Article Text

Abstract
Background Following the extensive use of immunosuppressive drugs in the clinic, immunosuppression-associated side effects have received increasing attention. Epstein-Barr virus (EBV) reactivation and related lymphoproliferative diseases (LPD) are the lethal complications observed after allogeneic hematopoietic cell transplantation (alloHCT). While studies generally suggest an association between immunosuppressants and EBV reactivation, the effects of specific immunosuppressive drugs and which T-cell subsets mediate these correlations are unclear. Vδ2+ T cells are correlated with EBV reactivation after alloHCT. Researchers have not determined whether Vδ2+ T-cell activities are affected by immunosuppressants and thereby facilitate EBV reactivation and related LPD.
Methods A clinical cohort study of 170 patients with hematopoietic malignancies who received haploidentical hematopoietic cell transplantation (haploHCT) was performed to investigate whether the early cessation of mycophenolate mofetil (MMF) decreases EBV reactivation and related LPD and to determine whether this change is associated with the recovery of Vδ2 + T cells after transplantation. The effects of MMF on the expansion and anti-EBV capacity of Vδ2+ T cells were detected in vitro and in an immunodeficient mouse model.
Results A reduction in the course of MMF significantly improved the recovery of Vδ2+ T cells from 30 to 90 days after haploHCT (p=0.002, p=0.042 and p=0.035, respectively), accompanied by a significant decrease in EBV reactivation (from 26% to 13%, p=0.033) and EBV-LPD (from 10.6% to 2.4%, p=0.029). The day-30 Vδ2+ T level remained an independent factor for EBV reactivation in patients with different MMF durations (p=0.007). In the in-vitro experiments, MMF inhibited Vδ2+ T-cell expansion and its cytotoxicity on EBV-transformed malignant cells. Furthermore, the therapeutic and prophylactic effects of adoptively transferred human Vδ2+ T cells were attenuated by the MMF treatment in immunodeficient mice with EBV-LPD.
Conclusions These results elucidated a negative effect of immunosuppressants on the anti-EBV capacity of Vδ2+ T cells. Strategies that appropriately relieve the immunosuppression may improve anti-EBV immunity by increasing the activity of Vδ2+ T cells after alloHCT.
- hematology
- immunology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Immunosuppressive agents have been widely used during the process of transplantation or treatment of malignant and autoimmune diseases over the past several decades.1–3 As emerging evidence supports the clinical efficacy of immunosuppressive therapy, the immunosuppressant-related side effects have received increasing attention. Viral infections and related diseases are the life-threatening complications observed after treatment with immunosuppressive medications; the underlying mechanisms have not been elucidated. Epstein-Barr virus (EBV) reactivation and related lymphoproliferative diseases (EBV-LPD) with high mortality rates are frequently reported after solid organ and hematopoietic transplantation.4–7 Among solid organ transplant recipients in Europe and the USA, over 80% of recipients with post-transplantation LPD presented with an EBV infection.8 9 Among the recipients who underwent allogeneic hematopoietic cell transplantation (HCT), the 3-year cumulative incidence of total EBV-associated diseases was approximately 15.6% and the 3-year overall survival rate was 37.3% in patients with EBV-LPD.10 Studies have not conclusively determined whether a direct link between immunosuppressive drugs routinely used in transplantation and EBV reactivation exists and the intrinsic mechanisms underlying this association. Answers to these questions are urgently needed and important for the clinical prophylaxis of EBV reactivation and its related malignancies in the scenario of HCT.
The administration of antithymocyte globulin (ATG) was a risk factor for EBV-related complications following HCT in a previous study.11 Christopeit et al reported an association between a high serum cyclosporine A (CsA) level and EBV DNAemia after allogeneic HCT.12 Nevertheless, ATG and CsA are generally postulated to act by targeting T cells, but the specific T-cell subset involved in immunosuppression-related EBV reactivation has not been clarified. Mycophenolate mofetil (MMF) is another common immunosuppressant used in the setting of transplantation. In the context of solid organ transplantation, MMF treatment was reported to be associated with a lower risk of EBV viremia/disease, whereas other reported opposite results.13–15 The correlation between MMF and EBV-LPD after HCT currently remains unclear. The Beijing protocol of HCT, which was pioneered in China, has been one of the main approaches for haploidentical HCT (haploHCT) and has been widely incorporated into clinical practice in Asia and some countries in Europe.16–19 MMF, along with ATG and CsA, is always used for graft-versus-host disease (GVHD) prophylaxis in the Beijing protocol. In contrast to the fundamental requirements for ATG and CsA treatments, the administration of MMF may be relatively flexible to balance the effect of immunosuppression and risk of infection. Because MMF selectively suppresses the proliferation of T and B lymphocytes,20 investigations of effector T-cell subsets based on the change in MMF administration may reveal a general mechanism that correlates immunosuppressant use to EBV reactivation.
Functions of adaptive T cells related to EBV reactivation have been well recognized. However, the reconstitution of EBV-specific CD8+ T cells is generally undetectable at early stages after haploHCT when viral reactivation occurs. Thus, the roles of other effector T cells in anti-EBV immunity must be explored. A special T-cell subpopulation, γδ T cells, has attracted increasing attentions due to its potent anti-infection and antitumor capacities.21–25 Indeed, Vδ2+ T cells are cytotoxic to the EBV-target cells in vitro and in mouse models.26 Regarding the clinical effect, we previously reported that the impaired early recovery of Vδ2+ T cells was significantly associated with the occurrence of EBV reactivation after haploHCT.27 According to our subsequent study, peripheral Vδ2+ T cells from haploHCT recipients were not expanded on stimulation with bisphosphonate.28 Whether the decrease in Vδ2+ T-cell activity was attributed to the administration of immunosuppressants remained undetermined.
In our present study, we investigate whether reliving the suppressive effects of MMF leads to a decrease in EBV reactivation and EBV-LPD, and whether these changes are associated with an improvement in Vδ2+ T-cell recovery in a clinical cohort after allogeneic HCT. The effects of MMF on the expansion and anti-EBV capacity of Vδ2+ T cells were also assessed in vitro and in mouse model.
Materials and methods
Design of the clinical study
We previously registered a clinical trial (ChiCTR-COC-16008052) that aimed to prospectively survey the recovery characteristics of γδ T-cell subsets and their associations with EBV reactivation after haploHCT from March 2016 to March 2018. The inclusion criteria were described in a previous study.27 MMF was administered orally at a dose of 1 g/day for GVHD prophylaxis to all transplant recipients. During the execution period of this trial, the protocol of MMF administration for GVHD prophylaxis was changed in our institution. Prior to March 2017, MMF was withdrawn at 45–60 days after transplant (defined as the “longer” duration); since March 2017, MMF was withdrawn by engraftment (defined as the “shorter” duration). At least 160 patients are required to evaluate the effects of different MMF durations on the recovery of γδ T-cell subsets and the occurrence of EBV reactivation after haploHCT, based on the calculation obtained using PASS V.11.0 Sample Size software (NCSS, USA). Accordingly, 170 patients who consented to join the current study were enrolled, with 85 consecutive patients each in the longer (from June to September 2016) and shorter (from September to December 2017) MMF groups.
All recipients were infused with grafts combined with granulocyte colony-stimulating factor-primed peripheral blood and unmanipulated bone marrow products. The transplant procedures, conditioning regimen including busulfan, cyclophosphamide, and ATG (rabbit ATG, Imtix Sangstat, Lyon, France), and GVHD prophylaxis and treatment were described previously.29 Patients in both groups all received 10 mg/kg ATG prior to transplantation. The whole blood CsA concentration of every patients was monitored weekly for at least 6 months, and the dosage was adjusted to maintain a trough blood concentration of 150–250 ng/mL. All recipients and their donors have signed consent forms.
Immunophenotyping
At days 30, 60, and 90 after haploHCT, peripheral blood samples were collected from recipients and stained with the fluorochrome-labeled antibodies: including anti-CD3, anti-TCRγδ, and anti-TCRVδ2 purchased from BioLegend (USA); anti-TCRαβ, anti-CD4, and anti-CD8 bought from Becton Dickinson (BD, USA); anti-TCRVδ1 from Miltenyi Biotec (Germany). Polychromatic flow cytometric analyses were performed on a BD LSRFortessaTM Cell Analyzer and further analyzed using BD FACSDivaTM software.
Diagnosis of viral infection and EBV-LPD
The viral-DNA loads in the peripheral blood were detected by real-time quantitative PCR. All recipients and donors were tested negative for EBV and cytomegalovirus (CMV) DNA before transplantation. Recipients were monitored weekly until day 100 after transplantation. Patients with EBV-DNA load >1000 copies/mL in the peripheral blood on more than two consecutive occasions were diagnosed as EBV reactivation. CMV DNA in the peripheral blood of recipients was routinely monitored similar with EBV DNA, as described above. Diagnosis of probable EBV-LPD was established when the EBV DNAemia was associated with lymphadenopathy, hepatosplenomegaly, or any other organ involvement on CT and ultrasound findings, without tissue biopsy and in the absence of other documented causes.
Ex-vivo expansion of Vδ2+ T cells upon immunosuppressant treatment
Peripheral blood mononuclear cells (PBMCs) were isolated from healthy donors using standard Ficoll-Hypaque density gradient centrifugation. Pamidronate was used to expand Vδ2+ T cells as previously described.26 30 A therapeutically relevant concentration of mycophenolic acid (MPA, 10 µM, Sigma-Aldrich, USA) or CsA (1 µg/mL, Novartis Pharma AG, Basel, Switzerland) was used to treat cells at the same time. Recombinant human interleukin-2 (Stemimmune LLC, USA) was added to a final concentration of 50 ng/mL every third day from day 3. At 5 and 10 days of culture, cells were detected with the fluorochrome-labeled anti-CD3 and anti-TCRVδ2 antibodies (BioLegend, USA).
For cell proliferation assay, PBMCs were labeled with 1 µM of carboxy fluorescein succinimidyl ester (CFSE, BioLegend). For cell activation assay, cells were stained with fluorochrome-labeled anti-CD25 and anti-HLA-DR antibodies (BioLegend). For detection of intracellular cytokine, cells were stained with anti-IFN-γ (BD Biosciences, USA) and anti-TNF-α antibodies (BioLegend) after stimulation with 1× Cell Stimulation Cocktail (500×, eBioscience, USA).
Assay of the effect of immunosuppressants on anti-EBV-LCLs capacity of Vδ2+ T cells
Pamidronate-expanded Vδ2+ T cells were isolated using the anti-TCR γ/δ MicroBead Kit. The purified Vδ2 cells (purity >95%) were treated with MPA (10 µM) and CsA (1 µg/mL, USA) for 48 hours and were cocultured with EBV-transformed B-lymphoblastoid cell lines (EBV-LCLs) at 5:1 ratio for additional 5 hours. Then, cells were harvested and stained with the fluorochrome-labeled anti-CD3, anti-TCRVδ2, and anti-CD19, and 7-AAD Viability Staining Solution (BioLegend).
Evaluation of the impact of MMF on the therapeutic and prophylactic effects of human Vδ2+ T cells in mice with EBV-related disease
All experiments in mice were performed in compliance with the guidelines and were approved by the Ethical Committee on the Use of Live Animals at Peking University People’s Hospital. The severe immunodeficient NOD-Prkdcscid Il2rgtm1/Vst (NPG) mice were purchased from Beijing Vitalstar Biotechnology (China). Female NPG mice of 6–7 weeks old were randomly divided into four groups: EBV-LCL+PBS, EBV-LCL+Vδ2+ T cells, MMF+EBV-LCL+Vδ2+ T cells, and CsA +EBV-LCL+Vδ2+ T cells (n=5 per group). Specifically, two groups of mice were intraperitoneally (i.p.) injected with clinical relevant concentrations of MMF (40 mg/kg/day, Roche Pharmaceuticals, Palo Alto, USA) and CsA (5 mg/kg/day), respectively. One week following the treatment with immunosurppressive drugs, EBV-LCLs were subcutaneously inoculated into all of the mice (4×105/mouse). Three weeks later than EBV-LCL inoculation, two groups with immunosuppressants and the third group were adoptively transferred with the pamidronate-expanded Vδ2+ T cells (4×106/mouse) intravenously at the indicated time. The remaining one group of mice was injected with PBS as the control. To evaluate the impacts of MMF and CsA on the cytotoxicity of Vδ2+ T cells targeting EBV-LCLs, the subcutaneous tumors (EBV-LPD) derived from EBV-LCLs were measured by caliper and statistically analyzed every week.
To evaluate the effects of different dosages of MMF on mice with EBV-LPD and received prophylactic Vδ2+ T cells, NPG mice were i.p. injected with 10, 20, and 40 mg/kg/day of MMF, respectively. EBV-LCLs (2×105/mouse) and the ex-vivo expanded human Vδ2+ T cells (2×106/mouse) were intravenously injected at the indicated time. Mice with hind-leg paralysis were counted as death and sacrificed. Considering its own antitumor efficacy, Pamidronate was not used during the experiment assessing the anti-EBV-LPD effects after Vδ2+ T cells were expanded ex vivo.
Statistical analysis
Differences in age, mononuclear cells (MNCs) and CD34+ cells in grafts, MMF durations, and cell counts of T-cell subpopulations at different time points between the groups were analyzed using the Mann-Whitney U test. Differences in gender, type of primary disease, and incidences of acute GVHD and viral infections were analyzed using the χ2 test. Cox regression analysis was performed to distinguish the independent association of T-subsets recoveries with EBV reactivation after haploHCT. Statistical significance was defined as p≤0.05, based on a two-tailed test. All calculations were performed using SPSS V.22.0 statistical software (SPSS).
Results
Reducing the duration of prophylactic MMF improved the recovery of peripheral Vδ2+ T cells after haploHCT
As described in the Methods section, two cohorts treated with different durations of MMF after haploHCT were included in this study. The clinical characteristics of the patients are summarized in table 1. Significant differences in age, the proportion of gender, disease types, the degrees of HLA mismatch, numbers of MNCs and CD34+ cells in grafts, and the proportions of donor/recipient pairs in EBV serology were not observed between the two MMF groups (p values are all >0.05) in the current study. The median duration of MMF in the shorter term group was 25 days (15–36 days), whereas the duration was 41 days (24–69 days) in the longer term group (p<0.001). Procedures for donor priming and graft harvesting, conditioning regimens, usage of ATG, the protocols for the administration of CsA and methotrexate in the GVHD prophylaxis regimen were the same for all included patients.
Clinical characteristics
Total T cells and various T-cell subsets, including CD3, CD4, CD8, CD8+αβ T, γδ T, Vδ1+, and Vδ2+ T cells, were monitored with flow cytometry at 30, 60, and 90 days after transplantation. The numbers of Vδ1+ T cells were not significantly affected by changing the MMF duration at different time points. Total T cells and other detected T-cell subpopulations recovered significantly faster at day 30 in the shorter MMF group than the longer MMF group (p values were all <0.01, table 2). Notably, the numbers of Vδ2+ T cells, but not other T-cell subsets, in the shorter MMF group were consistently higher than in the longer group at 60 and 90 days post-HCT (p=0.042 and p=0.035, table 2). Based on these results, recovery of Vδ2+ T cells at the early stage after haploHCT improved after the immunosuppression mediated by MMF was relieved.
Recoveries of T-lymphocyte subpopulations after haploidentical hematopoietic cell transplantation, ×103 cells/mL (median, range)
Early cessation of MMF decreased the incidence of EBV reactivation and related LPD after haploHCT
Next, the incidences of EBV and CMV reactivation, EBV-LPD, and aGVHD were compared between the groups. As shown in table 3, early cessation of MMF was associated with a decrease in the occurrence of EBV reactivation (from 26% to 13%, p=0.033). The incidence of EBV-LPD in patients who received shorter MMF prophylaxis (2/85, 2.4%) was also significantly decreased compared with the longer term group (9/85, 10.6%, p=0.029). In contrast, the incidence of CMV reactivation was comparable between the two cohorts (p=0.470). The time to the first CMV reactivation in patients with a shorter duration of MMF treatment was significantly prolonged compared with the longer term group (38 days vs 34 days, p=0.003). However, the time to the first EBV reactivation was not significantly affected by the different MMF durations (47 vs 44 days, p=0.541). Notably, the incidences of grades I–IV or grades III–IV aGVHD, and the onset time of aGVHD were all comparable (p=0.535, 0.103, and 0.548 respectively), regardless of the MMF duration. The actual 1-year survival rate of patients who received the shorter term MMF was superior to the patients receiving the longer term MMF (85.9% vs 68.2%, p=0.006, table 3). Thus, a reduction in the course of MMF facilitates a decrease in EBV reactivation and related LPD, but it does not increase the risk of GVHD after hematopoietic transplantation.
Major outcomes of haploidentical hematopoietic cell transplantation recipients with different mycophenolate mofetil (MMF) durations
In the current study, totally 33 patients experienced EBV reactivation after transplantation. All patients received antiviral drugs, such as acyclovir. Seventeen patients were treated with rituximab and five patients received rituximab plus EBV-CTL treatments. The other 11 patients did not receive rituximab because of the cost. Thirty-one patients achieved a clearance of EBV DNAemia. Among the patients experienced EBV reactivation, 11 developed EBV-LPD and 7 of whom achieved complete remission after treatments (online supplementary table 1).
Supplemental material
The day-30 number of Vδ2+ T cells remained an independent factor for EBV reactivation in haploHCT recipients with different MMF durations
In the current study, the day-30 recoveries of T-cell subsets were all improved by reducing the course of MMF, and the median time to onset of EBV reactivation was 44 (22-82) and 47 (27-86) days, respectively, in the longer and shorter term MMF groups after HCT. Although the numbers of total CD3+ and Vδ2+ T cells observed at day 60, and Vδ2+ T cells observed at day 90 after HCT in the shorter MMF group were higher than the longer MMF group, only four patients experienced EBV reactivation after 60 days and no EBV reactivation occurred after 90 days in the whole cohort. Accordingly, the decreased numbers of T cell subsets observed on day 30 might be a cause of EBV reactivation and a decrease in the numbers of Vδ2+ T cells on days 60 and 90 might be a subsequent event. Therefore, a Cox regression analysis was performed to detect the independent factors among the numbers of T cell subsets observed on day 30. As shown in online supplementary table 2, only the day-30 number of Vδ2+ T cells, but not the numbers of CD3+, CD4+, CD8+, CD8+αβ T, total γδ T, and Vδ1+ T cells, was a significant factor correlated with EBV reactivation (HR=0.347, p=0.007) in the whole cohort with different MMF durations after haploHCT. A time-dependent Landmark analysis also showed that lower recovery (<8.8 vs ≥8.8×103 cells/mL) of the number of Vδ2+ T cells on day 30 was correlated with a higher cumulative incidence of EBV reactivation after HCT (p=0.002) (online supplementary figure 1). Based on this finding, the effect of MMF on the EBV reactivation critically correlates with the number of Vδ2+ T cells observed at the early stage after allogeneic HCT.
MMF inhibited the expansion and anti-EBV-LCL capacity of Vδ2+ T cells
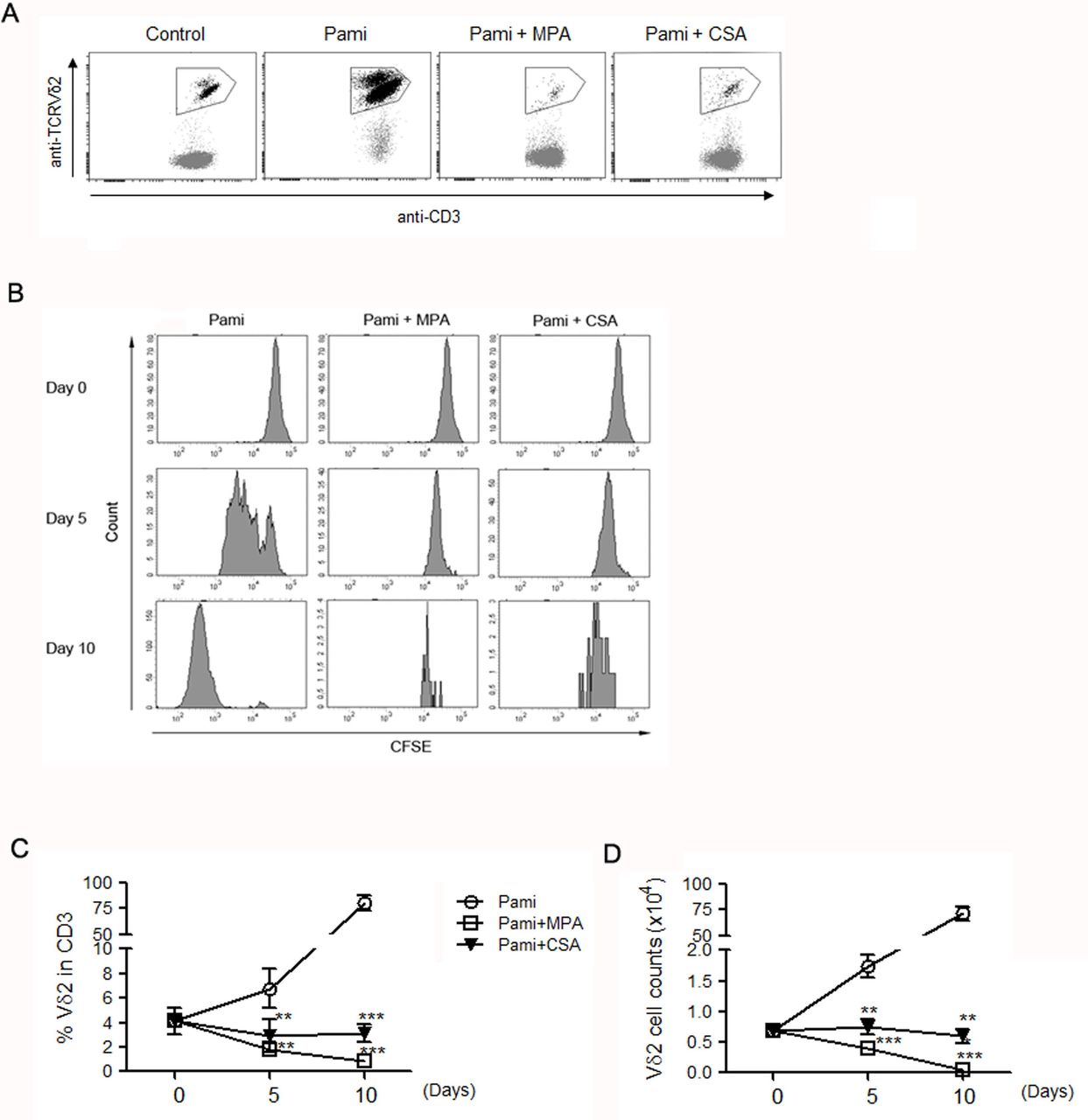
PBMCs isolated from healthy donors were treated with the active form of MMF, MPA, and CsA to explore the effects of immunosuppressants on the activity of Vδ2+ T cells. Representative dot plots of Vδ2+ T cells detected using flow cytometry are shown in figure 1A. Prelabeling with CFSE indicated the dynamic proliferation of Vδ2+ T cells in response to pamidronate stimulation, which was blocked by the treatment with MPA and CsA (figure 1B). Indeed, 75% of CD3+ cells were TCR-Vδ2 positive after 10 days of stimulation by pamidronate (figure 1C). The absolute number of Vδ2+ T cells increased 100 fold (from 7×103 to 7×105, figure 1D). However, Vδ2+ T cell expansion was completely inhibited by treatment with MPA and CsA (p values are all <0.01), as the percentages and absolute numbers were comparable or even lower than the baseline values (figure 1C,D).
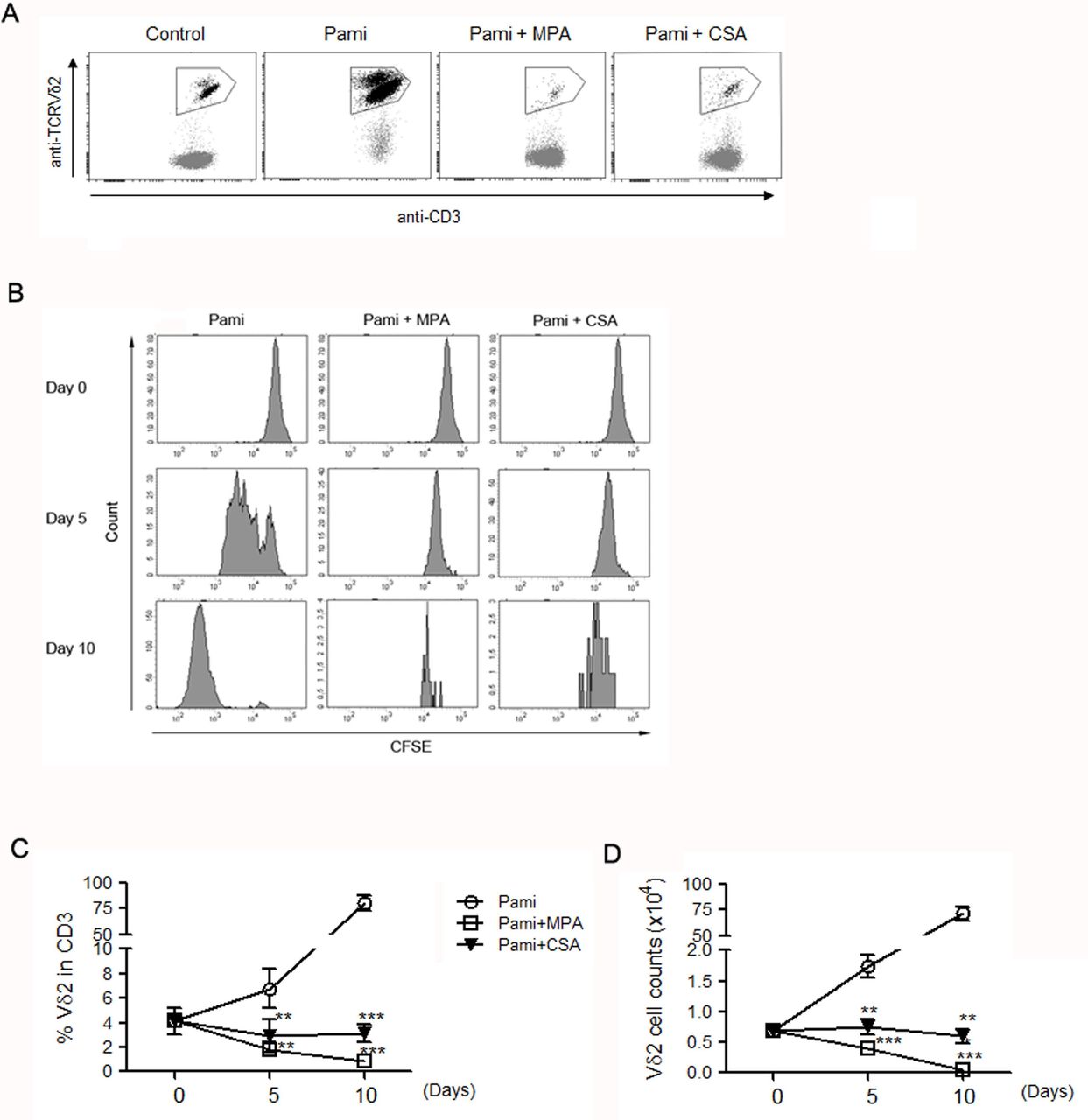
Effects of mycophenolicacid (MPA) and cyclosporine A (CsA) on the expansion of Vδ2+ T cells in peripheral blood mononuclear cells isolated from healthy donors were stimulated by pamidronate for 5 and 10 days, without or with treatment of MPA and CsA. (A) Representative dot plots of Vδ2+ T cells detected at 10 days after culture. (B) The intensity of carboxy fluorescein succinimidyl ester (CFSE), and (C) the percentage and (D) absolute number of Vδ2+ T cells were, respectively, detected by flow cytometry. ** p<0.01, *** p<0.001, n=4.
Different combinations of CD27 and CD45RO expression allowed us to identify the differentiation profile of Vδ2+ T cells, including naïve (N, CD27+CD45RO–), central memory (CM, CD45RO+CD27+), effector memory (EM, CD45RO+CD27–), and terminal differentiation (TD, CD45RO–CD27–) statuses. As shown in figure 2A, the proportion of the CM subset of Vδ2+ T cells was significantly increased after pamidronate stimulation (p=0.04) and was attenuated by the MPA and CsA treatments (p=0.004 and p=0.001, respectively). However, the proportion of the N subset was decreased in the pamidronate-expanded Vδ2+ T cells and returned to the baseline percentage at 10 days after CsA treatment (p values were all <0.01, figure 2A). The expression of HLA-DR (figure 2B) indicating T-cell activation, the cytotoxic receptor NKG2D (figure 2C), and cytotoxic cytokine interferon-γ (IFN-γ) (figure 2D) was significantly decreased in Vδ2+ T cells in the presence of MPA and CsA (p values are shown on the graphs).

Effects of mycophenolic acid (MPA) and cyclosporine A (CsA) on the activation and anti-Epstein-Barr virus (EBV)-transformed B-lymphoblastoid cell lines (LCLs) capacity of Vδ2+ T cells. (A) The differentiation profile of Vδ2+ T cell fractions in different groups. CM, central memory; EM, effector memory; N, naïve; TD, terminal differentiation. The expression of (B) HLA-DR, (C) NKG2D, and (D) interferon γ (IFN-γ) in Vδ2+ T cells was compared among different groups. (E) Assay of Vδ2+ T cell cytotoxicity on EBV-LCLs. P values are shown on the graphs; otherwise, *** p<0.001, n=4.
The effects of MMF on patients’ Vδ2+ T cells were investigated. PBMCs were isolated from selected recipients 90–180 days after haploHCT. As shown in online supplementary figure 2, the MPA treatment significantly decreased the expressions of IFN-γ and TNF-α in primary Vδ2+ T cells from HCT patients (p values all<0.05, n=6).
Representative images of generation and characterization of ex-vivo expanded Vδ2+ T cells used in the following analyses are shown in online supplementary figure 3. The flow cytometry analysis showed that the majority of cultured cells were Vδ2+ T cells. More than 95% of Vδ2+ T cells were NKG2D and IFN-γ positive, indicating the potent effective function of expanded Vδ2+ T cells. Next, the expanded Vδ2+ T cells were pretreated with MPA, CSA, or the combination of the two, and then cocultured with EBV-LCLs to determine the effect of immunosuppressants on the EBV-LCL cytotoxicity of Vδ2+ T cells. As shown in figure 2E, untreated Vδ2+ T cells increased the proportion of 7-AAD-positive EBV-LCLs from 2% to 27%. In contrast, the viability of EBV-LCLs was partially restored after coculture with MPA-treated and CsA-treated Vδ2+ T cells as the percentages of 7-AAD-positive EBV-LCLs decreased from 27% to 11% and 21%, respectively (p<0.001 and p=0.012). The combination of MPA and CsA further impaired the cytotoxic effects of CsA-treated Vδ2+ T cells on EBV-LCLs (p<0.001). These results highlighted a critical role for MMF in suppressing the function of Vδ2+ T cells against EBV target cells. The EBV specificity of Vδ2+ T cells was also detected. As shown in online supplementary figure 4, the expression of CD107a, IFN-γ, and TNF-α in Vδ2+ T cells was significantly increased on EBV-LCL stimulation. These results indicate the specific response of Vδ2+ T cells toward the EBV challenge.
MMF attenuated the therapeutic and prophylactic effects of Vδ2+ T cells on mice with EBV-LPD
Next, the effects of immunosuppressants on the anti-EBV-LPD activity of Vδ2+ T cells were investigated in immunodeficient NPG mice. The experimental protocol is presented in figure 3A. All mice were inoculated with human EBV-LCLs; two groups of them were injected with MMF or CsA beginning 1 week before the EBV-LCL inoculation. The average volumes of subcutaneous tumors derived from EBV-LCLs (EBV-LPD) were comparable (~120 mm3) among the groups at 3 weeks after inoculation. The purified (>95%) pamidronate-expanded Vδ2+ T cells were adoptively transferred at 3, 4, 5, and 6 weeks. As shown in figure 3B, Vδ2+ T cells were detectable in the peripheral blood of EBV-LPD mice from 5 to 7 weeks after the injection, which were present at extremely low percentages in the MMF-treated and CSA-treated groups. Consistent with these findings, the Vδ2+ T cells infusion tended to reduce the tumor volume in the EBV-LPD mice at 5 weeks (p=0.069), and the changes were more significant at 6 and 7 weeks compared with the control group (p=0.008 and 0.010, figure 3c). However, in EBV-LPD mice that were persistently treated with MMF or CsA, the infusion of Vδ2+ T cells did not decrease the tumor volumes compared with the controls over the same time course (p values>0.5). The therapeutic effect of Vδ2+ T cells was significantly attenuated by the treatment with MMF at 7 weeks (p=0.036). A similar trend was observed in the CsA-treated group, although the p value was close to the threshold for statistical significance (p=0.094, figure 3C). The macroscopic appearance of the subcutaneous tumors isolated from different groups at 7 weeks is shown in figure 3D. Taken together, MMF abolishes the therapeutic effect of Vδ2+ T cells on EBV-LPD in mice.
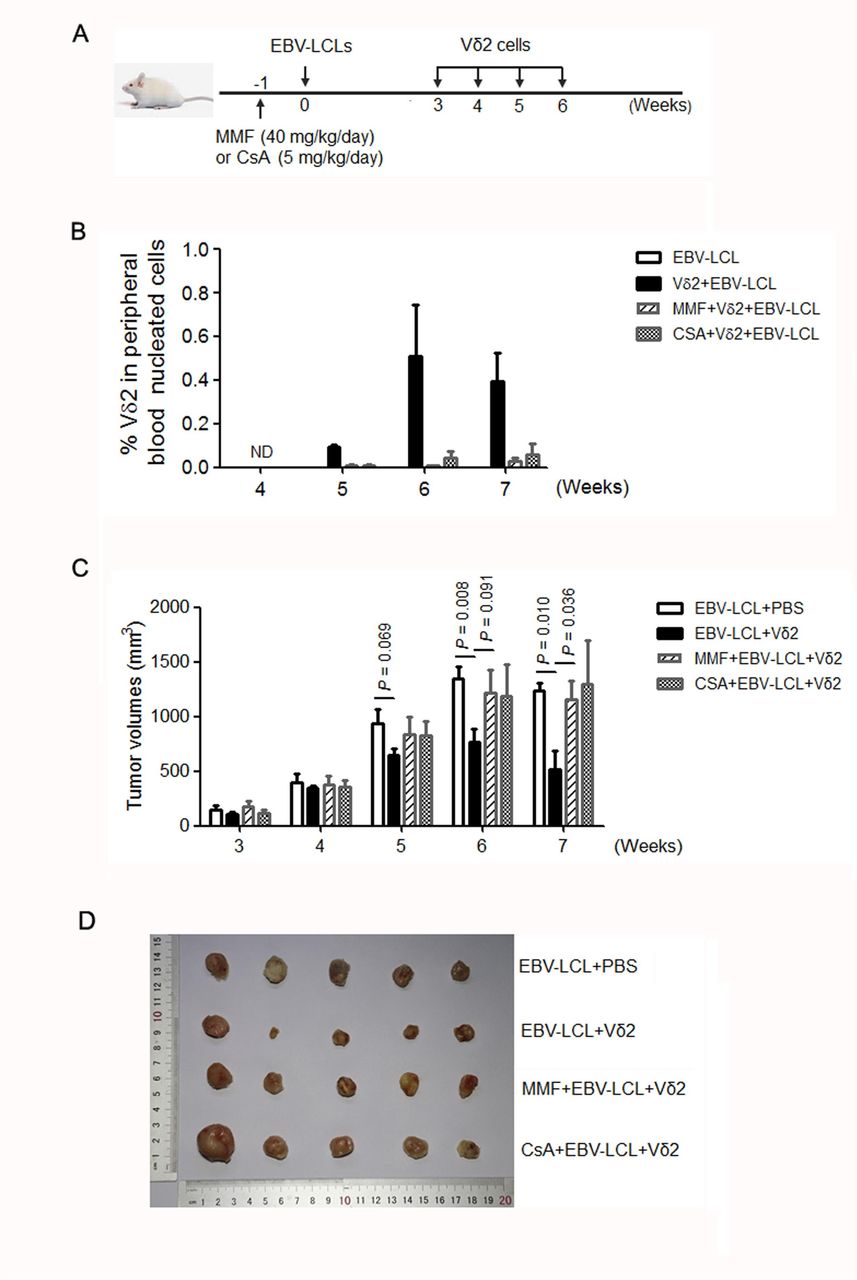
Mycophenolate mofetil (MMF) inhibited the cytotoxic effect of Vδ2+ T cells on Epstein-Barr virus (EBV)-related lymphoproliferative diseases (LPD) in immunodeficient mice. (A) Protocol for evaluating the effects of immunosuppressants on the anti-EBV activity of Vδ2+ T cells in NPG immunodeficient mice. (B) The average proportions of Vδ2+ T cells in the peripheral blood nucleated cells in different groups of mice. ND, not detected. (C) The average volumes of subcutaneous tumors from EBV-LPD mice in different groups at indicated time courses. The statistical significances are shown on the graph; otherwise, p values>0.5. (D) The macroscopic appearance of the tumors isolated from EBV-LPD mice in different groups at 7 weeks. CsA, cyclosporine A; LCL, lymphoblastoid cell lines.
Next, we explored the effects of different dosages of MMF on the prophylactic effect of Vδ2+ T cells on preventing the development of tumors from EBV-LCLs and the rescue efficacy following the cessation of MMF. NPG mice were injected with 10, 20, or 40 mg/kg/day of MMF beginning on day −7 and the treatment stopped on day 30. EBV-LCLs were injected on day 0. Vδ2+ T cells were transferred on days 0, 7, 14 and 21 for prophylaxis, and on day 32 for salvage treatment. All control mice injected with EBV-LCLs and PBS died from day 25 to day 36, whereas all mice injected with Vδ2+ T cells without the immunosuppressant survived for 7 weeks, the end of the observation (p=0.003, figure 4A). Although one mouse died in the group treated with 10 mg/kg/day of MMF on day 29, the survival rate was significantly higher than the control group (p=0.025, figure 4B). In contrast, groups treated with 20 (2 mice died on day 28 and day 31) and 40 (2 mice died on day 27 and day 30) mg/kg/day of MMF lost the superior survival compared with the control group (p=0.129 and 0.149, respectively, figure 4C,D). The remaining mice in the MMF+Vδ2 groups were injected with additional Vδ2+ T cells after MMF was withdrawn, which was the same treatment received by mice in the Vδ2 only group. Consistently, the same survival rate was observed among the groups at the later time course. These results suggest that MMF impairs the protective effect of Vδ2+ T cells on mice treated with lethal EBV-LCLs, probably in a dosage-dependent manner. This negative effect is rescued by withdrawing the immunosuppressant and transferring additional Vδ2+ T cells.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of different dosages of mycophenolate mofetil (MMF) on mouse survival in the presence of Epstein-Barr virus (EBV)-transformed B-lymphoblastoid cell lines (LCLs) and Vδ2+ T cells. All mice were injected with EBV-LCLs at the beginning. The survival rates of (A) mice treated with Vδ2+ T cells, (B) 10 mg/kg/day of MMF and Vδ2+ T cells, (C) 20 mg/kg/day of MMF and Vδ2+ T cells, and (D) 40 mg/kg/day of MMF and Vδ2+ T cells were compared with the control group, respectively. The statistical significances are shown on the graphs, n=5.
Discussion
Opportunistic EBV reactivation and its related lethal diseases usually occur in immunocompromised hosts, such as patients who have received a transplantation.31 32 Although immunosuppressive drugs are conventionally recognized as a risk factor for viral infections, few studies have reported the specific drugs that directly correlated with EBV reactivation and related LPD in the context of allogeneic HCT. The administration of ATG correlated with immune recovery and the overall outcome of alloHCT in a previous study.33 As shown in our previous study, the administration of 10 mg/kg ATG in conditioning regimen increased the occurrence of EBV reactivation in haploHCT recipients compared with 6 mg/kg ATG, and was associated with the recovery of CD4/CD8 double-negative T cells (DNTs).34 Because γδ T cells are a major subpopulation of DNTs, our subsequent study highlighted an inverse correlation of early Vδ2+ T cell recovery with EBV reactivation after haploHCT.28 To date, no studies have dissected the effects of different immunosuppressants on T cell subsets and identified which T-cell subsets mediate the correlation of immunosuppressive drugs with EBV reactivation. In the present study, our clinical study revealed that the recovery levels of Vδ2+ T cells continuously improved from 30 to 90 days after the course of routinely used immunosuppressant MMF was reduced, accompanied by significant decreases in EBV reactivation and related LPD in recipients who underwent haploHCT. These findings are consistent with a recent published meta-analysis showing that an increase in the number of γδ T cells after alloHCT was associated with better outcomes.35 The inhibitory effects of MMF on the expansion and anti-EBV-LCL capacity of Vδ2+ T cells were further confirmed in vitro and in a mouse model. Withdrawal of the drug and the transfer of additional Vδ2+ T cells overcame the immunosuppression and improved the survival of mice. Notably, neither the adoptive transfer of Vδ2+ T cells into mice nor a reduction in the duration of MMF in patients after hematopoietic transplantation increased the risk of aGVHD. These results strengthen the translational relevance of Vδ2+ T cells that link the immunosuppression with opportunistic infections and suggest a potential option for the treatment of EBV-related complications after allogeneic HCT.
In terms of the effect of MMF on other viral infections following transplantation, Hamad et al reported a significantly higher 1 year cumulative incidence of CMV viremia in the MMF/CsA group compared with the MTX/CsA group of patients who received related donor myeloablative peripheral blood HCT.36 Another study reported an increased risk of infectious complications following MMF administration after HCT, whereas no specific viral infections were clarified.37 Here, the incidence of EBV reactivation was significantly decreased after the course of prophylactic MMF was reduced in haploHCT recipients. In contrast, the incidence of another major infectious complication after HCT, CMV reactivation, was not significantly affected by the change in the MMF duration in our study. However, the median time to the first CMV reactivation in patients with a shorter MMF treatment was significantly prolonged compared with the longer term MMF group (38 vs 34 days, p=0.003). The correlation between other immunosuppressants and CMV infection after transplantation remains to be studied. Here, we provided clinical evidence of a significant correlation between MMF and EBV reactivation in the context of allogeneic HCT, which may provide a reference for investigations of solid organ transplantation.
Interestingly, the recovery of another γδ T subpopulation, Vδ1+ T cells, was not significantly affected by the change in the MMF duration in our study. Slightly greater numbers of Vδ2-negative γδ T cells were observed in the shorter term MMF group than in the longer term MMF group at 30 days (p=0.045), but not at 60 (p=0.263) and 90 (p=0.445) days (data not shown). Because the major fraction of Vδ2-negative γδ T cells are Vδ1+ T cells in human peripheral blood, we mainly focused Vδ1+ T cells in the current study. Previous studies reported a significant increase in the number of Vδ1+ T cells in patients who experienced CMV reactivation after allogeneic HCT.38 39 Thus, the comparably high incidences (76% and 80%) of CMV reactivation in shorter and longer MMF groups in the present study may neutralize the effect of MMF on the recovery of Vδ2-negative γδ T cells including Vδ1+ T cells.
A recent study showed that the recovery of NK cells was impaired by the long-term administration of MMF after haploHCT. However, that small cohort study did not provide evidence for an effect of different durations of MMF treatment on EBV reactivation.40 In the present study, the numbers of NK (CD3-CD56+) cells were monitored using immunophenotyping, and were comparable between the two MMF groups at 30 (p=0.843) and 60 days (p=0.463) after HCT (data not shown). This observation is distinct with the significant changes in Vδ2+ T cell recovery under the same condition and consistent with the effect of MMF that selectively inhibits T and B lymphocytes. The differential responses of NK and γδ T cells to EBV have been reported.41 Since the major goal of current study is to investigate the effects of MMF on the occurrence of EBV reactivation and related Vδ2+ T cells, we did not distract the focus to further dissect the minor subpopulations of NK cells. Of course, our results do not exclude a potential role for some NK subpopulations in preventing EBV infection after HCT.
Adaptive cytotoxic T cells play an important role in the elimination of EBV-infected cells. However, the reconstitution of EBV-specific CD8+ T cells was rarely detectable in most recipients within the first 3 months after alloHCT.42 Meanwhile, the HLA phenotypes of patients in our large cohort were very complicated; thus, the detection of the HLA-restricted EBV-specific CD8+ T cells in all patients was impractical. Alternatively, we evaluated the levels of CD8+αβ T cells recovery in the current study. Although the recovery of CD8+αβ T cells improved on day 30 by reducing the course MMF, the numbers of CD8+αβ T cells on days 60 and 90 were comparable between the shorter and longer MMF groups. According to the multivariate analyses, the day-30 number of Vδ2+ T cells, but not CD8+αβ T cells, remained an independent factor associated with EBV reactivation in recipients with different MMF durations. These findings implicate Vδ2+ T cells as a key effector subset in anti-EBV immunity at the early stage after allogeneic HCT, which at least partially explains the positive correlation of MMF with EBV reactivation and related LPD.
In summary, MMF significantly attenuated Vδ2+ T cells expansion and anti-EBV-LCL activities. Based on the clinical evidence, Vδ2+ T cell recovery was altered by changing the MMF duration, which was independently correlated with EBV elimination at the early stage after allogeneic HCT. These findings reveal an important Vδ2+ T cells-based mechanism that may generally underlie the associations of immunosuppressive drugs with EBV-related complications. A comprehensive understanding of the effects of immunosuppressants on Vδ2+ T cells and anti-EBV immunity will be conductive to optimizing the EBV-LPD treatment strategy and improving the outcomes of hematopoietic transplantation.
Conclusions
As shown in the present study, longer use of a routine immunosuppressant, MMF, was associated with the decreased recovery of Vδ2+ T cells and increased occurrences of EBV reactivation and EBV-LPD after alloHCT for patients with hematopoietic malignancies. Early Vδ2+ T cells recovery was an independent risk factor for EBV reactivation in these patients. Indeed, MMF significantly inhibited the expansion and cytotoxicity of Vδ2+ T cells toward EBV-transformed malignant cells in vitro. The negative effects of MMF on the therapeutic and prophylactic effects of Vδ2+ T cells were further confirmed in a mouse model with EBV-LPD. These findings reveal an important Vδ2+ T cells-based mechanism that may generally underlie the associations of immunosuppressive drugs with EBV-related complications. A comprehensive understanding of the effects of immunosuppressants on Vδ2+ T cells and anti-EBV immunity will be conductive to optimizing the strategy of EBV-LPD treatment and improving the outcome of hematopoietic transplantation.
Acknowledgments
The authors thank the principal investigators and the skilled teams.
References
Footnotes
JL and HG contributed equally.
Contributors JL designed and performed the research, analyzed data, and wrote the manuscript; HG designed and performed the research, and analyzed data; L-PX and X-DM collected and analyzed data; RL, SL, and NW performed the research; MW and ZW collected the blood samples; Y-JC, YW and X-HZ interpreted data and reviewed the manuscript; and X-JH supervised research and revised the manuscript.
Funding This study is supported by the National Key Research and Development Programme of China (no. 2017YFA0104500), Innovative Research Groups of the National Natural Science Foundation of China (Grant No. 81621001), and National Natural Science Foundation of China (Grant No. 81770191).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the Ethics Committee of Peking University People’s Hospital and was performed in accordance with the Declaration of Helsinki. Informed consent was obtained from each patient.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.