Article Text

Abstract
Background In melanoma patients who progress after prior ipilimumab/nivolumab (ipi/nivo) combination immunotherapy, there is no information regarding the risks and benefits of reinduction ipi/nivo.
Methods This was a retrospective review of 26 melanoma patients treated at Memorial Sloan Kettering Cancer Center (MSKCC) since 2012 who received reinduction ipi/nivo at least 6 months following completion of an initial course of ipi/nivo. We collected data on demographics, genetics, immune-related adverse events (irAEs), best overall responses (BORs), time to treatment failure (TTF) and overall survival (OS).
Results The BOR rate (complete response+partial response) was 74% (95% CI 52% to 90%) after the first course of ipi/nivo but only 23% (95% CI 8% to 45%)) after reinduction. Response to reinduction did not correlate with response to the initial course. Among the 16 patients who had an objective response to the first course, only four (25%) responded to reinduction. Of five patients who did not respond to the first course, one responded to reinduction. For all patients, median TTF was 5.3 months after reinduction; TTF was shorter for reinduction than for the first course in 85% of patients. Median OS from reinduction was 8.4 months; estimated 2-year OS was 18%. Although reinduction was associated with fewer irAEs than the initial course of ipi/nivo (58% of patients vs 85% of patients in the initial course), eight (31%) patients experienced at least one new irAE after the second course.
Conclusions BOR rate and TTF were markedly less favorable after reinduction with ipi/nivo than after the initial course of ipi/nivo. Reinduction ipi/nivo was associated with frequent irAEs although less frequent than for the initial course.
- immunotherapy
- melanoma
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. We will make available a deidentified version of an Excel datasheet containing the extracted data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Starting with the first phase 1 trial of ipilimumab/nivolumab (ipi/nivo) combination,1 multiple trials have confirmed the high level of antimelanoma activity.2–4 This combination has also become a treatment of choice for melanoma patients with brain metastases.5 6 Because of the mechanism of action and high response rate, ipi/nivo has been tested in patients with other malignancies and has shown impressive activity in lung cancer,7 renal cell carcinoma,8 and others.9 Ipi/nivo is associated with a high incidence of immune-related adverse events (irAEs), most of which are serious and require treatment. Some irAEs do not resolve. This has led to ongoing discussions as to the risks and benefits of ipi/nivo in various melanoma patient cohorts.
We have a long experience in our institution of using ipi/nivo in melanoma, and during this time, we have had the opportunity to re-treat melanoma patients who progressed following an initial course of ipi/nivo with a second (or reinduction) course of ipi/nivo; this was generally not allowed on the previous clinical trials. Reinduction with ipi monotherapy has been shown to be effective in a minority of patients after an initial course of ipi10–12; similarly, reinduction with anti-PD1 therapy can benefit a minority of patients after an initial course of anti-PD1 therapy.13 Little is known about the efficacy of reinduction ipi/nivo even though reinduction ipi/nivo is listed in the NCCN guidelines14 as a treatment option. We describe this cohort of melanoma patients who were treated with reinduction ipi/nivo at least 6 months after the end of the first induction course of ipi/nivo. In reporting the outcomes, we hope to provide guidance on the risks and benefits of reinduction ipi/nivo.
Methods
Patients and treatment
We studied outcomes in patients who had received at least two separate courses of ipi/nivo. To be a separate course, there had to be at least a 6-month interval between doses. We performed an electronic search of the electronic medical record at MSKCC for melanoma patients treated with ipi/nivo between January 2012 and December 2020. Specifically, we searched for patients who had received more than four doses of ipi/nivo or who had received two doses separated by at least 6 months. Patients who received maintenance anti-PD1 therapy after the initial course of ipi/nivo were included if there had been at least 6 months between the completion of maintenance anti-PD1 and the start of reinduction ipi/nivo. Cases were confirmed by detailed chart review. Basic demographics were collected including treatment dates, date of last follow-up and date of death. In patients in whom the melanoma had undergone next-generation sequencing of actionable cancer targets,15 we collected information on driver mutations, tumor mutational burden, and class I HLA identification.
irAEs and time-to-treatment failure (TTF), defined as the time from start of ipi/nivo to the start of a subsequent treatment (either systemic therapy, radiation therapy, or surgery but not including maintenance anti-PD1 therapy) or death, were collected by chart review. No attempt was made to grade the irAEs, but we did note if the patient required corticosteroids, infliximab, or mycophenolate immunosuppression for irAEs.
A retrospective radiographic review was performed in order to assess best overall response (BOR) according to RECIST V.1.1.
Statistical analysis
Patient and tumor characteristics were summarized using summary statistics. Overall survival was defined as the time from date of first (or second) course of ipi/nivo to date of death or date last known alive. TTF was defined as the time from the start of the first (or second) course of ipi/nivo to the date of the next treatment, death, or date last known alive. TTF from first cycle (y-axis) and reinduction (x-axis) were plotted on a correlation plot to visualize any associations between time to treatment failure after each treatment. McNemar’s test was used for paired data to compare best objective response rate (complete response (CR)/partial response (PR) vs other) assessed after first course ipi/nivo and reinduction.
Results
Our search initially identified 53 potential patients. After chart review, we eliminated 27 patients either because they did not have melanoma, had not received ipi/nivo, or had received multiple courses with no interruption of at least 6 months. The remaining 26 patients form the basis of this report.
Patient demographics
The 26 patients in this cohort (table 1) were typical of patients with metastatic melanoma. There were 17 men and 9 women with a median age of 57.6 years at the time of initial ipi/nivo treatment. The primary site was cutaneous in 65% of cases and was unknown in 4/26 patients (15%). The remaining five patients (27%) had acral or subungal primary sites. There were no patients with mucosal or choroidal primaries. At the time of initial ipi/nivo treatment, four patients had unresectable stage III melanoma; the remaining patients had stage IV melanoma including seven patients with central nervous system metastases (stage IVD).
Patient demographics (n=26)
The driver mutation was BRAF in 10 patients, NRAS in 5 patients, and 2 patients had other driver mutations (KRAS and NF1 inactivation, respectively). In six cases, we could not identify a driver mutation, and in three cases, genetic analysis was not performed. Half of the cases analyzed qualified as having a high mutational burden (defined as ≥10 mutations/Mb). The patient’s class I HLA-A, B, and C alleles were identified as well from this analysis.
Treatment courses
Ipi/nivo was administered every 3 weeks using ipilimumab at dose of 3 mg/kg and nivolumab at 1 mg/kg. In 3/150 treatments (all during the reinduction course of ipi/nivo), ipilimumab was used at 1 mg/kg and nivolumab at either 3 mg/kg or 240 mg flat dose.
During the first course of ipi/nivo, the median number of doses was 4 (range 1–4); 16 patients (61.5%) received maintenance nivolumab after the first course. The median time to reinduction with ipi/nivo was 22.2 months (range 6–49.1). Nine patients (35%) had received a total of 10 treatment regimens after induction ipi/nivo but prior to reinduction (four received BRAF/MEK inhibition; three received chemotherapy, two received ipi; one was treated on a phase I trial). For reinduction, the median number of ipi/nivo doses was 3 (range 1–4); seven patients received all four doses of reinduction ipi/nivo.
Efficacy
The BOR after the first course of ipi/nivo was a CR in 1 patient, PR in 16 patients, and stable disease in 6 patients; three patients did not have tumor measurable by RECIST. This corresponds to a 74% (95% CI 52% to 90%) response rate. After reinduction with ipi/nivo, we observed two CRs, three PRs, nine stable disease, and eight progression of disease as BOR; four patients did not have measurable disease. This corresponded to only a 23% (95% CI 8% to 45%) response rate. We analyzed the concordance of response between the initial and the reinduction course of therapy at the individual patient level (table 2). Of the 21 patients who had measurable tumor prior to both courses of ipi/nivo, only three (14%) had a better objective response after reinduction compared with the first course, while 14 (67%) had a worse objective response to reinduction. Of the 16 evaluable patients who had a CR or PR to the first course of ipi/nivo, only four (25%) responded to reinduction with ipi/nivo. Of the five patients who had stable disease as BOR to the first course of ipi/nivo, only one responded to reinduction (PR that lasted 4.1 months). Initial response to the first course of ipi/nivo was not associated with response to re-induction (McNemar’s test; p value=0.002).
Concordance of BOR between courses of ipi/nivo
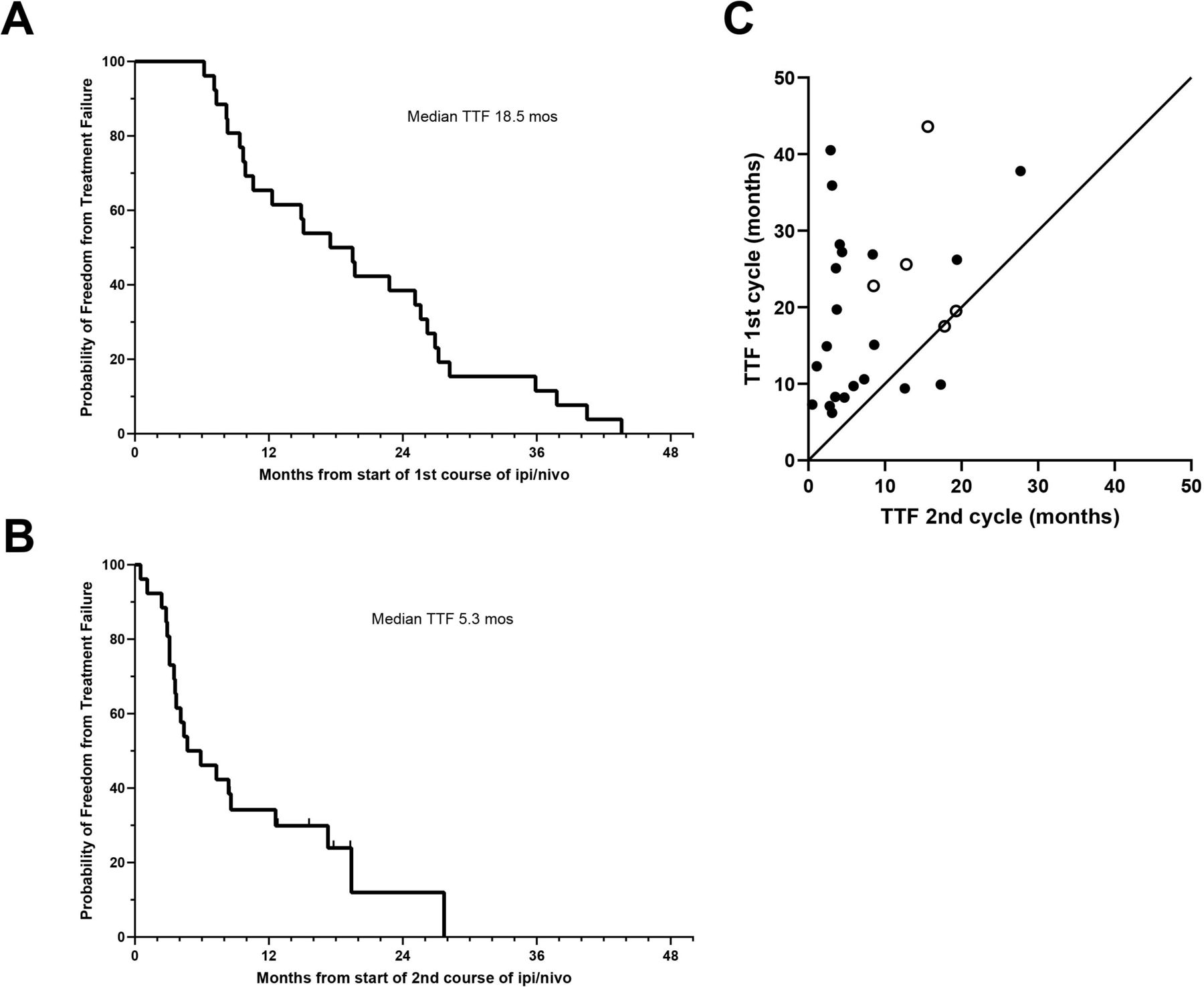
By definition, all patients in this cohort progressed after the first course of ipi/nivo; the median TTF was 18.5 months (95% CI 9.9 to 25.6) (figure 1A). However, after reinduction with ipi/nivo, the median TTF was only 5.3 (95% CI 3.5 to 12.6) months (figure 1B). The estimated treatment failure rate after reinduction was 100% by 28 months. In comparing the TTF after the first course with the TTF of the reinduction course of ipi/nivo for each patient (figure 1B, the TTF after reinduction was shorter by a median of 8 months. At an individual patient level, 22/26 patients (85%) experienced shorter TTF after reinduction compared with the first course (median: 12 months, range: 3–38 months). In two patients, TTF was the same after initial ipi/nivo and reinduction. In two patients, TTF after reinduction was slightly longer (3.2 months and 5.4 months) than for the first course.
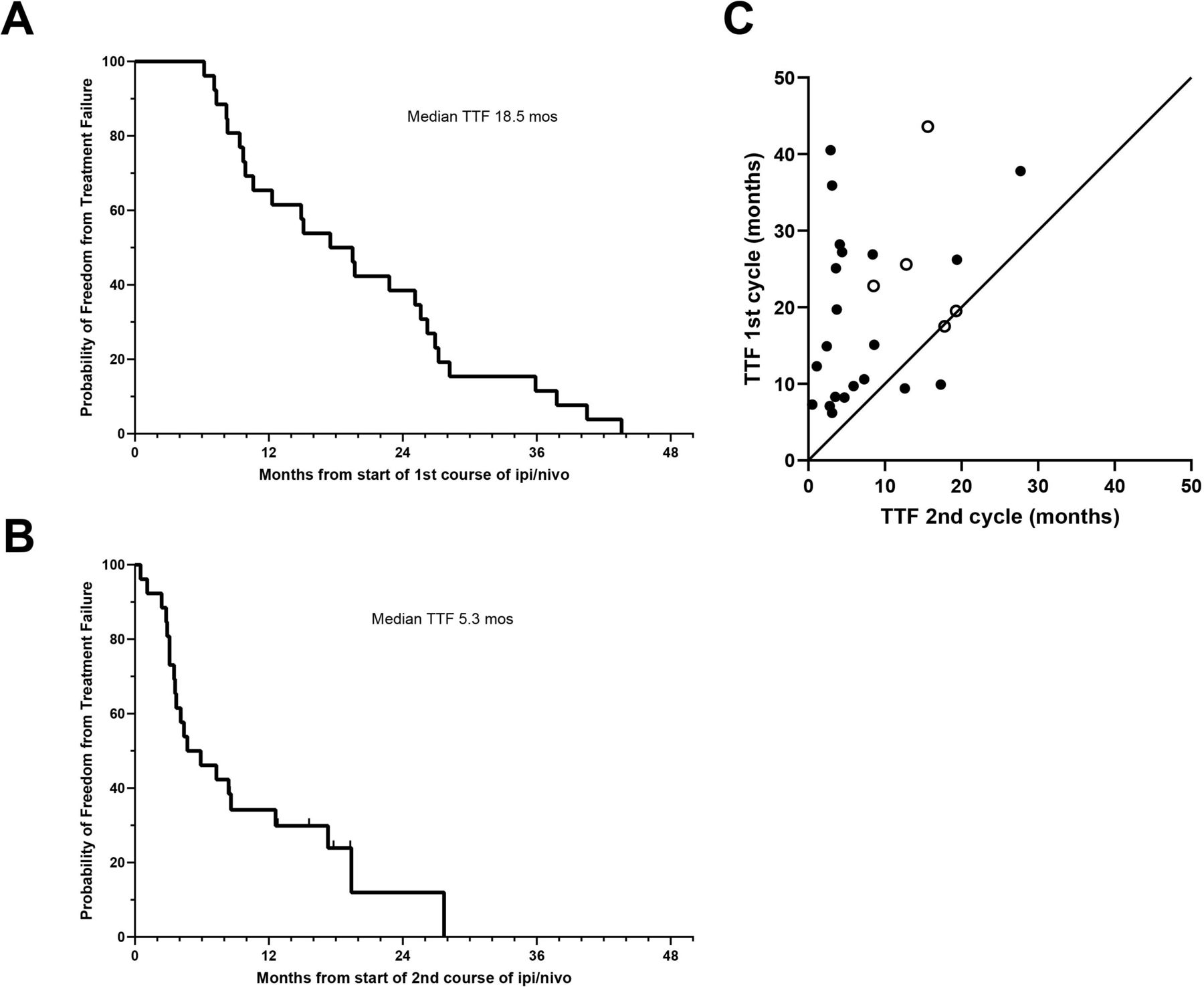
Time-to-treatment failure (TTF) for all patients from the start of the initial course if ipi/nivo (A) and from the start of reinduction ipi/nivo (B). Tick marks indicate censored patients. Figure part C compares the TTF seen after the initial course if ipi/nivo with the TTF seen after reinduction for each individual patient. Open circles indicate patients censored for TTF after reinduction with ipi/nivo. The equivalence line is indicated. ipi/nivo, ipilimumab/nivolumab.
The median overall survival from the start of the first course of ipi/nivo was 35.3 months (figure 2). The estimated survival at 4 years was 28%. However, from the start of reinduction with ipi/nivo, the median survival was only 8.4 months; the estimated 2-year survival was only 19%. This is consistent with the low ORR and TTF observed after reinduction with ipi/nivo.

{kind=link}
{kind=link}
Overall survival (OS) from the start of the first course of ipi/nivo (A) and from the start of reinduction ipi/nivo (B). Tick marks indicate censored patients. ipi/nivo, ipilimumab/nivolumab.
We did not observe any correlation between treatment efficacy and driver mutation, tumor mutation burden, or class I HLA type.
Immune-related adverse events
The irAEs observed are indicated in table 3. Twenty-two of 26 patients (85%) had at least one irAE as a result of the first course of ipi/nivo; 13 (50% of all patients) required treatment with infliximab and/or corticosteroids. The most common irAEs were hepatitis, rash, and colitis. After reinduction ipi/nivo, only 58% of patients experienced an irAE with the second course, but 11 patients required immunosuppression with corticosteroids, infliximab, or mycophenolate (42% of all patients). The most common irAEs as a result of the second course of treatment were again hepatitis, rash, and colitis. Only two patients received both courses of ipi/nivo without experiencing an irAE. The irAEs that most commonly occurred in both the initial and the reinduction course of ipi/nivo were: hepatitis, colitis, rash, and fever. Eight patients (31%) experienced one or more serious irAEs after the reinduction course of therapy that they had not experienced after the first course including: type I diabetes, pneumonitis, hypopituitarism, meningitis, colitis, and hepatitis. We did not observe any correlation between incidence of irAE and class I HLA type.
Immune-related adverse events
Discussion
In treatment-naïve patients, combination ipi/nivo is associated with 58% response rate with 22% CRs.16 This translated into 5-year progression-free survival of 48% in BRAF-mutated patients and 38% in BRAF wild-type patients. Five-year overall survival was 60% and 48%, respectively. Based on these data and other supportive data,2 4–6 ipi/nivo has become a standard of care for the treatment of metastatic melanoma.
There are a variety of known and conjectured mechanisms of resistance to checkpoint inhibitor therapy, both native and acquired.17–21 The patient’s T cell repertoire may not contain T cells capable of recognizing the specific tumor antigen expressed by the melanoma. Melanoma cells may downregulate expression of tumor antigens if the protein is not required for tumor cell viability. If the melanoma cell cannot downregulate the protein antigen, it can downregulate expression of HLA molecules responsible for presentation of the peptide antigen. The melanoma itself can acquire an immunosuppressive phenotype by loss of IFNγ/JAK/STAT signaling or by producing inhibitory cytokines such as IL6 or IL1β. The tumor microenvironment can be immunosuppressive due to regulatory T cells, suppressive macrophages, or myeloid-derived suppressive T cells. Given these mechanisms of acquired or native resistance, it is not surprising that once a patient develops resistance to checkpoint inhibitor treatment, even after an initial response, retreatment with checkpoint inhibitor therapy is usually less successful.
Experience with single-agent ipilimumab indicated that retreatment with ipilimumab could result in tumor responses ranging from 12% to 23%.10–12 Among patients treated with single-agent anti-PD1, retreatment with anti-PD1 or ipi/nivo resulted in objective responses in 15% and 25% of patients, respectively.13 Recently, Olson22 and colleagues reported that in patients who had previously progressed on anti-PD1/PDL1 therapy, treatment with ipilimumab/pembrolizumab was associated with a 29% response rate. There is little published experience in reinduction with ipi/nivo among patients previously treated with ipi/nivo. Hepner et al23 described 47 patients who received ipi/nivo reinduction after progressing from prior ipi/nivo. Their cohort was slightly different than ours in that their patients all had experienced at least stable disease on induction ipi/nivo, and 15% of their patients were reinduced either with ipi alone or an attenuated ipi/anti-PD1 schedule. Despite these differences, the ORR and median PFS to reinduction were 26% and 5 months, similar to what we observed. Reoccurrence of the same irAEs was seen at reinduction in 40% of their patients.
In assessing the benefits of reinduction with ipi/nivo at least 6 months after completion of the first course of ipi/nivo, we found that 23% of patients achieved a CR or PR after reinduction. This is much lower than the BOR rate to the first cycle of ipi/nivo but very similar to the BOR rate seen in patients initially treated with either single agent ipilimumab or single agent anti-PD1 and then reinduced with the same agent, as noted previously. Objective response to the initial course of ipi/nivo was not associated with response to reinduction. The median TTF was only 5.3 months after reinduction, and in 85% of patients, responses to reinduction with ipi/nivo were shorter (by a median of 12 months) than the duration of response to the first cycle. Among the five patients with CR/PR to reinduction ipi/nivo, the median TTF was 17.3 months, although two patients were censored for treatment failure at the time of data analysis. After reinduction, the overall survival after 1 year and 2 years was 40% and 19%, respectively.
The irAEs associated with reinduction using ipi/nivo required immunosuppression in 58% of the patients and 31% of patients experienced a new irAE that had not been experienced during the first course. In two of these patients, the new irAE was irreversible (hypopituitarism and type I diabetes).
Overall, the risks and benefits of reinduction with ipi/nivo are far less favorable than the risks and benefits to the initial course of ipi/nivo and resemble the risks and benefits of chemotherapy treatment for many malignancies: low response rates (23%), few durable responses, high proportion of significant toxicity, and no clear evidence of prolonged survival. The objective response rate seen after reinduction with ipi/nivo in our cohort was similar to objective response rates seen in other studies after reinduction with either ipilimumab alone or anti-PD1 alone.
Going forward, we need to understand resistance mechanisms more fully and to ascertain whether any of them can be reversed or prevented. If resistance mechanisms are not reversible, we need new treatments that exploit different mechanisms of action. We should not anticipate the same high rate of object responses on ipi/nivo reinduction that we see with initial treatment with ipi/nivo, emphasizing the importance of clinical trials testing novel approaches for immunotherapy-resistant melanoma. In the meantime, in patients requiring reinduction therapy after ipi/nivo, it is reasonable to speculate from these data that we might decrease toxicity and achieve similar objective response rates using single-agent checkpoint inhibitors for reinduction.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. We will make available a deidentified version of an Excel datasheet containing the extracted data.
Ethics statements
Patient consent for publication
Ethics approval
This retrospective analysis was approved by the Memorial Sloan Kettering Cancer Center institutional review board.
References
Footnotes
Twitter @DrBetofMDPhD
Contributors PC: original concept, data acquisition, and manuscript generation. VSJ: radiographic review and RECIST measurements. ABW: data analysis. KSP: data analysis and biostatistics. All coauthors reviewed the data and contributed to editing the manuscript.
Funding This work was funded in part by the Marie-Josée and Henry R. Kravis Center for Molecular Oncology and the National Cancer Institute Cancer Center Core Grant No. P30-CA008748. Some patients were treated on clinical trials funded in part by Bristol-Myers Squibb, the Ludwig Center for Cancer Research, or the Parker Institute for Cancer Immunotherapy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.