trials are underway in mRCC and other malignancies to investigate the duration of ICI therapy required for optimal long-term clinical benefit.54–56 A primary challenge in these trials is the need to identify predictive factors for patients who can discontinue treatment prior to disease progression or toxicity. Further exploration of treatment response parameters, blood-based biomarkers, and novel imaging techniques are all urgently required to properly select patients for ICI discontinuation.
Conclusion
A subset of patients with mRCC who are treated with ICI-based therapy can have durable TFS after therapy discontinuation. Prospective clinical trials and biomarkers are needed to identify patients who can discontinue ICI therapy without compromising clinical outcomes.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AT and MCO designed the project. AT and THT performed the database search, study selection, data extraction and quality assessment. AT analysed the data. All authors contributed to manuscript writing and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AT and THT have no relevant financial or non-financial interests to disclose. MCO receives research funding from Bristol-Myers Squibb (BMS) and Pfizer; consulting/advisory fees from BMS, Pfizer, Merck, Exelixis, Eisai, and Aveo.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.